


Department of Dermatology and Venereology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
#These authors contributed equally to this work and should be considered co-first authors.
Port-wine stains are congenital vascular malformations that affect the quality of life of children and their parents. This study used the Family Dermatology Life Quality Index and Children’s Dermatology Life Quality Index to examine the effects of port-wine stains on the quality of life of children and their parents, including an in-depth, systematic analysis of the moderating effects of the children’s sex and port-wine stain classification. The study included 43 children (25 girls and 18 boys) and their parents. The presence of a port-wine stain had a significantly greater impact on the quality of life of mothers than on that of fathers (p < 0.001). Port-wine stains in girls had a greater effect on paternal quality of life than did port-wine stains in boys (girls p < 0.01; boys p = 0.542). Severe types of port-wine stains exerted a greater impact on maternal quality of life (pink-red type, dark-red type, and purple-dark type: p < 0.001, p = 0.948 and p = 0.086, respectively). Therefore, clinicians should consider familial relationships and differences when offering psychological support.
Key words: port-wine stains; quality of life; parents’ quality of life; Family Dermatology Life Quality Index.
Accepted Jul 14, 2021; Epub ahead of print Jul 15, 2021
Acta Derm Venereol 2021; 101: adv00516.
doi: 10.2340/00015555-3883
Corr: Jingjing Liu and Zhiming Li, Department of Dermatology and Venereology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325005, China. E-mails: liujingjing312@126.com, wzykdxlzm@163.com
Port-wine stains are congenital vascular malformations that have a negative impact on the quality of life of the affected child and their family members. This study examined the effects of port-wine stains on the quality of life of children and their parents, including an in-depth, systematic analysis of the moderating effects of the children’s sex and port-wine stain classification. It was found that both sex and port-wine stain classification were moderators of the effect of the children’s quality of life on their parents’ quality of life. Impaired quality of life in children with port-wine stain and their family members should be taken into account when offering psychological support.
Port-wine stains (PWS) are congenital benign vascular naevi, and 90% occur on the face (1). PWS are flat patches of erythema during infancy. However, the skin lesions turn from pink to purple with age and may form elevated vascular papules or nodules that lead to uncontrollable spontaneous bleeding (2). The colour of PWS can be categorized as pink-red, dark-red, or purple-dark, based on clinical manifestations (3). Various treatment methods are helpful for PWS and lead to a certain degree of improvement; these methods include topical antiangiogenic agents, cryotherapy, photodynamic therapy (PDT), and laser therapies (4).
Although it is generally believed that PWS are asymptomatic (no itching, pain, or significant dysfunction), their abnormal appearance and potential complications seriously negatively affect patients’ mental health (5, 6). Patients, especially paediatric patients, are the core of the family network in the medical context (7). Therefore, it is necessary to further examine the complicated relationship between children’s quality of life (QoL) and their parents’ QoL, in order to reveal the underlying mechanism and provide suggestions for improving parents’ QoL.
Several studies have focused on the impact of sex, disease type, severity, and comorbidities on the QoL of children with psoriasis and atopic dermatitis (AD) and on that of their families (8–12). However, no similar research into the psychosocial impact on the parents of children with PWS has been conducted to date. The current study used the Family Dermatology Life Quality Index (FDLQI) to assess parents’ QoL and examine the effects of PWS on the QoL of children and their parents, including an in-depth, systematic analysis of the moderating effects of the children’s sex and PWS classification.
This study was performed in children with PWS who were referred to the Dermatology Clinic of the First Affiliated Hospital of Wenzhou Medical University over a period of 2 years (from August 2018 to May 2021). The following inclusion criteria were used: a diagnosis of PWS confirmed by a professional dermatologist, based on typical clinical manifestations, an age between 4 and 16 years, consent of both parents for participation in the study, and the absence of other skin diseases or systemic diseases that might affect the study results. In addition, all children were raised by their parents rather than by other caregivers, such as grandparents. A total of 43 children with PWS (18 boys and 25 girls, mean age ± standard deviation (SD) 9.047 ± 3.817 years) and their parents (43 fathers and 43 mothers) were included. Clinicians classified PWS into pink-red type, dark-red type and purple-dark type according to their colour.
