


1Department of Dermatology, Changwon Fatima Hospital, Changwon, and 2Department of Dermatology, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
There have been no epidemiological studies identifying associations between systemic inflammatory diseases and actinic keratosis. This study used a large nationwide database to investigate the associations between actinic keratosis and systemic inflammatory diseases. Records of patients over 20 years of age newly diagnosed with actinic keratosis (n = 64,659) from 2012 to 2017 were analysed. A control population of individuals without actinic keratosis, matched for age, sex, and year of claim, who visited an outpatient clinic, was sampled at a ratio of 1:1 (n = 64,659). Both cohorts were analysed for the presence of systemic inflammatory diseases within at least 5 years prior to diagnosis of actinic keratosis. Patients with actinic keratosis exhibited higher odds ratios for rheumatoid arthritis (1.336; 95% confidence interval (95% CI) 1.161–1.537)) and psoriasis (1.513; 95% CI 1.435–1.595) compared with the control group on multivariate analysis. However, the proportions of Behçet’s disease, Crohn’s disease, ulcerative colitis, and multiple sclerosis in the actinic keratosis group were not statistically significant.
Key words: actinic keratosis; psoriasis; rheumatoid arthritis.
Accepted Jul 14, 2021; Epub ahead of print Jul 15, 2021
Acta Derm Venereol 2021; 101: adv00510.
doi: 10.2340/00015555-3877
Corr: Young Bok Lee, Department of Dermatology, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 271 Chunbo Street, Uijeongbu 07345, Republic of Korea. E-mail: lyb80@catholic.ac.kr
The main mechanisms involved in the onset of actinic keratosis include ultraviolet-induced mutated keratinocytes and dermal inflammation. There have been no epidemiological studies identifying associations between systemic inflammatory diseases and actinic keratosis. In the current study, the population diagnosed with actinic keratosis and the control population without actinic keratosis were compared. The prevalence of rheumatoid arthritis and psoriasis was significantly higher in the actinic keratosis group than the control group. However, the proportions of Behçet’s disease, Crohn’s disease, ulcerative colitis, and multiple sclerosis in the actinic keratosis group were not statistically significant.
Actinic keratosis (AK) is a common premalignant skin disorder among elderly people, characterized by transformed keratinocyte proliferation and chronic inflammation due to chronic exposure to ultraviolet (UV). The incidence of AK in Korea has increased from 19.57 per 100,000 person-years in 2006 to 52.86 per 100,000 person-years in 2015 (1). AK can develop into invasive squamous cell carcinoma (SCC) through mutations of oncogenes and immunosuppressive genes, including ultraviolet B (UVB)-induced p53 tumour-suppressor gene mutations, which are found in cases of AK (2).
Although AK is caused mainly by UV-induced DNA damage, UV-induced inflammation and immunosuppression also play a role in the pathogenesis of AK (3). UV-induced aberrant over-expression of COX-2 mediates dermal inflammation and promotes tumour growth by enhancing tumour cell proliferation, stimulating angiogenesis, and inhibiting apoptosis (4). The fact that topical non-steroidal anti-inflammatory drug (NSAID) diclofenac is used for treatment of AK by downregulating COX-2 enzymes supports its key role of inflammation in AK (4). Other than diclofenac, regular use of low-dose aspirin or non-aspirin NSAIDs is reported to be associated with significantly lower counts of AKs (5). The chronic inflammation and up-regulation of proinflammatory cytokines in AK suggest a need for studies on the associations between systemic inflammatory diseases and AK (6). Until now, not many studies have been performed on the comorbidities of patients with AK (1, 7, 8).
The current study aimed to find the associations between AK and systemic inflammatory diseases, including rheumatoid arthritis (RA), psoriasis, Behçet’s disease, Crohn’s disease, ulcerative colitis, and multiple sclerosis.
This study adopted a nationwide population-based cohort design to analyse data from the National Health Insurance Research Database in Korea.
