


1Keck School of Medicine, University of Southern California, Los Angeles, 2School of Medicine, University of California Riverside, Riverside, CA, 3Western University of Health Sciences, Pomona, CA and 4Dermatology Research and Education Foundation, Irvine, CA, USA. *E-mail: jashinwu@gmail.com
Accepted Jul 1, 2021; Epub ahead of print Jul 5, 2021
Acta Derm Venereol 2021; 101: adv00518.
doi: 10.2340/00015555-3864
Emerging evidence has suggested that chronic systemic inflammation plays an important role in psoriasis and respiratory comorbidities, including asthma, chronic obstructive pulmonary disease (COPD), sarcoidosis and interstitial lung disease (1). The principal cause of COPD is smoking, followed by pulmonary inflammation. In recent literature, a large nationwide cohort study demonstrated that patients with psoriasis have a greater risk of developing COPD during 18-month follow-up compared with controls (2). Whether this association is attributable to chronic inflammation from psoriasis or from smoking remains unknown. To date, few studies have examined the relationship between psoriasis and COPD by smoking status in a representative sample of US adults. This cross-sectional study aimed to determine the role of smoking status in the association between psoriasis and COPD in the US population using the most recent data from the 2009 to 2014 National Health and Nutrition Examination Surveys (NHANES) (3).
The study was approved by the National Center of Health Statistics ethics review board. De-identified data were then assessed from the following NHANES cycles: 2009 to 2010, 2011 to 2012, and 2013 to 2014. Sample weights were computed from the US census bureau to adjust for survey non-response and stratification of demographic variables, including age, sex, race/ethnicity, income, education, and marital status. Consistency of sampling methods between cycles allowed for inclusion of sample weights across all 6 years of the NHANES. The questionnaire comprised baseline demographics (age, sex, race/ethnicity, income, education, and marital status), history of psoriasis, history of chronic bronchitis, history of emphysema, and other medical conditions. Participants were selected based on a complex, 4-stage, stratification to reflect the non-institutionalized civilian resident population of the USA. Hispanic, African American, Asian, and low-income Caucasians were oversampled to increase the precision of prevalence estimates in these traditionally underrepresented populations. Psoriasis status was determined by affirmative responses to the question “Have you ever been told by a doctor or other health care professional that you had psoriasis?” Controls were defined as all participants who responded “No” to the question. Self-reported diagnosis of chronic dermatological conditions has demonstrated sufficient validity, with sensitivity of 61%, specificity of 69%, and positive predictive value of 82% reported in validation studies (4). This self-report method of ascertaining psoriasis status has been used in numerous other epidemiological studies of psoriasis (5–8). Chronic bronchitis status was determined by affirmative responses to “Has a doctor or other health professional ever told you that you had chronic bronchitis?” Emphysema status was determined by affirmative responses to “Has a doctor or other health professional ever told you that you had emphysema?” A composite binary variable was created for COPD, using responses to the above 2 questions. Participants who answered “No” to the question “Have you ever smoked at least 100 cigarettes in your entire life?” were classified as never smokers, while those who answered “Yes” to the question above were classified as ever smokers. In addition, ever smokers who answered “Yes” to the question “Do you now smoke cigarettes?” were classified as current smokers. Ever smokers who answered “No” to the question above were classified as ex-smokers.
Multivariable logistic models were constructed on SAS version 9.4 with psoriasis as the explanatory variable, COPD as the dependent variable, and the following covariates to adjust for confounding: age, sex, race/ethnicity, socioeconomic status/SES (insurance, healthcare access), and obesity. To evaluate smoking status as a potential effect modifier, subgroup analyses was performed on never-smokers, ever-smokers, current smokers, and ex-smokers.
