


1Tulane University School of Medicine, New Orleans, LA, USA and 2Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemoon-Gu, Seoul 120-752, Korea. *E-mail: dykim@yuhs.ac
#These authors contributed equally and should be considered as first authors.
Accepted June 21, 2021; Epub ahead of print Jun 23, 2021
Acta Derm Venereol 2021; 101: adv00489.
doi: 10.2340/00015555-3853
Immunotherapy is revolutionizing approaches to cancer treatment. Monoclonal antibodies that inhibit specific immune pathways, such as programmed cell death protein 1 (PD-1) and PD-ligand 1 (PD-L1), are used to boost immune response against cancer cells (1). However, antibodies targeting PD-1/PD-L1 can provoke immune-related adverse events (irAEs), which often manifest as skin changes. Among cutaneous irAEs, approximately 8% are immunobullous in nature, commonly bullous pemphigoid (BP) (2).
The pathogenesis of anti-PD-1/PD-L1-associated BP is not fully understood. BP180, a basement membrane protein, is expressed in some tumour cells, and persistent immune activation induces antibody production against both tumour and normal skin (3). In this context, more serious cutaneous irAEs can be expected in novel cancer immunotherapies boosting anti-PD-1/PD-L1-induced immune responses.We report here a case series of BP associated with combined treatment using anti-PD-1/PD-L1 antibodies and novel agents targeting transforming growth factor (TGF)-β, an immunosuppressive cytokine upregulated in the cancer microenvironment (4, 5).
This study retrospectively reviewed the medical records of 46 BP patients selected based on the following criteria: BP diagnosis based on clinical and histological findings including direct and/or indirect immunofluorescence at Severance Hospital, Seoul, Korea, between 2017 and 2021. Among the 46 cases, 10 were identified as anti-PD-1/PD-L1-induced BP (Table SI). Four of them were treated the combined regimen of anti-PD-1/PD-L1 and TGF-β inhibitor (TGFβi) (combination group); 6 patients were treated with anti-PD-1/PD-L1 only (monotherapy group). The culprit anti-PD-1/PD-L1 drugs included pembrolizumab, nivolumab, and durvalumab. TGFβi agents included vactosertib (TEW-7197), a selective small molecule inhibitor of TGF-β receptor type 1 and bintrafusp alfa (M7824), a bifunctional fusion protein composed of an antibody directed to PD-L1 fused to the extracellular domain of human TGF-β receptor type 2 (4, 5). There were 36 patients diagnosed with BP that was not associated with any cancer immunotherapy (idiopathic group, Table SII).
Using clinical images, patients’ Autoimmune Bullous Skin Disorder Intensity Scores (ABSIS) and Bullous Pemphigoid Disease Area Index (BPDAI) scores were assessed (6). To assess regional severity on acral areas; both hands and both feet were ascribed separate severity scores of 0–4 (0: none; 1: < 25%; 2: 25–50%; 3: 50–75%; 4: > 75% involvement). Statistical analysis was performed using Kruskal-Wallis H tests and Dunn’s multiple comparison tests.
There was no statistical difference in age between the idiopathic, monotherapy, and combination groups (p = 0.32; Tables SI and SII). The incubation time from the start of immunotherapy to BP onset was not different between the monotherapy vs combination groups (313.8 vs 241.0 days, p = 0.10).
Severity evaluation using ABSIS found a higher mean score in the combination group (43.6 points) compared to the idiopathic group (5.08 points, p = 0.007, Fig. S1A). The mean BPDAI was higher in the combination group (116.5 points) than the monotherapy group (22.7 points, p = 0.040) and the idiopathic group (18.6 points, p = 0.003, Fig. S1B).
Mucosal involvement was reported in 2 patients in the monotherapy group (33%) and 2 patients in the combination group (50%), which was significantly higher (p = 0.018, Fisher’s exact test) than the idiopathic group (n = 2, 5.5%). However, mucosal involvement was limited to oral mucosa, and the overall severity was mild in all reported cases.