Study design and database
This study used data from the Korean Health Insurance Review and Assessment (HIRA) Service claims database from 2007 to 2017. The Korean government operates a mandatory nationwide insurance service with an HIRA database containing all claims data covering the entire population of Korea (>50 million). Medical institutions electronically submit healthcare utilization information for reimbursement purposes, and this information is integrated into the HIRA claims database. This nationwide, population-based retrospective cohort study used HIRA database diagnoses according to the International Classification of Disease, Tenth Revision (ICD-10) codes. The study was approved by the Institutional Review Board at Uijeongbu St. Mary’s Hospital, Catholic University of Korea (UC19ZEISI0017) and was conducted according to the principles of the Declaration of Helsinki. All identifiable personal information in the medical records was de-identified to comply with the privacy rule of the Health Insurance Portability and Accountability Act. Since the information used for analyses from the HIRA database was encrypted, anonymized, and de-identified, informed consent was not required.
Study population
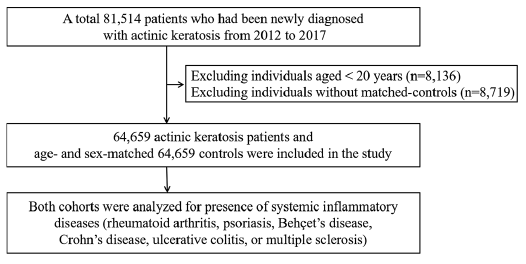
Inclusion criteria were: all patients newly diagnosed with AK (ICD-10 code L57.0) between January 2012 and December 2017 (n = 81,514) who had not been diagnosed with AK at least 5 years before enrollment (Table SI). Of these patients, those younger than 20 years were excluded (n = 8,136). For the control cohort, an age-, sex-, index year-matched control without AK was extracted during the same period with a ratio of 1:1 (n = 64,659) (Fig. 1). Individuals without matched-controls were excluded (n = 8,719).
Concurrent inflammatory diseases in both the AK group and control group
The presence of inflammatory diseases was defined as a visit to an outpatient clinic or admission with a main diagnosis of inflammatory diseases within at least 5 years prior to diagnosis of AK, starting in 2007. ICD-10 codes for inflammatory diseases are as follows: RA, M05; Psoriasis, L40; Behçet’s disease, M35.2; Crohn’s disease, K50; Ulcerative colitis, K51; and Multiple sclerosis, G35.
For adjustments, the presence of comorbidities was defined as a visit to an outpatient clinic, or admission with a diagnosis of ICD-10 code of diabetes mellitus (E11-14 with antidiabetic medications), hypertension (I10–13 and I15 with antihypertensive medications), or dyslipidaemia (E78 with antihyperlipidaemic medications) with the same period of 5 years prior to AK diagnosis.
Statistical analysis
It was expected that chronic diseases, such as diabetes mellitus, hypertension, and dyslipidaemia, would be possible confounders, and they were adjusted for in the analyses. Associations among AK and other inflammatory diseases were analysed using multiple logistic regression models and odds ratios (OR). The 95% CI was presented with the adjustment models. To evaluate the robustness of the associations, subgroup analyses were performed separately for age, sex, and comorbidities of diabetes mellitus, hypertension, and dyslipidaemia. The standardized rates for estimation of the prevalence and incidence of actinic keratosis were calculated after standardizing by age and sex, based on the 2010 Korean Census population. All statistical analyses were performed using SAS software (ver. 9.4; SAS Institute, Cary, NC, USA).
Fig. 1. Study population.
Characteristics of the study population
Among the 64,659 individuals, 35,437 were female (54.81%) and 29,222 were male (45.19%). The mean ± standard deviation (SD) age was 62.44 ± 15.52 years, with 63.29% of participants were over 60 years of age. Since a control group was extracted matched for age, sex, and year of claim, the characteristics of the control group were the same as those of the AK group (Table I).
Table I. Demographics of the study population
Positive associations between RA/psoriasis and AK
The analysis of claims data entered from 2007 to 2017 at least 5 years prior to baseline showed a proportion for RA (0.71%) and psoriasis (5.64%) in the AK group that was significantly higher than in the control group (0.54 and 3.82%, respectively). Among the comorbid diseases, diabetes mellitus was significantly higher in the AK group (Table I).
ORs for RA and psoriasis in the AK group were 1.334 (95% CI 1.160–1.534; p < 0.001). and 1.509 (95% CI 1.432–1.591; p < 0.001), respectively. Increased ORs for RA and psoriasis in the AK group were consistent after adjustments for other comorbid diseases (Table II). The proportions of Behçet’s disease, Crohn’s disease, ulcerative colitis, and multiple sclerosis were not significant.
Table II. Odds ratios (ORs) for rheumatoid arthritis (RA), psoriasis, ulcerative colitis (UC), Behçet’s disease (BD), Crohn’s disease (CD), and multiple sclerosis (MS) in patients with actinic keratosis
Subgroup analysis
The ORs for RA and psoriasis were further analysed according to age, sex, and the presence of diabetes mellitus, hypertension, and dyslipidaemia (Fig. 2).
Fig. 2. Subgroup analysis by age, sex, and the presence of comorbid diseases. Odds ratios for rheumatoid arthritis and psoriasis in patients with actinic keratosis. 95% CI: 95% confidence interval.
The increased proportion of RA and psoriasis in patients with AK persisted after subgroup analyses, except for the group ages less than 60 years who had an OR of RA with a value below 1.0 (OR 0.81, 95% CI 0.58–1.13).
To our knowledge, this is the first epidemiological study to investigate the associations between systemic inflammatory diseases and AK based on a large nationwide database. One of the most critical limitations of this study was the lack of information on UV exposure, phototype and use of immunosuppressive drugs. However, the results of the study showing the increased ORs for rheumatoid arthritis and psoriasis in patients with AK demonstrates that rheumatoid arthritis/psoriasis and AK are associated with each other and may share some pathogenic features. Increased ORs for rheumatoid arthritis and psoriasis in the AK group persisted after subgroup analyses and they were consistent after adjustments for comorbid metabolic diseases, which are frequent in older ages.
The main mechanisms of AK development are inflammation, immunosuppression, mutagenesis, oxidative stress, cell cycle deregulation and cell proliferation, impaired apoptosis, and human papillomavirus (HPV) (9). The first possible link between rheumatoid arthritis and AK was identified in human papillomavirus (HPV), regarded as a co-carcinogen in the development of AK. In patients with AK, E6 and E7 proteins of HPV prevent apoptosis in a p53-independent manner (10). Apoptosis-resistant cells are subject to additional UV-induced DNA damage accumulation, leading to unregulated cell proliferation (10). Furthermore, E6 protein can downregulate the expression of interleukin (IL)-8 in primary keratinocytes, which weakens the response to UV-induced DNA damage (10). In patients with rheumatoid arthritis, HPV infection is considered to affect RA through cross-reactions between self-antigens, viral proteins, and telomere shortening (11). The HPV-infected group exhibited a higher incidence density of RA compared with non-HPV controls in a recent Taiwanese nationwide cohort study (11). Since RA is postulated to result from immunosenescence through various mechanisms, including telomere shortening, HPV E6 and E7 protein-induced telomere shortening may be a mechanism in RA development following HPV infection (11).
The second possible link between rheumatoid arthritis and AK is the increased expression of proinflammatory cytokines (IL-1, IL-6, and tumour necrosis factor (TNF)), which are involved in the pathophysiology of RA and AK. Release of these cytokines is induced by UV exposure, leading to changes in gene expression in patients with AK, and these cytokines show increased expression in RA synovium (10, 12). Among the biologic drugs targeting the molecules (TNF, IL1, and IL6) involved in the pathogenesis of RA, the TNFα inhibitor is reported to be an additive risk factor for development of non-melanoma skin cancer in patients with RA through immunosuppression. Development of AK after initiation of TNFα inhibitor for RA has been reported (13, 14). Further studies are required to clarify this issue.
The prevalence of psoriasis was also increased in patients with AK. The pathogenic mechanisms of the association between AK and psoriasis have yet to be established, but increased expression of proinflammatory cytokines, including IL-1, IL-6 and TNF, shown in AK has also been demonstrated in psoriasis to propagate chronic inflammation and promote keratinocyte proliferation (15, 16). In addition, high-dose psoralen UVA therapy used in the treatment of psoriasis has been reported to be associated with an increased risk of AK (17). Therefore, patients with psoriasis treated with psoralen-UV light therapy are at greater risk of AK compared with the average population. In addition, since natural sunlight has been used for decades to treat psoriasis through immunomodulatory mechanisms, patients with psoriasis tend to make more of an effort to be exposed to sunlight, and this high degree of sun exposure exposes the patients to a greater risk of development of AK.
