


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroc?aw, Poland
The incidence of basal cell carcinoma has increased in recent years. The aim of this study was to analyse the influence of itch on quality of life and psychosocial status of patients with basal cell carcinoma. A total of 180 patients with basal cell carcinoma were included in the study. Itch intensity was assessed with Numerical Rating Scale and 4-Item Itch Questionnaire (4IIQ). Quality of life in basal cell carcinoma was assessed with the 36-item Short-Form Health Survey (SF-36), Dermatology Life Quality Index (DLQI), 6 Item Stigmatization Scale (6-ISS) and Beck Depression Inventory (BDI). Mean DLQI in the study group was 2.0 ± 2.0, while mean SF-36 was 71.38 ± 15.77 points. The intensity of itch assessed with 4IIQ correlated negatively with SF-36 (R = –0.48, p = 0.003). The mean ± SD BDI score was 6.16 ± 5.72 points and mean 6-ISS score was 0.66 ± 1.24. In conclusion, presence and intensity of itch may debilitate quality of life among patients with basal cell carcinoma.
Key words: basal cell carcinoma; quality of life; itch; stigmatization; depression.
Accepted Jul 6, 2021; Epub ahead of print Jul 7, 2021
Acta Derm Venereol 2021; 101: adv00507.
doi: 10.2340/00015555-3871
Corr: Jacek C Szepietowski, Department of Dermatology, Venereology and Allergology, Cha?ubi?skiego 1, PL-50-368 Wroc?aw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Basal cell carcinoma is the most common humane cancer, and its incidence is still raising. Here we analyzed the data of 180 patients with basal cell carcinoma regarding the influence of itch on quality of life and psychosocial status of these patients. Patients struggling with this skin cancer had greatly reduced general health perception comparing to the normative population. Moreover, more than 15% of these patients may be threatened with the co-existence of depression. Itch presence and intensity may diminish quality of life among the affected subjects with basal cell carcinoma.
Basal cell carcinoma (BCC) is the most common malignancy in humans. BCC might be debilitating, not only because of the character of the tumour itself, but also due to frequently encountered symptoms, such as moderate itching, stinging, tingling or burning sensations (1, 2). The incidence of BCC has increased in recent years, affecting a younger population. Although the mortality rates are low, treatment of BCCs is associated with high morbidity. Eighty percent of BCCs are located on the head or neck, and an estimated 40% of patients who develop their first non-melanoma skin cancers (NMSC) also develop at least 1 additional tumour within 2 years of diagnosis (3). Prevalence of BCC-associated itch varies from 15.5% to 31.9% of patients (1, 2, 4–7). Itch may influence patients’ quality of life (QoL), depriving patients of sleep and causing annoyance (2). However, studies evaluating the impact of itch on the psychosocial state of patients with BCC are lacking.
The aim of this study was to analyse the psychosocial status of patients with BCC and the influence of itch on patient well-being in a group of subjects with histologically confirmed diagnosis of BCC.
Patients
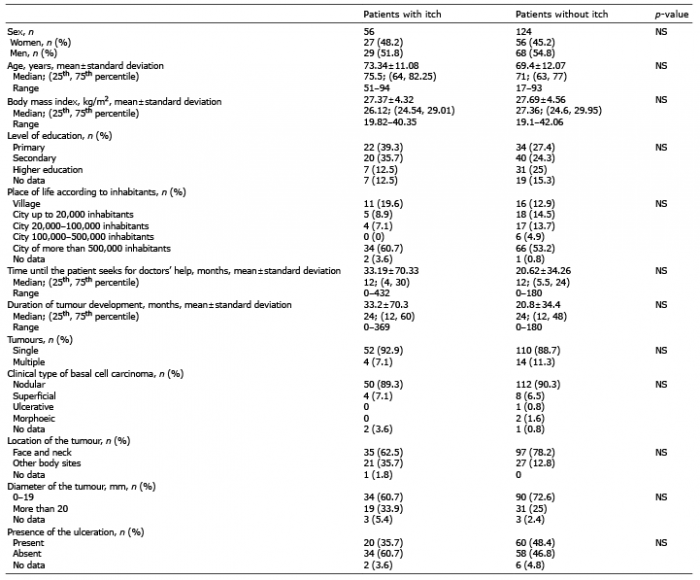
A total of 200 consecutive patients over the age of 17 years with histologically confirmed BCC, who were referred for surgical treatment, were invited to join the study. Twenty patients declined to participate (response rate 90.0%). Exclusion criteria included a history of chronic dermatological or psychiatric disease. The final study group was 180 patients (83 women, 97 men). The age range of the studied individuals was 17–95 years (mean ± standard deviation (SD) 70.5 ± 11.9 years). No subjects received specific antipruritic treatment. Detailed demographic data are shown in Table I. Patients with BCC without itch did not differ from those with itch concerning age, sex, body mass index (BMI) and duration of the lesion. The study was approved by the Wroclaw Medical University ethics committee (ST.C260.18.019).
