


1Department of Dermatology, Jeonbuk National University Medical School, 20 Geonji-ro, Deokjin-gu, Jeonju 54907 and 2Research Institute of Clinical Medicine of Jeonbuk National University – Biomedical Research Institute of Jeonbuk National University Hospital, Jeonju, Korea. E-mail: kyung1212@hanmail.net
Accepted Jul 1, 2021; Epub ahead of print Jul 5, 2021
Acta Derm Venereol 2021; 101: adv00494.
doi: 10.2340/00015555-3861
Cutaneous pili migrans (CPM) is a rare condition characterized by creeping eruption caused by a hair shaft embedded in the superficial skin or mid-dermis (1). The classic clinical presentation is a serpiginous, slightly elevated, erythematous, linear migrating skin lesion (2). Published data primarily comprises case reports involving a single lesion at various locations (e.g. foot, face, neck, breast, abdomen, extremities, and inguinal area) (1–3). We report here a case of CPM with a very rare presentation, of multiple, embedded short hairs on the axillae and neck.
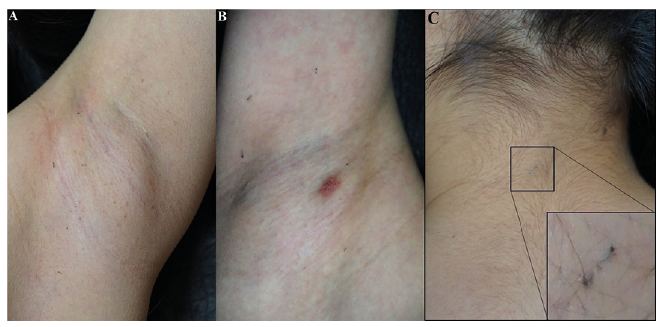
A 7-year-old girl presented with a 1-year history of asymptomatic “spreading black dots” on both axillae and neck. She had no history of travelling, shaving, or habitual rubbing. Her parents often embraced her and shared towels. Physical examination revealed multiple, slightly raised, linear, black eruptions (Fig. 1). Dermoscopy showed a black line running within the superficial and deep skin layers with both ends puncturing the skin, resembling a surgical stitch (Fig. 2). Histopathology revealed a penetrating, cross-sectioned hair shaft without a hair follicle, lying in the canal made by the burrowed surface epithelium (Fig. 3). The final diagnosis was CPM.
Fig. 1. Clinical findings of multiple cutaneous pili migrans. (A) Left axilla, showing multiple black dots and lines. (B) Right axilla, showing multiple black dots and lines and a scar on the erythematous patch from a biopsy. (C) Posterior neck, showing a black elevated area between 2 horizontally-oriented black dots with central sparing.
Fig. 2. “Hair stitch sign” on dermoscopy, revealing a black line, probably a hair shaft, within the superficial and deep skin layers, with both ends puncturing the skin, presenting as black dots resembling a surgical stitch.
Fig. 3. Histopathology showing a cross-sectioned hair shaft and absence of a hair follicle, consistent with the diagnosis of cutaneous pili migrans. The epidermis is rolled inward and appears upside down with mild lymphocytic and histiocytic infiltration around the hair shaft without eosinophilic infiltration (haematoxylin and eosin, ×40).
After applying topical anaesthetic cream without making an incision, gentle pressure was applied to one end of the canal, while the visible black hair shaft was pulled through the other opening with forceps. No bleeding occurred before or after the procedure. Seven of 11, 8 of 9, 4 of 5, and all 8 foreign bodies extracted from the right axilla, left axilla, anterior neck, and posterior neck, respectively, were found to be hair shafts on light microscopy (LM) and scanning electron microscopy (SEM). The longest and shortest hair shafts were 3 and 0.3 mm, respectively. The thickness ranged from 200 to 230 µm. Hair samples from the patient and her parents, including her father’s moustache, were collected, and their thickness measured using SEM: 91.29–97.21 μm (father’s hair shaft), 132.6–168.7 μm (father’s moustache), 90.19–92.99 μm (mother’s hair shaft), and 82.90 μm (patient’s hair shaft). Complete remission without recurrence was observed at 6 months. The family members were advised to avoid sharing towels and to refrain from close contact with the father’s moustache.