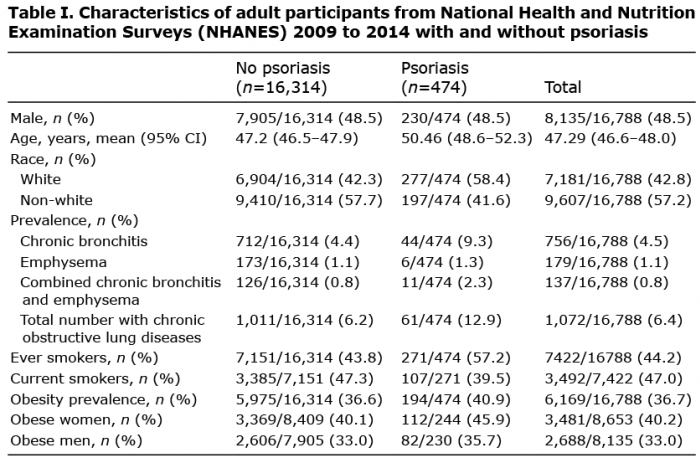
Of the 16,788 participants who responded to all survey items from adults aged 20 years and older, 474 participants were classified as having been diagnosed with psoriasis and 16,314 participants had no psoriasis (Table I). Overall COPD prevalence was higher in patients with psoriasis compared with controls (12.9% vs 6.2%) (Table I). The odds of having COPD were significantly increased in psoriasis patients (aOR 1.42 95% confidence Interval (95% CI) 1.01–2.01) (Table SI). On stratification of the population by smoking status, psoriasis was a risk factor for COPD only in current smokers (aOR 1.97 95% CI 1.19–3.25), but not in never smokers (aOR 1.27 95% CI 0.60–2.69), ever smokers (aOR 1.28 95% CI 0.80–2.04), or ex-smokers (aOR 1.09 95% CI 0.52–2.27) (Table SI). On stratification of current smokers by pack-year history, psoriasis was a risk factor for COPD only in participants with a smoking history of greater than 20 pack-years (aOR 2.17 95% CI 1.06–4.44) (Table SII).
Table I. Characteristics of adult participants from National Health and Nutrition Examination Surveys (NHANES) 2009 to 2014 with and without psoriasis
The aim of this study was to determine the role of smoking status in the association between psoriasis and COPD in the US population. In the current analysis, the prevalence of self-report of a healthcare provider diagnosis of COPD was statistically similar to previous estimates from prior NHANES cycles (9). Psoriasis is positively and significantly associated with the risk of COPD in the general US population. Upon stratification, the relationship between psoriasis and COPD risk was modified by smoking status, with this relationship being significant only in current smokers.
Several mechanisms have been postulated to be critical for the increased risk of COPD in patients with psoriasis. In 1 study, IL-17A, the major effector cytokine in the pathogenesis of psoriatic disease, was increased in the bronchial mucosa of stable COPD patients (10). In addition to keratinocyte stimulation, IL-17 has proinflammatory activities and acts as a potent inducer of airway mucins and sputum inflammatory markers seen in COPD exacerbations (11). In another study, spirometry and markers of airway inflammation, such as exhaled fraction of nitric oxide (FeNO), were positively correlated with PASI (12). These findings may suggest that chronic inflammation from psoriasis potentially results in a similar deleterious effect on the alveolar epithelial lining. However, the findings from the current study suggest that the relationship between psoriasis and COPD may be non-causal, as patients with psoriasis in the absence of active or passive smoking may not have an underlying risk of developing COPD. Clinically, these results highlight the importance of smoking cessation and counselling for patients with psoriasis.
The NHANES contains data collected through on-site examinations and interviews with demographic, socioeconomic, dietary, and health-related questions. Among the primary strengths of the study design, NHANES participants are selected to be representative of the general US population. Among the primary limitations, the cross-sectional design precludes the ability to measure temporal sequence between psoriasis, smoking, and COPD, since exposure and outcome are ascertained at the same time. In addition, the use of self-report of physician-diagnosed chronic bronchitis and emphysema may subject patient interview data to recall bias. Patients may forget previous diagnoses, recall a non-existent diagnosis, misunderstand questions, or be influenced by various factors that may lead to imprecise estimates of disease prevalence. Nevertheless, questionnaire-based case definitions (i.e. affirmative responses to physician-diagnosed chronic bronchitis and emphysema) are generally highly specific (96%), accurate (89–90%), and widely accepted in various epidemiological studies of COPD (2, 13).
In conclusion, smoking modifies the association between psoriasis and COPD in US adults. Patients with psoriasis who do not smoke may not have an increased risk of developing COPD. Counselling patients with psoriasis on the benefits of smoking cessation remains a valuable approach for preventing worsening of clinical severity and COPD risk.
JJW is or has been an investigator, consultant, or speaker for AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Dermavant, Dr Reddy’s Laboratories, Eli Lilly, Galderma, Janssen, LEO Pharma, Mindera, Novartis, Regeneron, Sanofi Genzyme, Solius, Sun Pharmaceutical, UCB, Valeant Pharmaceuticals North America LLC, and Zerigo Health.
The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize