


1Department of Dermatology, 2Institute for Transfusion Medicine and Cell Therapy, University of Muenster, 3Central Laboratory Facility, University Hospital Muenster, Muenster, 4Institute of Pathology, Heidelberg University Hospital Heidelberg, Heidelberg, Germany, 5Department of Biological and Geographical Sciences, University of Huddersfield, Huddersfield, UK, 6Cologne Center for Genomics, University of Cologne, Cologne, Germany, 7Department of Biology, Edge Hill University, Ormskirk, UK, 8Steroid Research and Mass Spectrometry Unit, Laboratory for Translational Hormone Analytics, Division of Pediatric Endocrinology and Diabetology, Center of Child and Adolescent Medicine, Justus Liebig University, Gießen, Germany, 9Instituto de Productos Lácteos de Asturias-Consejo Superior de Investigaciones Científicas (IPLA-CSIC), Villaviciosa, Spain, 10Institute of Biostatistics and Clinical Research, University of Muenster, Muenster, and 11Institute of Human Genetics, University Medical Center Freiburg, Freiburg, Germany
#Shared first-authorship.
Data on vitamin D status of patients with inherited ichthyosis in Europe is scarce and unspecific concerning the genetic subtype. This study determined serum levels of 25-hydroxyvitamin D3 (25(OH)D3) in 87 patients with ichthyosis; 69 patients were additionally analysed for parathyroid hormone. Vitamin D deficiency was pronounced in keratinopathic ichthyosis (n = 17; median 25(OH)D3: 10.5 ng/ml), harlequin ichthyosis (n = 2;7.0 ng/ml) and rare syndromic subtypes (n = 3; 7.0 ng/ml). Vitamin D levels were reduced in TG1-proficient lamellar ichthyosis (n = 15; 8.9 ng/ml), TG1-deficient lamellar ichthyosis (n = 12; 11.7 ng/ml), congenital ichthyosiform erythroderma (n = 13; 12.4 ng/ml), Netherton syndrome (n = 7; 10.7 ng/ml) and X-linked ichthyosis (n = 8; 13.9 ng/ml). In ichthyosis vulgaris 25(OH)D3 levels were higher (n = 10; 19.7 ng/ml). Parathyroid hormone was elevated in 12 patients. Low 25(OH)D3 levels were associated with high severity of scaling (p = 0.03) implicating scaling as a risk factor for vitamin D deficiency. Thus, this study supports our recent guidelines for ichthyoses, which recommend screening for and substituting of vitamin D deficiency.
Key words: ichthyosis; vitamin D deficiency; parathyroid hormone.
Accepted Aug 13, 2021; Epub ahead of print Aug 16, 2021
Acta Derm Venereol 2021; 101: adv00546.
doi: 10.2340/00015555-3887
Corr: Kira Süßmuth, University Hospital of Muenster, Department of Dermatology, Von-Esmarch-Str.58, DE-48149 Muenster, Germany. E-mail: Kira.Suessmuth@ukmuenster.de
This study collected clinical data for 87 patients with inherited ichthyoses, and analysed serum levels of 25-hydroxyvitamin D3 (25(OH)D3) and parathyroid hormone. These measurements were performed before routine substitution of vitamin D in ichthyoses. Vitamin D deficiency and insufficiency was highly prevalent in this study cohort. Less than 10% of the patients had sufficient vitamin D levels. Moreover, vitamin D deficiency was related to the clinical severity of scaling. Thus, this study supports our recent guidelines for ichthyoses, which recommend screening for and substituting of vitamin D deficiency.
Inherited ichthyoses are monogenic disorders of cornification, which are caused by genetic defects affecting the function of the epidermal barrier (1) and associated with increased transepidermal water loss (2). Homeostatic repair processes compensating for transepidermal water loss result in clinically pronounced scaling and hyperkeratosis and are associated with either epidermal hyperproliferation or with retention hyperkeratosis (1–3). Marked inflammation induced by barrier defects and by epidermal repair mechanisms is typical for most types of autosomal recessive congenital ichthyosis (ARCI), keratinopathic ichthyosis (KPI) including epidermolytic ichthyosis (EI) and superficial epidermolytic ichthyosis (SEI), and many syndromic forms, such as Netherton syndrome (NTS).