Table I. Basic demographics and tumour-related data for itchy and non-itchy patients
Study design and questionnaires
Detailed information on demographic data and clinical history were collected from all participants (Table I). Unidimensional scale – Numerical Rating Scale (NRS) was used to evaluate itch, where the patients were asked to they had experienced during the last report on an 11-point scale, the maximum intensity of itch 3 days and during the whole course of the tumour. The score ranged from 0 (no itch) to 10 points (worst imaginable itch), with cut-off points for NRS as follows: 1–2 points: mild itch, 3–6 points: moderate itch, 7–8 points: severe itch and very severe itch with more than 9 points (8). In addition, the itch was characterized with a 4-item Itch Questionnaire (4IIQ). This instrument was successfully utilized by our group to estimate the extent (1–3 points), intensity (1–5 points), frequency (1–5 points) and sleep disturbances (0–6 points) caused by the itch of various types (9–11).
To evaluate a wide spectrum of psychosocial aspects, all patients were asked to complete the validated Polish language versions of multiple questionnaires. All the questionnaires were distributed among patients shortly before surgical treatment after thorough instructions about how to complete them and were completed by the patients alone, without any help from the investigator.
Health-related quality of life (HRQoL) was evaluated with 2 different questionnaires: (i) a generic instrument: the 36-item Short-Form Health Survey (SF-36) (12), and (ii) a dermatological-specific questionnaire: Dermatology Life Quality Index (DLQI) (13). The SF-36 consists of questions concerning physical and mental health status within the last 4 weeks. Thirty-six items of the SF-36 are related to 8 different dimensions: physical functioning (PF), role limitation-physical functioning (RP), bodily pain (BP), general health perception (GH), vitality (V), social functioning (SF), role limitation-emotional functioning (RE) and mental health (MH). The 8-dimension scores range from 0 to 100 points, with a lower score indicating a worsened functioning and lower level of HRQoL (12). Apart from the points obtained for particular areas, the questionnaire allows to obtain 2 additional summary results; 1 for the physical component (PCS) and the other for the mental component of quality of life (MCS). The components of MSC are V, SF, RE, MH, while the physical component (PCS) consists of the subscales PF, RP, BP, GH. The DLQI, because of its self-explanatory questions, is one of the most commonly used tools for the assessment of HRQoL in dermatology. The DLQI score ranges from 0 to 30 points, with a lower score indicating better HRQoL. According to the classification of DLQI score proposed by Hongbo et al. (14), 0–1 points indicates normal QoL, 2–5 points indicate slightly impaired, 6–10 points severely impaired, 11–20 points very severely impaired, and 20–30 extremely severely impaired HRQoL.
The assessment of depression symptoms was based on the Beck Depression Inventory (BDI) (15), which comprised 13 items (score range 0–39). Each item of BDI is evaluated from 0 to 3 points. It is widely accepted for screening purposes that the BDI cut-off points suggesting a depression are 10 or above (16). 6-Item Stigmatization Scale (5-ISS) was developed for the assessment of stigmatization level (score range 0–18). The higher the scores, the greater the stigmatization level was observed (17).
Statistical analysis
Statistical analyses were performed using Statistica 12 software (StatSoft, Tulsa, OK, USA). All data were assessed for parametric or non-parametric distribution. Pearson’s χ2 test was applied to sets of categorical data. Differences between groups were determined using the Mann–Whitney U test, as analysed variables were of abnormal distribution. Correlations were determined by Spearman correlation analysis. The resulting p-values were considered nominally significant at p < 0.05 level.
BCC-associated itch was present in 56 out of 180 studied patients (31.1%). According to the NRS, the maximum intensity of itch in the whole period of existing tumours was assessed as 3.4 ± 1.8 points (range 1–8 points), and during the last 3 days as 3.1 ± 1.2 points (range 1–5 points). Of patients reporting itch during the whole duration of tumour disease, 23.5% did not experience any itch during the last 3 days, while mild itch was observed in 25% of patients and moderate itch in 51.5% of patients. The mean result for 4IIQ was assessed as 4.3 ± 2.4 points (range 3–15 points) and significantly correlated with NRS both during the last 3 days and during the whole period of the existing tumour (r = 0.36, p = 0.01, and r = 0.32 p = 0.02, respectively).
A total of 140 patients completed the SF-36 questionnaire (30 patients with itch, 110 patients without itch). Mean SF-36 for the whole studied population was assessed as 71.38 ± 15.77 points (with mean MHC 77.53 ± 15.28 points and PHC 68.09 ± 23.04 points). According to the SF-36, there were no significant differences in total score of SF-36 in patients with and without itch (70.38 ± 15.77 and 71.67 ± 15.9 points, respectively). Separate analysis of each dimension of SF-36 revealed no statistically significant differences among the analysed groups (Table II, Fig. 1). Despite the lack of significant differences in the level of functioning, significant negative correlations were found between total SF-36 score and intensity of itch assessed with 4-IIQ (R = –0.48, p = 0.003). Concerning the dimensions of SF-36, the intensity of itch in 4IIQ correlated negatively with PHC (R = –0.50; p = 0.001) and its components: PF, RP, GH (R = –0.43; p = 0.008; R = –0.4, p = 0.02; R = –0.48, p = 0.002, respectively). Itch intensity also correlated negatively with 1 of the components of MHC–MH (R = –0.53, p < 0.001). Concerning factors other than itch that may influence SF-36, age correlated negatively with the total SF-36 score (R = –0.23; p = 0.009) and the PHC component (R = –0.21; p = 0.02). On the other hand, place of living slightly influenced the MHC component: there was a negative relationship between city population and MHC (R = –0.17, p = 0.05) and its components – SF and V in SF-36 (R = –0.18, p = 0.04; R = –0.19, p = 0.03, respectively). Subjects with a higher level of education were also predisposed to have lower MHC and its component V (p = 0.03 for both). The higher the SF component, the longer the time until the patient decided to seek doctors’ help (R = 0.18, p = 0.03).
Table II. Questionnaires’ scores and dependencies on selected clinical data
Fig. 1. Dermatology Life Quality Index (DLQI) scores among patients with basal cell carcinoma (BCC) in comparison with patients with other dermatoses. The DLQI results obtained for BCC should not be compared directly with those for other skin diseases, as the data come from distinct studies. BCC: basal cell carcinoma, SCC: squamous cell carcinoma, NMSC: non-melanoma skin cancer.
To further assess the impact of itch on HRQoL in patients with BCC, the DLQI was employed. A total of 52 itchy patients with BCC completed the DLQI questionnaire, compared with 79 patients without itch who decided to complete the questionnaire (Table I). The mean DLQI in the whole group was 2.0 ± 2.0 points. Patients with itch had a significantly (p = 0.002) higher score of DLQI than those without itch (2.7 ± 2.7 and 1.5 ± 1.9 points, respectively). Moreover, significant correlation was found between DLQI score and intensity of itch assessed with the 4IIQ (R = 0.37, p = 0.008). DLQI score correlated negatively with total SF-36, MHC and PHC (R = –0.2, p = 0.04; R = –0.24; p = 0.01; R = –0.21 p = 0.03, respectively). Analysing several other factors, including the patients’ demographic and the time until the patient seeks doctors’ help, no significant correlations were found between these factors and DLQI score (detailed data not shown).