Each child’s father and mother completed the validated Chinese version of the FDLQI (from http://dermatology.org.uk/), which evaluates the influence of a patient’s skin condition on their parents/caregivers. A validation study involving 132 people found that the FDLQI had high internal consistency (Cronbach’s α 0.88) and test–retest reliability (intraclass coefficient 0.94) (13). The FDLQI consists of 10 questions about the impact of a childhood condition on family members’ QoL over the preceding month. It covers emotions, health, social interactions, work, and several aspects of life and well-being. Each question is answered with 1 of the following 4 independent options, and the score for each question ranges from 0 to 3 points (0: completely irrelevant; 1: slightly relevant; 2: quite relevant; and 3: very relevant). The maximum FDLQI score is 30 points, with a higher score indicating a more noticeable impact on QoL.
The impact of PWS on children’s health was assessed using the Chinese version of the Children’s Dermatology Life Quality Index (CDLQI) (14) (sourced from http://dermatology.org.uk/). This questionnaire was validated in children aged 4–16 years, and the CDLQI score can range from 0 to 30 points. A higher score indicates more pronounced deterioration in QoL. The patients completed the questionnaire alone or with the assistance of parents, when necessary.
The Institutional Review Board approved the study. Signed informed consent forms were received from the parents.
Statistical analysis
Statistical analyses were performed using Statistica® 12.0 software for Windows. Data are presented as means and standard deviations (SDs) or as medians. Independent samples t-tests and χ2 tests were used for parametric and non-parametric analyses, respectively. Spearman’s correlation analysis was used to identify potential relationships. A p < 0.05 was considered statistically significant. Where appropriate, the Bonferroni correction for multiple comparisons was applied (in this case, a p < 0.05 was considered statistically significant), and Model 1 in Process 3.3 was used to test the moderating effects of sex and PWS classification.
Clinical characteristics of children with port-wine stain
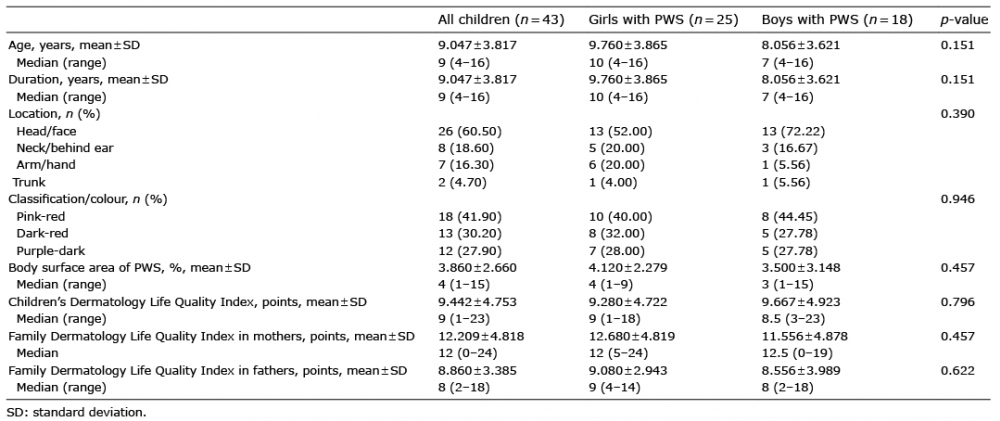
Twenty-five girls (58.1%) and 18 boys (41.9%) were included in the study (Table I). The mean age of the children with PWS was 9.047 ± 3.817 years, and the median age was 9 years. All skin lesions presented at birth, and the duration of the PWS ranged from 4 to 16 years. The skin lesions were on the head/face in 26 patients (60.50%), on the neck/behind the ears in 8 patients (18.60%), on the arms/hands in 7 patients (16.30%), and on the trunk in 2 patients (4.70%). Children had varying colour classifications of PWS: 18 (41.90%) patients had pink-red lesions, 13 (30.20%) patients had dark-red lesions, and 12 (27.90%) patients had purple-dark lesions. The mean affected body surface area (BSA) was 3.86 ± 2.66% (median 4%; range 1–15%). PWS significantly affected the children’s QoL; the mean CDLQI score was 9.442 ± 4.753 points (median 9 points; range 1–23 points). No significant differences were noted between boys and girls in age, duration, BSA, lesion location, skin colour, or reduction in QoL. Family members of 3 patients (6.98%) also had PWS. The mean FDLQI of all parents was 10.535 ± 4.469 points. The effect of PWS in children on the QoL of parents showed a significant difference in FDLQI scores between mothers (12.209 ± 4.818 points) and fathers (8.860 ± 3.385 points) p < 0.001), which indicated that the QoL of mothers was significantly worse than that of fathers.
Table I. Clinical characteristics of children with port-wine stain (PWS)
Correlation analysis of variables
Table II shows the correlation analysis results for each variable. A significant positive correlation was identified between the FDLQI scores of the mothers and fathers (r = 0.364, p < 0.05). In addition, the CDLQI scores of the children correlated positively with the FDLQI scores of the mothers (r = 0.440, p < 0.01), but not those of the fathers (r = 0.245, p = 0.113). Finally, the relationships between demographic variables and the CDLQI scores of children were examined. The impairment of children’s QoL was positively associated with the children’s age (r = 0.452, p < 0.01) and PWS classification (r = 0.311, p < 0.05). However, no correlations were found with the child’s sex, skin lesion location, mean BSA, or family history.
Table II. Correlation analyses of variables (n = 43)
Moderating effect of sex on the relationship between children’s Children’s Dermatology Life Quality Index scores and their parents’ Family Dermatology Life Quality Index scores
Analysis of the moderating effect showed that sex had a crucial moderating effect on the relationship between the children’s CDLQI scores and their fathers’ FDLQI scores (β = 0.677, t = 2.323, p < 0.05, 95% CI [0.087, 1.265]). In contrast, the moderating effect of sex on the relationship between the children’s CDLQI scores and their mothers’ FDLQI scores was not significant (β = –0.083, t = –0.286, p = 0.777, 95% CI [–0.667, 0.502]). The fathers’ FDLQI scores were divided into high and low groups, based on the mean ±1 SD to examine the difference in the moderating affect based on the sex of the children. Children were divided by sex into boys and girls. A moderating effect graph was constructed, and a simple slope test was performed. The regulating effect was not significant in boys (β = –0.135, t = –0.615, p = 0.542, 95% CI [–0.577, 0.308]), but was significant in girls (β = 0.542, t = 2.821, p < 0.01, 95% CI [0.153, 0.930]). The results are shown in Table SI and Fig. 1. These findings suggest that sex is a moderating factor in the relationship between children’s QoL and father’s QoL.
Fig. 1. Sex moderated the positive relationship between children’s Children’s Dermatology Life Quality Index (CDLQI) scores and fathers’ Family Dermatology Life Quality Index (FDLQI) scores (boys, p = 0.542; girls, p < 0.01).
Moderating effect of port-wine stain classification/colour on the relationship between children’s Children’s Dermatology Life Quality Index scores and their parents’ Family Dermatology Life Quality Index scores
Analysis of the moderating effect revealed that the PWS classification had a critical moderating effect on the relationship between the children’s CDLQI scores and their mothers’ FDLQI scores (β = –1.035, t = –2.821, p < 0.01, 95% CI [–1.778, –0.291]). However, no moderating effect was noted for the relationship between the children’s CDLQI scores and their fathers’ FDLQI scores (β = –0.175, t = –0.947, p = 0.350, 95% CI [–0.549, 0.199]). The children’s CDLQI scores were divided into 2 groups, based on the mean value ±1 SD to examine the effects of different PWS classifications. The lesions were divided by colour into pink-red, dark-red and purple-dark. A moderating effect graph was constructed, and a simple slope test was performed. The results showed that the moderating effect was significant for pink-red lesions (β = 1.016, t = 3.662, p < 0.001, 95% CI [0.544, 1.488]). In contrast, the moderating effect was not significant for dark-red lesions (β = –0.019, t = –0.066, p = 0.948, 95% CI [–0.593, 0.556]) or purple-dark lesions (β = 0.395, t = 1.765, p < 0.086, 95% CI [–0.059, 0.850]). The results are shown in Table SII and Fig. 2. These results indicate that PWS classification may be a moderating factor that affects the relationship between children’s and their mothers’ QoL.
Fig. 2. Different PWS classifications moderated the positive relationship between children’s Children’s Dermatology Life Quality Index (CDLQI) scores and mothers’ Family Dermatology Life Quality Index (FDLQI) scores (pink-red, dark-red, purple-dark: p < 0.001, p = 0.948 and p = 0.086, respectively).
To date, many studies reported that chronic skin conditions (such as psoriasis, AD, haemangioma, and vitiligo) in children have a substantial impact on the mental health and QoL of their parents and that there are differences in the psychological burdens of fathers and mothers (15–19). In the current study, the QoL of the parents of children with PWS was impaired, and the mothers were more severely affected than the fathers, see above, findings similar to those in the studies mentioned above. In addition, it was observed that, when the impairment of the children’s QoL was severe, the FDLQI scores of their mothers, but not those of their fathers, were increased significantly, suggesting that the decline in the children’s QoL would have a serious impact on the mothers’ life and work. This finding is consistent with that of the study by Marciniak et al. (20), who found that, among 50 children with AD and their parents in Poland, the mothers spent more time caring for their children and took on more family responsibilities than the fathers, which negatively impacted numerous aspects of the mothers’ lives. These results are not surprising. In Chinese culture and tradition, mothers primarily care for the family, and fathers are primarily responsible for supporting the family financially. Therefore, mothers often have a closer emotional connection with their children and are more negatively impacted by problems experienced by the children than are fathers. To maintain the family’s physical and mental health, parents, especially mothers, should be aware of their own emotions in addition to their children’s health. Strategies to enhance their QoL that involve leisure, entertainment, and social interactions can be implemented promptly.
Another interesting finding was that both the children’s age and PWS classification correlated positively with the CDLQI score, indicating that children’s QoL was more affected as they got older or the colour of the skin lesions deepened. Wang et al. (6) made similar findings in 197 Chinese people with PWS, and found that their QoL was significantly impaired, and the impairment of their QoL was related to sex, age, lesion size, and lesion location. This finding may be due to the fact that PWS is a congenital condition that affects individuals’ appearance and is associated with social stigma; the colour of the PWS has a well-established negative influence on the QoL of affected children. When the patient is young and has less social exposure, this asymptomatic condition does not cause inconvenience. However, the unique appearance of the lesion affects the child’s self-esteem and emotional and psychological development as the patient ages and matures, which subsequently affect all aspects of daily life (21).
Sex is an essential factor affecting QoL in patients with skin conditions that affect appearance. Women with psoriasis were found to have higher expectations and more specific needs for treatment than men (22). Women had low self-esteem because it was difficult to hide the affected area. Some of our observations verified the moderating effect of sex on the relationship between the children’s CDLQI scores and the fathers’ FDLQI scores. The QoL of fathers decreased significantly when the QoL of girls decreased, while there was no such relationship between boys and fathers, consistent with previous studies. ?ychowska et al. (8) performed a study with 65 children with psoriasis, and discovered that, compared with boys’ caregivers, girls’ caregivers were more likely to think that other people paid attention to the skin lesions, causing substantial distress. Chernyshov (23) investigated 50 children with AD and concluded that AD imposed a significant burden on the patients’ QoL and the quality of family life when the patients were female, and these effects were particularly strong for “child’s mood” and “sleep disturbances”. These results suggest that parents pay more attention to girls’ appearance and care more about girls, reflecting the differences in the methods of parenting girls and boys that have existed throughout history. Compared with the relatively caring method of parenting girls, parents tend to adopt a laissez-faire attitude to raising boys. Boys receive less care and supervision from their parents, especially their fathers. Parents of boys should eliminate this prejudice and give boys more care and attention.
The type and severity of disease appears to play a critical role in the impact of children’s QoL on their parents’ QoL. Indeed, Putterman et al. (24) found that impaired parental QoL was related to the severity of the disease, after investigating 153 children with alopecia areata. In the current study, PWS were divided into pink-red, dark-red and purple-dark, according to lesion colour, which was an indicator of severity. Differences were observed in PWS classification in terms of the effect of children’s PWS on their caregivers’ QoL. When the child’s skin lesions were pink-red, with the decrease in the child’s QoL (the increase in the child’s CDLQI score), the mother’s QoL tended to decrease more obviously. On the other hand, when a child had dark-red or purple-dark skin lesions that were more difficult to treat, regardless of whether the child’s QoL was high or low, it severely affected the mother’s own life. As the child’s supporter and primary caregiver, the mother felt responsible for the condition, which led to a more substantial psychological burden. Therefore, treatments that can lighten skin lesions and slow disease progression are needed. Parents should be aware of the importance of early treatment of the condition and cooperate actively with doctors. Clinicians should provide patients and their parents with supportive strategies that can guide treatment. Focus should be placed on lightening the colour of PWS in preschool children to reduce the imposed social and psychological burdens and improve their parents’ mental health.
Overall, the clinical significance of these findings lies at the intersection between psychology and dermatology. Both sex and PWS classification can moderate the impact of affected children’s QoL on their parents’ QoL. When clinicians develop education and treatment plans for patients and their families, they should be aware that the child’s sex and PWS classification can predict the effect on the parents’ QoL and should pay attention to strengthening their communication and providing education. For families with severely impaired QoL, appropriate support and treatment should be provided in a timely manner to help parents adjust their expectations and manage the condition.
Study limitations
This study has some limitations. Due to the rarity of the condition and parents’ unwillingness to participate, the sample size was relatively small. Difficulties were encountered in recruiting children with PWS and in having both parents complete the questionnaires about their mental health. Therefore, a larger study population is needed to confirm these observations. The research was performed in a single centre, and the cultural background of the research subjects was the same. Thus, these results may not be generalizable to other countries or cultures with different family models or division of parental roles.
This work was supported by the National Natural Scientific Fund of China [grant numbers 81703105, 81772904].
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize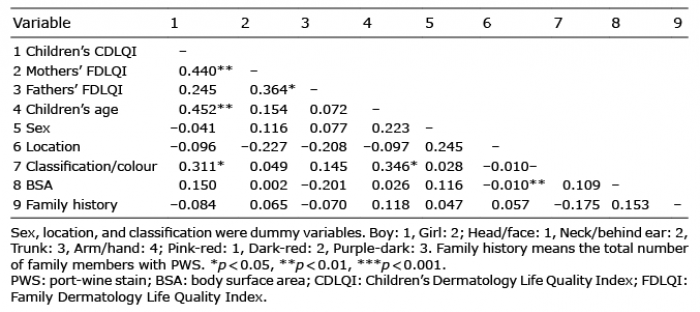 Click to show fullsize
Click to show fullsize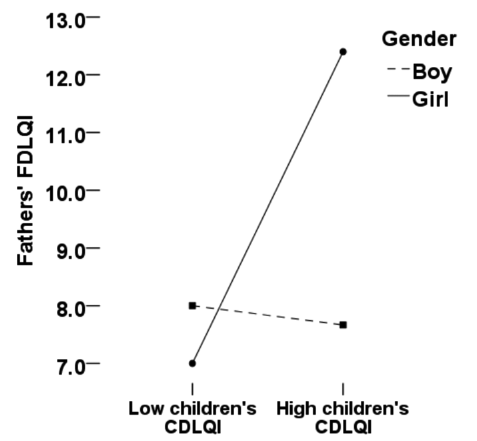 Click to show fullsize
Click to show fullsize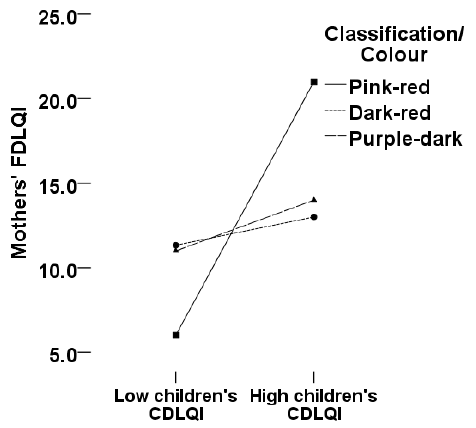 Click to show fullsize
Click to show fullsize