After Yaffe reported a case of “imbedded hair” resembling cutaneous larva migrans (CLM) in 1957 (4), a hair inducing migrating skin eruption has also been described as “bristle migrans”, “burrowing hair”, “hair fragment in the skin”, “creeping hair”, “migrating hair”, “creeping eruption”, and CPM (3–8). Among these, Francesco suggested “burrowing hair (pili cuniculati)” as a novel term, because the lesion appeared similar to horizontally and superficially formed burrows of scabies (6). Likewise, “pili cuniculati” more appropriately describes the current case, because dermoscopic and histopathological findings revealed clear burrows, and the short hair fragments did not conspicuously represent the typical migrating serpiginous manifestation of CLM. Therefore, we described the current case as pili cuniculati multiplex, a variant of CPM in which multiple, short hairs are burrowed.
Dermoscopy and biopsy are valuable diagnostic tools for CPM. A mobile dark line that runs within the superficial skin layer is the characteristic dermoscopic finding of classic CPM (9, 10). In the current case, the dermoscopic view resembled a surgical stitch, because short hair fragments were burrowed superficially at both punctured ends. Therefore, we propose the term hair stitch sign as a novel dermoscopic description. The absence of hair follicles with inflammation surrounding the hair shaft without eosinophils is the characteristic histopathological finding (11). The current case showed shorter linear lesions than other common presentations of CPM. Repeated penetration of short hair fragments may cause interdigital pilonidal sinuses, as observed in hairdressers or barbers (12, 13). However, granulomatous inflammation was not observed in the current case. Some authors suggested that CPM develops from ingrown hair burrowing in the superficial skin (3, 14). However, the current case had a hair shaft without a follicle, suggesting an extrinsic origin.
Although the aetiology of CPM has not been established, penetration of extrinsic hair shafts has been suggested, mostly affecting Asians with thick hair of high tensile strength (1, 2). A combination of the sharp-pointed hair shaft, body surface movement forces, and the biomechanical force exerted during limb movement is a postulated mechanism (15). Known risk factors are also mainly extrinsic; including shaving, habitual pulling, and walking barefoot (2, 9, 14). Based on the hair thickness of the patient’s family, measured by SEM, the father’s moustache was the most likely origin, and application of local anaesthetic cream probably induced swelling of the embedded hair shaft. Moreover, the thick, stiff, straight characteristics of men’s hair would increase its penetrability (13). This is the first case of CPM involving both axillae, in which the more permeable skin barrier in a child and thinner epidermis on intertriginous areas probably contributed to a susceptible environment. Frequent hugging and sharing of towels probably contributed to the occurrence of CPM in this rare location.
Most treatment modalities for CPM involve shallow incisions, using a blade or needle, which often cause pain and bleeding (2, 9). For the optimal treatment modality for multiple CPM, we suggest applying light pressure to one end of the embedded hair shaft while pulling the exposed tip at the other end, using forceps, to remove the hair shaft. Dermoscopy can be used to locate the openings of the punctured skin to facilitate this process. While the previous treatment modality was invasive and involved incisions or needle punctures, this minimally invasive technique using forceps and dermoscopy minimizes pain, bleeding, time-consumption, and secondary infection risk.
To the best of our knowledge, this is the first case report of multiple CPM occurring at multiple locations. This case provides valuable insights and raises questions for dermatologists on whether pili cuniculati multiplex is likely to have been underdiagnosed because the burrowed short hairs are primarily asymptomatic and are often unrecognized. In conclusion, when multiple CPM is suspected, we suggest careful inspection using dermoscopy and non-invasive treatment using the simple application of gentle pressure with forceps.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize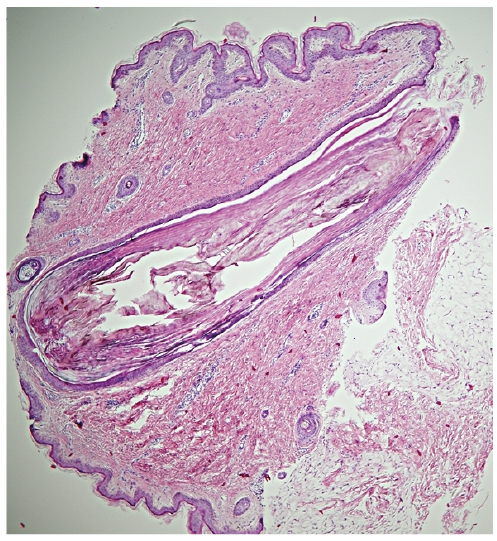 Click to show fullsize
Click to show fullsize