A total of 153 patients completed the BDI (46 out of the itchy group and 107 out of the non-itchy group). The mean BDI score was 6.16 ± 5.72 points. There were no significant differences in the total score of BDI in patients with and without itch (Table I). In our study group 25 patients (16.34%) had clinically suspected depression (BDI ≥ 10). Suspected depression in the itchy group was noted in 17.39% and within the non-itchy BCC group in 15.88%; however, the difference between both groups did not reach the significance level (p > 0.05). BDI scores correlated positively with the patient’s age (R = 0.2, p = 0.01).
Concerning stigmatization, a total of 118 patients completed the 6-ISS questionnaire fully (44 itchy patients and 74 subjects without itch). Mean score was 0.66 ± 1.24 points in the whole cohort of patients in this study. 6-ISS scores showed no statistical differences between the 2 studied groups (Table I). There was also no significant correlation between itch intensity and 6-ISS scores. There was no statistically significant correlation between intensity of itch and level of stigmatization. Sex, age, place of living, BMI, and the time until the patient seeks doctor’s help did not correlate with the 6-ISS score.
Analysing several other factors concerning the lesion, including the location (face and neck compared with other regions), number (single lesion compared with multiple lesions), clinical presence of the ulceration, size (diameter up to 20 mm compared with more than 20 mm) and clinical subtype, we were unable to find any significant correlations between the analysed factors and the questionnaire-related scores of the patients’ psychological status (detailed data not shown).
The results of this study indicate that there is an impact of BCC-associated itch on HRQoL. Patients with itch had significantly higher impairment of HRQoL measured with DLQI. Moreover, the itch intensity influenced not only the mental health of the patient, but also self-assessed physical health.
BCC-associated itch was first described 13 years ago (7); however, its frequency, pathophysiology, management, and impact on QoL have not been fully established. Amongst the limited published data focusing on the impact of BCC on QoL, it was emphasized that BCC had no or hardly any influence on patient QoL (18–23). To the best of our knowledge, this is the first study of BCC-associated itch that focuses predominantly on the influence of itch on the psychological status of patients, utilizing different validated questionnaires.
Mean DLQI in the current study group was 2.0 ± 2.0 points, indicating slightly impaired HRQoL, in concordance with previous studies. Analysing the literature, only a few studies dealing with QoL in BCC were found. Blackford et al. (21), in 1996, prospectively evaluated 44 patients with BCC, using the DLQI at baseline and 3 months after treatment. As was found in the current study, the scores demonstrated slight handicap (mean DLQI 5.3 ± 4 points) associated with the disease at baseline, with a significant reduction after treatment (p < 0.01). Other studies focus on QoL in NMSC. In contrast to previously mentioned findings, Çetinarslan et al. (24) assessed 255 patients with facial NMSC referred for surgical treatment, of whom 174 had BCC (68.2%). All participants completed the DLQI at baseline and 3 months after surgery. In patients with BCC, mean total DLQI scores were 6.37 ± 6.28 points, indicating severely impaired QoL, with significant improvement after surgical treatment. QoL of patients with NMSC was affected by tumour localization on the head area, treatment procedure and last, but not least, primary, or recurrent tumour (results concerned specifically with BCC were not revealed). Abedini et al. (23) assessed 95 patients with NMSC, of whom 75 had BCC (78.94%). Mean DLQI scores of all participants were 4.1 ± 4.25 points (range 0–16 points), indicating slight impairment in QoL. In the group of patients with BCC, the mean DLQI was 3.9 ± 0.4 points. There were no statistically significant differences between the QoL of patients with BCC and those with squamous cell carcinoma (SCC). Rhee et al. (19), in 2004, conducted a study on 121 consecutive patients with NMSC (103 with BCC) referred to a dermatological Mohs surgery clinic with the lesion of the head and neck. Assessment of QoL was performed using the DLQI before and 