This study had several limitations. First, sun exposure, phototype and occupational information were not available in the HIRA database. Secondly, we did not consider the immunosuppressive drugs used in systemic inflammatory diseases, which could act as a risk factor for AK by inducing immunosuppression. Thirdly, health-related habits, such as smoking status and alcohol consumption, which could influence the incidence of the diseases, were not available in the HIRA database. Smoking is a risk factor for RA, psoriasis, and AK (18, 19), and alcohol could enhance pro-inflammatory cytokine production in many cell types, leading to persistent systemic inflammation (20).
In spite of these limitations, this study has several strengths, including the relatively large sample size of the entire national population. The ORs for rheumatoid arthritis and psoriasis were high in patients with newly diagnosed AK. Physicians should be aware of the increased risks of these inflammatory diseases in their patients with AK and treatment should also take into account common concurrent inflammatory diseases. This study will broaden our knowledge in understanding the pathogenesis of AK. Further studies of the potential mechanisms underlying the association between RA/psoriasis and AK incidence are necessary.
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (NRF-2019R1F1A1056601).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize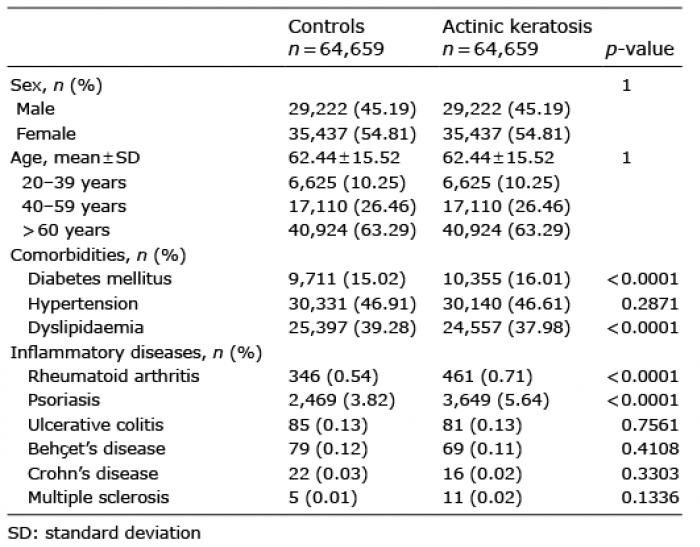 Click to show fullsize
Click to show fullsize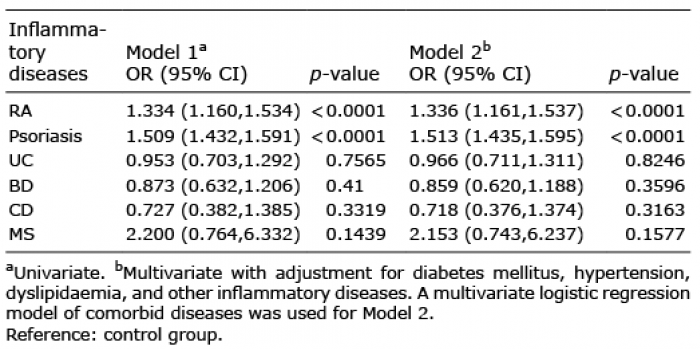 Click to show fullsize
Click to show fullsize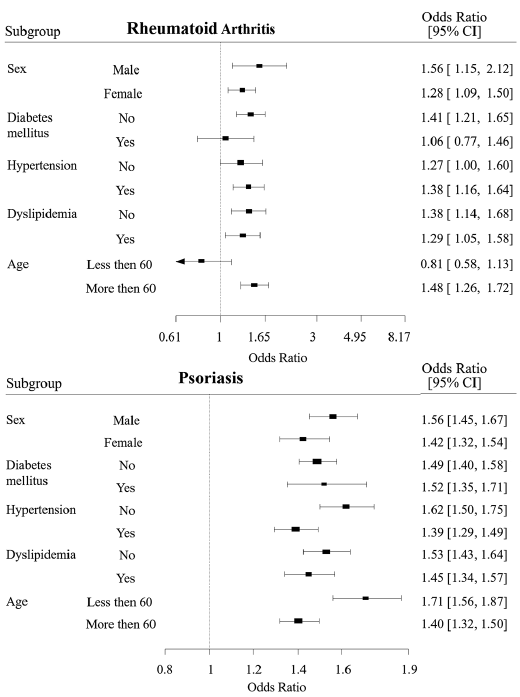 Click to show fullsize
Click to show fullsize