


Department of Dermatology, The First Hospital of China Medical University, 155N Nanjing Street, Shenyang 110001 P.R. China. E-mail: guohao27@126.com; Pfkl2011@126.com
A 70-year-old woman with widespread pruritic nodules on her back, trunk, arms, and legs, which had persisted for 6 years, presented to our department. There were fewer lesions on areas of the body that were not scratched, such as the upper back, compared with her limbs. She had been treated with triamcinolone acetonide acetate ointment (0.1%), 2 times a day, and oral ebastine 10 mg, 4 times a day, for 2 weeks, with no significant improvement. The affected areas increased gradually to include almost her entire body and morphed into pruritic plaques and nodules over the course of 6 years (Fig. 1). Due to irritation, the patient had been scratching at the lesion sites, with the result that the lesions and surrounding normal skin regions frequently showed ulcerations, bleeding, and scabs. She had a history of hypertension for 6 years and had been taking Levamlodipine maleate 2.5 mg daily. Results from laboratory assays revealed the level of circulating IgG to BP180 was 111.4 U/ml (normal < 9 U/ml), increased levels of serum erythrocyte sedimentation rate (ESR) at 27 mm/h (normal 0–20 mm/h) and IgE of 494.4 IU/ml (normal 0–100 IU/ml), but no signs of eosinophilia (eosinophils 0.04~0.31×109/l). A biopsy was performed from a lesion on her right forearm, showing an interface dermatitis with erosive ulcers on the epidermis and infiltrations of lymphocytes and histiocytes into the entire dermis. Neutrophil infiltration was observed in the superficial dermis deep to the erosive ulcers of the epidermis. Direct immunofluorescence analysis of the skin from the lesion showed C3 linear bands along the dermoepidermal junction (Fig. 2). Previous measurements of circulating IgG to BP180 were negative (0.0 U/ml) 2 years earlier, and no biopsy or immunopathological assays were performed at that time. The patient had previously been diagnosed with prurigo nodularis and the skin lesions had improved after oral triamcinolone 24 mg with gradual reduction over a period of 6 months.
Following presentation and assessment at our hospital she was commenced on oral triamcinolone (24 mg daily) and supplemental potassium and calcium. Her skin condition improved remarkably. At the 3-month follow-up, most of the nodular lesions had subsided and no new lesions were present (Fig. 3). The dose of oral triamcinolone was reduced gradually and the patient remains in follow-up.
What is your diagnosis? See next page for answer.
Fig. 1. Skin lesions. Elevated pruritic nodules on the (a) upper and (b) lower limbs, covered with excoriations and occasional crusts.
Fig. 2. Histological and immunological stains. (a) Biopsy specimen of lesions from the right forearm showing infiltrations of lymphocytes and histiocytes in the entire dermis and neutrophil infiltrations in the superficial dermis deep to erosive ulcers of the epidermis (haematoxylin-eosin stain; original magnification×200). (b) Direct immunofluorescence analysis of this biopsy showing a linear deposition of C3 along the dermo-epidermal junction (magnification×200).
Fig. 3. Skin lesions after treatment for 3 months. Most of the lesions on the (a) upper and (b) lower limbs subsided, leaving pigmentations at these sites.
Acta Derm Venereol 2021; 101: adv00519.
Diagnosis: Pemphigoid nodularis
Clinicopathological correlation was consistent with a diagnosis of pemphigoid nodularis. Pemphigoid nodularis, a clinically distinct variant of bullous pemphigoid, is a relative rare disease. This condition is characterized by chronic pruritus nodular lesions with an immunohistochemical profile of pemphigoid in the lesioned and normal skin (1). As the clinical manifestations are similar to that of prurigo nodularis, pemphigoid nodularis is frequently misdiagnosed.
Pemphigoid nodularis was initially characterized and named by Yung et al. in 1981 (2) and shows a higher morbidity in elderly females (3, 4). Due to the limited information available on pemphigoid nodularis, dermatologists frequently misdiagnose this disease as prurigo nodularis. Moreover, the absence of any salient pathological and laboratory assay results in the early stages of this disease further complicates the diagnosis of this condition. However, the histological features of pemphigoid nodularis can be differentiated from prurigo nodularis. In pemphigoid nodularis, dermal infiltration of inflammatory cells is noticed. A linear deposition of C3 or IgG along the dermo–epidermal junction can be detected under direct immunofluorescence in pemphigoid nodularis. In prurigo nodularis, hyperkeratosis of epidermis, hypertrophy of spinous layer, pseudoepitheliomatous hyperplasia of epidermis, and infiltration of inflammatory cells in the dermis are noted. The direct immunofluorescence of prurigo nodularis is negative. Thus, with this case report, we hope to alert dermatologists to the possibility of pemphigoid nodularis.
There are several approaches that can be employed for treatment of pemphigoid nodularis, including systemic corticosteroids, azathioprine, dapsone, intravenous immunoglobulins and minocycline. However, topical and systemic corticosteroids is the most effective treatment for pemphigoid nodularis (3). Based on findings reported in the literature, use of topical corticosteroids and antihistamines are insufficient for pemphigoid nodularis. Thus, the ability to correctly diagnose pemphigoid nodularis becomes particularly important. When prurigo nodularis-like eruptions appear, dermatologists should consider the possibility of pemphigoid nodularis and perform histological examinations.
Different opinions exist on the pathogenesis of pemphigoid nodularis. Some authors have suggested that pemphigoid nodularis may present with numerous autoantibodies, presumably due to epitope spreading as a consequence of the intense scratching of pruritic nodules. Epitope spreading is a dynamic change due to recruitment and activation of autoreactive T lymphocytes specific for “secondary” epitopes of the autoantigen contributing to the disease course (5–7). The current case supports this opinion, as autoantibodies could not be detected 2 years earlier. In recent years, it has been reported that pemphigoid nodularis can be triggered by drugs (8). There are 2 cases in the literature reported by Ross et al. (9) in 1992, where nodules appeared after the diagnosis of bullous pemphigoid had been established via the presence of autoantibodies (BP180/230).
Clinically, it is important to distinguish pemphigoid nodularis from prurigo nodularis as soon as possible, as pemphigoid nodularis requires more systemic immunosuppression. Although prurigo nodularis is the principal clinical differential diagnosis, it is necessary to differentiate other diseases, such as actinic prurigo, epidermolysis bullosa pruriginosa, prurigo nodularis-like lepromatous leprosy, and cutaneous T-cell lymphomas, by typical histological and direct immunofluorescence features of pemphigoid nodularis. For those patients with the clinical manifestations of prurigo nodularis, it is recommended to conduct biopsy and direct immunofluorescence promptly, as well as measuring circulating IgG to BP180 and BP230, which should be monitored regularly during long-term follow-up.
We thank the patient for allowing us to use her pictures and clinical data. We also thank Dr Song Zheng and Dr Guang-Yu Jin from the First Hospital of China Medical University for helping with the pathology. This work was supported by the National Nature Science Foundation of China (81903228 HG) for data collection.


 Click to show fullsize
Click to show fullsize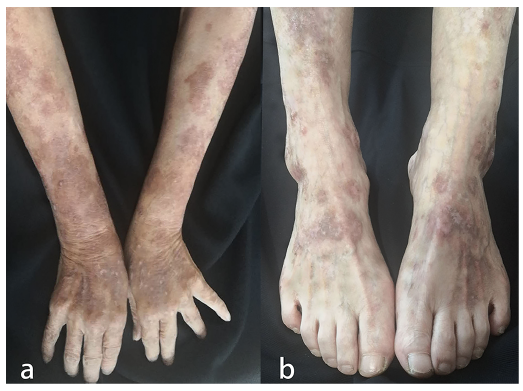 Click to show fullsize
Click to show fullsize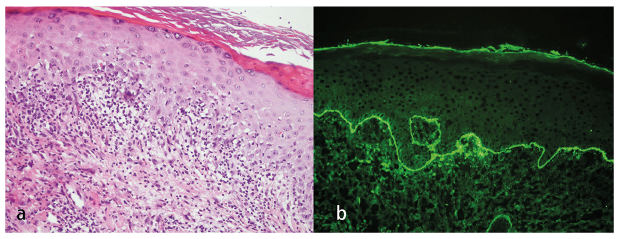 Click to show fullsize
Click to show fullsize