4 months after surgical treatment. Once again, QoL scores demonstrated little handicap (mean DLQI was 2.4 ± 2.7 points) at initial diagnosis, with only a small change after surgery. In contrast to these findings, Steinbauer et al. (25), in Germany, received different results. Her group comprised a study of 52 patients with NMSC, of whom 36 (69%) had a confirmed diagnosis of BCC and completed the German version of the DLQI questionnaire. The results showed that 31% of the patients experienced moderate-to-severe impairment in QoL; however, the detailed score of total DLQI was not provided. QoL in patients with NMSC has also been evaluated in patients treated non-surgically, such as with vismodegib hedgehog pathway inhibitor therapy. Villani et al. (26) evaluated HRQoL using the DLQI in 48 patients with advanced and/or multiple BCC who were undergoing the above-mentioned therapy. The mean reported DLQI score was 5.7 points. They found that patients with BCC in visible areas, such as the face or neck, presented an overall DLQI that was higher than in patients with BCC located on the trunk and legs at the baseline visit. However, DLQI scores of these 2 groups were decreased to almost the same point after 6 months of vismodegib therapy. Thanks to common and worldwide usage of the DLQI questionnaire, it is relatively easy to make an assessment comparing not only with other skin tumours, but also with other dermatological conditions, such as hidradenitis suppurativa (27), atopic dermatitis (28), chronic urticaria (28), alopecia (29), acne (30), psoriasis (31), Hailey-Hailey disease or Darier’s disease (32) (Fig. 2). QoL of patients with BCC seems to be less affected than in the above-mentioned dermatoses, and is similar to other skin tumours (33). One can even suggest that DLQI items are more appropriate to evaluate chronic, inflammatory skin conditions, such as psoriasis or atopic dermatitis, because they emphasize physical complaints of irritation and do not include questions related to disfigurement, scarring, and worry about new lesions or recurrence. In the current study group of patients with BCC, itch correlated with impairment of QoL, and patients with BCC-associated itch had significantly higher DLQI scores in comparison with the non-itchy group. It is generally accepted that chronic itch is a debilitating symptom in the majority of patients with itch.
Fig. 2. Quality of life of patients with basal cell carcinoma (BCC) measured by the 36-item Short-Form Health Survey compared with a representative, normative sample of the French population (34). PF: physical functioning; RP: role limitation-physical functioning; BP: bodily pain; GH: general health; V: vitality; SF: social functioning; RE: Role limitation-emotional functioning; MH: mental health.
According to the SF-36 general health questionnaire scores, the patients with BCC, in general, had greatly reduced general health perception compared with the normative population (34) (Fig. 1). There are several studies measuring SF-36 in NMSC (Table III). Rhee et al. (35), in 2004, assessed 121 consecutive patients with NMSC who were referred to the dermatological surgery clinic, of whom 103 (85%) had histologically confirmed BCC. There were no significant differences compared with the general population. Maciel et al. (36), in 2014, assessed 50 patients with head or neck NMSC, of whom 43 were BCC (86.4%). In the 5-year follow-up, there was a significant improvement in the MH domain of SF-36, compared with the preoperative assessment. More recently, Dos Santos Tejada et al. (37) in 2018 conducted a preliminary study on 52 patients with both benign and malignant skin lesions qualified to reconstructive surgery (18 with BCC; 34.6%). After the surgical intervention, significant improvement in QoL score in most SF-36 domains (emotional, physical, social, pain, general health, and mental health aspects) was noted. However, in this study, the mean size of the skin lesion was 6.8 cm, which may justify why the surgical intervention caused such significant improvement in several components of SF-36. In the current cohort of patients, it is notable that the intensity of itch affected both MHC and PHC. The lower the SF component, the shorter was the time until the patient decided to seek doctors’ help. Further studies assessing BCC-associated itch influence of diagnostic delay are required.