Systemic glucocorticoid treatment dosage, which can indirectly reflect severity of BP, was evaluated as prednisolone-equivalent dose (mg/kg). A peak steroid dose of 1.22 mg/kg was necessary for control of acute flare in the combination group, which was a higher dose than either the monotherapy (0.54 mg/kg, p = 0.09) or idiopathic group (0.35 mg/kg, p = 0.005) (Fig. S1C). Correspondingly, the mean lowest steroid dose sufficient for maintenance in the combination group required a higher dose (0.30 mg/kg) than the monotherapy (0.10 mg/kg, p = 0.25) or idiopathic group (0.06 mg/kg, p = 0.003) (Fig. S1D).
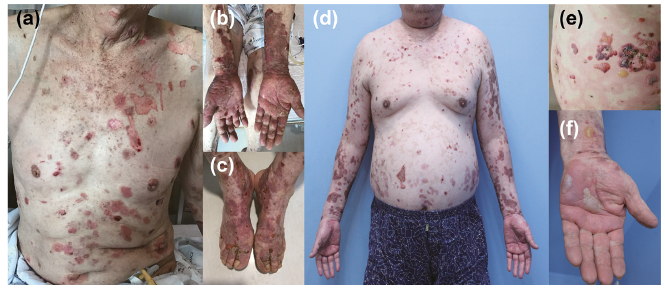
Patients in the combination group presented a patterned distribution with an acral predilection for hands and feet (Fig. 1). With a maximum possible score of 8 (0–4 scoring for hands, 0–4 scoring for feet), the combination group had a mean value of 6.50 points, which was significantly higher than monotherapy (0.67 points, p = 0.006) or idiopathic BP (1.19 points, p = 0.003) groups (Fig. S1E).
Fig. 1. Clinical presentations of anti-programmed cell death protein 1 (PD-1)/PD-ligand 1 (PD-L1)-associated bullous pemphigoid induced by a combination regimen including transforming growth factor-β inhibitors. (a) Case 1: extensive erosions induced by (b, c) bullae and severe involvement of acral areas. (d) Case 3: widespread erosions that originated from (e) typical tense bullae and (f) severe palmar involvement.
This case series documented severe, distinctively-patterned anti-PD-1/PD-L1-associated BP in patients treated with a TGFβi combination regimen. Moreover, a greater requirement on steroid dosage to control disease activity suggests that BP symptoms induced by this novel combination regimen are more difficult to manage.
Most patients in the monotherapy group reached the minimal dose or discontinuation of systemic steroids after discontinuation of the immunotherapy regimen. However, the combination group had a significantly more severe and protracted disease course. For instance, exceptionally high dosages (>1.3 mg/kg/day) of systemic steroids (e.g. case 1, 2) or additional immunosuppressants (e.g. case 3, 4) were required to prevent development of new blisters until withdrawal of the culprit drug (Table SI). Notably, the culprit drug was discontinued more rapidly in the combination group (mean, 4.5 days) than in the monotherapy group (37.7 days), suggesting that delayed drug discontinuation was not the cause of a more severe phenotype. In addition, patients in the combination group experienced frequent (50%) mucosal involvement of BP, further indicating a more severe disease presentation.
These findings indicate the importance of TGF-β signalling in restricting autoimmune bullous disease, particularly in cutaneous irAEs. This may be due to the role of the TGF-β signalling pathway for prevention of self-reactive B-cell activation and autoantibody production (7). TGF-β signalling also plays a key role in the proliferation of regulatory T cells, which produce IL-10 and TGF-β to promote immune regulation (8). Thus, disruption of this complex regulatory interaction may further reinforce ongoing inflammatory processes and result in a more severe BP presentation.
TGFβi combination regimen-induced BP had a greater predilection for acral areas. Considering the essential role of the TGF-β/Smad signalling pathway during limb regeneration or the preferential expression of TGF-β in the limbs vs the trunk during wound healing in animal models (9), imbalance of TGF-β, a pleiotropic signal, may be related to vulnerability of inflammatory processes in specific anatomical locations.
Since this study was a retrospective case series was performed at a single institution with a small group, future studies that include larger subject populations are required. Due to medical insurance guidelines in Korea, we were unable to measure serum levels of anti-BP180 autoantibody, which may be insightful in explaining the development of this distinctively-patterned and severe BP. Nonetheless, this study displays a relationship between the use of the TGFβi combination regimen and anti-PD-1/PD-L1-associated BP which implies the important role of TGF-β signalling for restricting development of autoimmune skin toxicity.
This work was supported in part by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (number 2020R1C1C1005198).
The patients in this article gave written informed consent to publication of their case details.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize