


Department of Dermatology, Venereology and Allergology, Paediatric Dermatology Outpatient Department, Charité – Universitätsmedizin Berlin, Charitéplatz 1, DE-10117 Berlin, Germany. E-mail: ulrike.blume-peytavi@charite.de
A 7-year-old German boy was referred for specialized paediatric dermatological consultation due to recurring pruriginous papules after exposure to sunlight. His family history revealed similar symptoms in his 23-year-old sister, starting at 17 years of age.
Both siblings experienced strong itching directly after sun exposure, followed by the appearance of multiple erythematous papules, with a symmetrical pattern limited to the sun-exposed skin, on the forehead, cheeks, forearms and hands (Figs 1 and 2).
Clinical examination revealed occasional superficial scarring, erosions and lichenification of the forearms, as well as an actinic cheilitis in both patients. The symptoms were reported to begin in spring and persist over the summer, with resolution in the autumn.
Based on the familial occurrence, patients’ history and clinical symptoms, we assumed a photodermatosis with genetic susceptibility. Phototesting of the older sibling revealed reduced minimal erythema doses after exposure to ultraviolet A (UVA), but not UVB. Human leukocyte antigen (HLA) typing, conducted on both siblings, showed positivity for the HLA-DR4 antigen.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical examination of a 7-year-old boy showing papulonodular lesions and erosions in the sun-exposed areas, including the face, cheilitis of the lower lip and residual scarring of the dorsal hands. Patients permission is given to publish this photos.
Fig. 2. The 23-year-old sister presented residual lesions in the sun-exposed areas including scarring of forehead and forearms and post-inflammatory hyperpigmentation of the dorsal hands and cleavage. Patients permission is given to publish this photos.
Acta Derm Venereol 2021; 101: adv00513.
Diagnosis: Actinic prurigo
Actinic prurigo (AP) is an idiopathic photosensitivity disorder with typical onset in childhood, although it may have an onset at any age. AP is commonly observed in Indian populations of North and Latin America, especially in individuals with mixed American-Indian and European ancestry, while it occurs sporadically in Europe and Asia. Females are 5–7 times more often affected than males (1). The lesions are typically induced by exposure to ultraviolet (UV) radiation. Both UVA and UVB have been implicated; however, UVA wavelengths elicit disease in most patients (2). Clinical manifestation is represented by itchy papulonodular lesions on the sun-exposed skin, which arise shortly after sun exposure and exhibit a tendency to chronicity, sometimes even persisting in winter. Mucosal and conjunctival involvement is a distinguishing feature of the disease, and is more common in Amerindian populations. Other clinical features include excoriation, scarring and frequent involvement of both exposed and covered sites (3). HLA typing often reveals positivity for the DR4 allele, in particular with the rare subtype DRB1*0407, thus suggesting an autoimmune basis for the disorder (4).
Differential diagnoses comprise other idiopathic photodermatoses, as well as erythropoietic protoporphyria (EPP) and X-linked protoporphyria (XLP).
AP presents similarities with polymorphic light eruption (PMLE), which is the most common photodermatosis in paediatric patients (5). Lesions in PMLE typically manifest hours after UV or sun exposure, rarely involving the face and the dorsal hands, and usually resolving without scarring (6). PMLE has no HLA association, although familial occurrence is often described (3). A clinical variant of PMLE is represented by juvenile spring eruption, which mostly occurs in childhood. Skin lesions include erythematous scaly papules and vesicles, characteristically involving the helices of the ears (7).
Another important differential diagnosis is represented by hydroa vacciniforme (HV), characterized by vesicular lesions and ulcerations, most commonly of the face and dorsal hands within hours of sun exposure, usually resulting in depressed scars (8). HV has been associated with chronic Epstein-Barr virus (EBV) infection (9).
Finally, porphyrin analyses are required to exclude EPP and XLP, which also present acute non-blistering eruptions within minutes after sun exposure (10). Measurement of total erythrocyte protoporphyrin (with fractionation, if elevated) is required for diagnosis, whereas urine porphyrins are not usually elevated. Both EBV serology and porphyrin analyses proved negative in the current patients.
Therapeutic options for AP comprise topical glucocorticoids, phototherapy and oral thalidomide. Antimalarials have been used successfully in PMLE; however, controversial reports could not lead to a recommendation for hydroxychloroquine in AP. Parents should be advised on the importance of sunlight avoidance as a preventive measure (11).
Intermittent courses of topical clobetasol represent an effective alternative to systemic therapy (12). Light hardening with narrowband UVB or psoralen plus UVA leads to increased tolerance of sun exposure; however, symptoms usually recur when treatment is discontinued (13, 14).
The efficacy of thalidomide has been proven in several case reports, with initial daily doses of 50–100 mg/day and subsequent tapering to the lowest dose able to control symptoms (15). Some patients remain symptom-free even after discontinuing thalidomide therapy. However, side-effects, such as sedation, peripheral neuropathy and teratogenicity, must be taken into account, and adequate contraception must be ensured in women of child-bearing age.
Intermittent topical treatment with class III–IV glucocorticoids proved effective in controlling symptoms in the younger male sibling during spring and summer. However, in the older female sibling topical glucocorticoids showed only moderate clinical improvement with immediate relapse shortly after discontinuing application. Thus, after excluding pregnancy and under safe contraception, a systemic therapy with thalidomide was initiated under careful clinical observation for potential side-effects. Both skin eruptions and itching after sun exposure improved significantly within 4–8 weeks of treatment. Thalidomide intake was performed successfully during spring and summer and discontinued in autumn and winter with no relapses.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize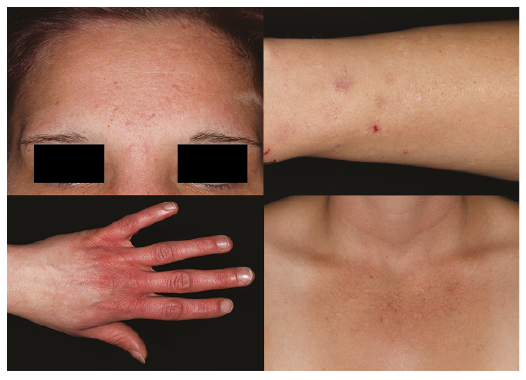 Click to show fullsize
Click to show fullsize