Table III. Comparison among the subscales of 36-item Short-Form Health Survey in patients with non-melanoma skin cancer (NMSC)
The BDI scores in the current study showed that more than 15% of patients with BCC may develop co-existence of depression. Prevalence of depression, although assessed with different methodology, in the general population in Poland was assessed as 3.0% (38). A higher prevalence of depression in patients with BCC in comparison with the normative population suggests that BCC might be a disease of risk for the development of this type of reactive disorder, similarly for other dermatoses, such as psoriasis (39), in which 16.9% of patients fulfilled the criteria suggesting depression. There was a clear link between the age of patients and the BDI score. What was surprising was that there was no association between itching and depression in the current study cohort of patients, in contrast to other itchy dermatoses. In atopic dermatitis (9), urticaria (40) or psoriasis (39) co-occurring disorders, such as depression, may be more frequent among patients with itch and, in turn, negative emotional states can intensify the condition (41, 42). The current results might be connected with the fact that itch in BCC is mostly localized (2), and the intensity of itch is much lower than in the previously mentioned dermatoses. Most researchers agree that itch may be a distressing factor, resulting in a higher probability of the development of depressive symptoms. Roberts et al. (43), in their study on 63 patients with NMSC, stated that 19% of the affected patients experienced significant levels of psychological distress. Furthermore, those who engaged in avoidant coping strategies (specifically behavioural avoidance) were more likely to experience distress. Fagundes et al. (44) suggested that, among patients with BCC who experienced a severe stressor in the past year, those who were emotionally maltreated by their caregivers in childhood were more likely to have poorer immune responses (reflected in lower levels of mRNA for CD25, CD3ε, ICAM-1, and CD68) to their BCC tumours. Emotional maltreatment by the father was also linked to higher depressive symptoms. However, depressive symptoms and a history of depression were not linked to the BCC immune responses related to the BCC tumour. Stress, especially early in life, can impact tumour growth and progression, especially when exposed to an additional stressor in adulthood (45).
The stigmatization level among patients with BCC was also quite low. An analysis was performed concerning the level of stigmatization in the context of selected clinical and demographic parameters and, surprisingly, no significant relationship with all of the studied characteristics was found. It was unexpected to find that the presence of the lesion on the face or scalp area did not influence patients’ feelings of stigma. This might be connected to the fact that the development of the BCC is very slow, and the patient’s family and friends are more used to the age-related changes in the patient’s appearance. For now, there is a lack of studies concerning the subject of stigmatization, not only in BCC, but also in any other skin tumours (46, 47).
This study has some limitations. First, it was a single-centre study and the number of subjects with itch was relatively small. Therefore, the study should be considered exploratory. Secondly, the study population was a relatively homogenous elderly group, which makes it more difficult to generalize to other patient populations. Thirdly, the QoL of our patients was measured with a DLQI. Itch-specific instruments, such as ItchQoL scale, should be used in further studies on itch impact on QoL in patients with BCC.
Moreover, not all of the included patients completed all of the questionnaires. Last, but by no means least, the questionnaire was not administered to the patients during the follow-up after surgery; therefore the potential itch alleviation after treatment was not explored. Further studies concerning that topic are necessary.
In conclusion, this prospective study on patients with BCC found a slight impact of the disease on QoL; however, the presence and the intensity of itch may diminish QoL among affected subjects. Further studies exploring the potential impact of itch on diagnostic delay are required, as well as detailed studies with prolonged follow-up focusing on changes in itch after successful treatment of BCC.


 Click to show fullsize
Click to show fullsize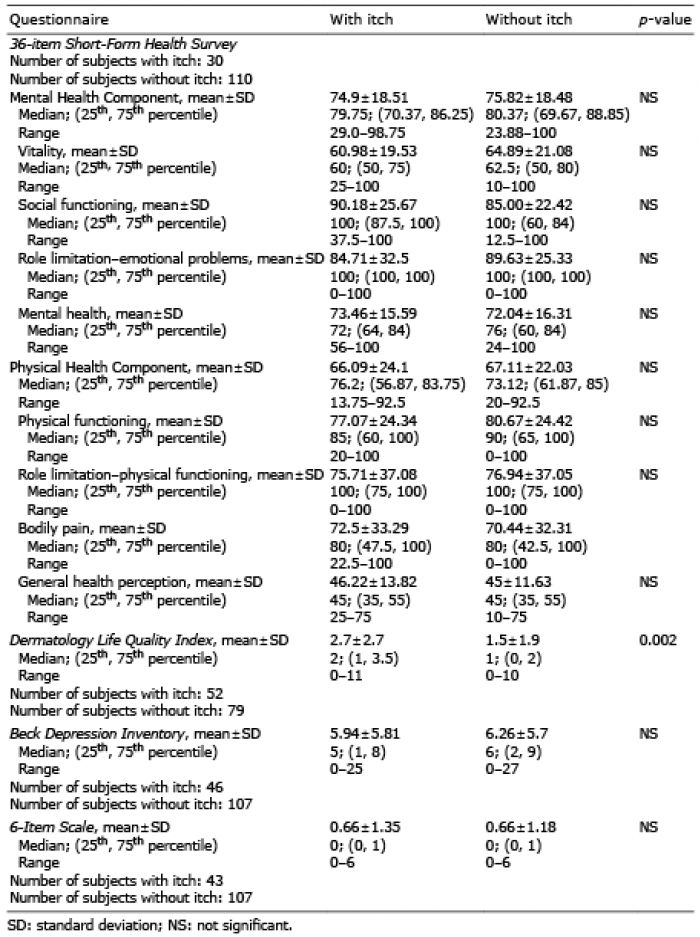 Click to show fullsize
Click to show fullsize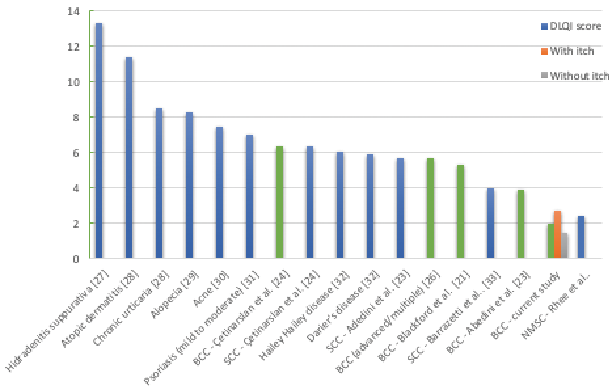 Click to show fullsize
Click to show fullsize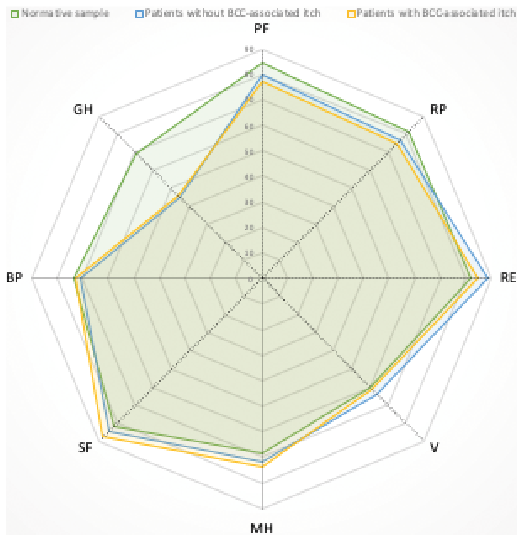 Click to show fullsize
Click to show fullsize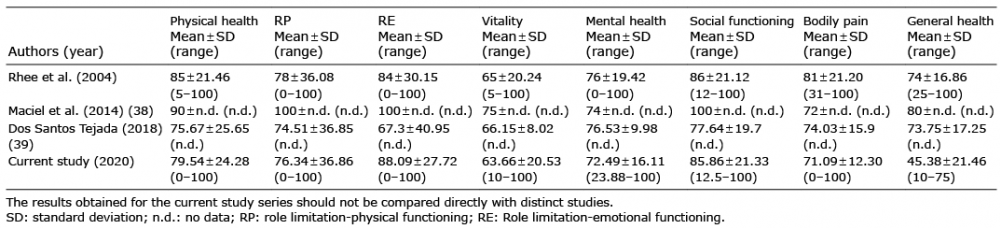 Click to show fullsize
Click to show fullsize