In humans, the epidermis is the major source of vitamin D production. It is synthesized photochemically from 7-dehydrocholesterol, which is an intermediate in the late steps of epidermal biosynthesis of cholesterol. Under the influence of UVB light 7-dehydrocholesterol is photolysed in a non-enzymatic reaction to previtamin D3 bound in the vessels of the dermis to vitamin D binding protein. From there it is transported to the liver, where it is transformed into 25-hydroxyvitamin D3 (25(OH)D3; cholecalciferol; vitamin D3). This metabolite is later transformed in the kidneys into 1α,25-dihydroxy-vitamin D3 (calcitriol), which is the biologically active form of vitamin D3 (4). The typical human manifestation of severe vitamin D deficiency is osteomalacia (5). Numerous medical conditions, ranging from cardiovascular problems to metabolic syndrome, certain types of cancer, proneness to infections, Alzheimer’s disease and atopic dermatitis have recently been linked to vitamin D deficiency. Vitamin D3 acts in humans as a prohormone and is relevant for innate and adaptive immunity (6). CAMP, encoding for the antimicrobial peptide cathelicidin, is a target gene, and its expression in human skin can be increased by topical application of vitamin D derivatives, such as calcipotriol (7, 8).
To date, data on vitamin D status in European patients with ichthyosis is scarce, and mostly unspecific concerning the genetic subtype. Single cases or a few selected patients have been studied. Manifestations of rickets after treatment with oral retinoids in children with lamellar ichthyosis have been reported (9–11). Furthermore, one study has systematically evaluated vitamin D status in a European cohort of patients with ichthyosis. This study also established that the severity of scaling acts as an independent risk factor, possibly by providing a physical blockade for ultraviolet (UV) light penetration (12). In an Indian cohort of patients with ichthyosis an association between highly pigmented skin (type IV and type V skin) and vitamin D deficiency was found (13).
It remains unknown which type of ichthyosis is the strongest risk factor for vitamin D deficiency. This observational, prospective monocentric study of 87 characterized patients with hereditary ichthyosis focussed especially on genetically defined ARCI. The study determined 25(OH)D3 serum levels in patients without vitamin D substitution. The study also analysed parathyroid hormone (PTH) to exclude alterations of vitamin D due to abnormal levels of PTH and to analyse whether patients with vitamin D deficiency show secondary hyperparathyroidism. The study also evaluated the importance of the severity of scaling as a possible independent risk factor in ichthyosis.
Study design
This is a prospective monocentric study, performed at the Department of Dermatology of the University Hospital of Muenster and its reference centre for genetic skin diseases. The centre was a member of the Network for Ichthyoses and Related Keratinization disorders (NIRK).
All investigations were carried out within the framework of NIRK, and approval was provided by the institutional review board (2XTrau1). In total, the study enrolled 87 patients, who underwent a careful clinical examination in the University Hospital of Muenster, Germany, by 2 expert dermatologists (H.T. and V.O.).
All patients were clinically studied regarding erythema, scored from absent to severe (0–3; 0: absent; 1: mild; 2: moderate; 3: severe). In order to characterize the severity of scaling we adapted a 5-point physician general assessment, as used in a clinical trial on lamellar ichthyosis (R00002CR301(ORF), www.clinicaltrialsregister.eu). This Scaling and Cornification Score in Ichthyosis (SCSI) encompasses the extent of cornification as well as affected body surface area (BSA) as published recently (Table SI) (14).
Genetic analysis
The patients underwent further diagnostic procedures to analyse the genetic subtypes of ichthyosis. Consequently, all patients diagnosed with ichthyosis vulgaris (IV) were analysed for filaggrin (FLG) gene mutations by restriction enzyme analysis as well as typical ultrastructural and/or immunohistological features (14, 15). In patients with X-linked ichthyosis (XLI), steroid sulphatase deficiency was confirmed by biochemical methods, that either included direct STS activity testing in blood or detection of typical metabolite profiles, such as high levels of oxysterol sulfates in serum (14,16). In patients with ARCI, skin biopsies were routinely taken, and cryosections were tested for transglutaminase-1 (TG1) deficiency by in situ monitoring of TG1 activity (17). In addition, genomic DNA from peripheral blood lymphocytes was isolated from most patients with ARCI, and PCR amplification, Sanger sequencing or NGS methods were performed (18). For the group with KPI, histology and/or ultrastructural characterization were performed to underline KRT1, KRT10 or KRT2 mutations (19). In patients with NTS the clinical diagnosis was confirmed by demonstrating LEKTI deficiency in immunohistology and by molecular analysis with detection of SPINK5 mutations (1). For all remaining cases, including keratitis ichthyosis deafness (KID) syndrome, genetic analyses were performed.
Serum analysis
To determine vitamin D status (serum concentrations of 25(OH)D3) and PTH levels, blood samples were collected from patients by venipuncture and centrifuged immediately. Sera were aliquoted, stored at −70°C and analysed in a routine hospital laboratory (Center for Laboratory Medicine, University Hospital Muenster) using commercially available immunoassays. Concentrations of 25(OH)D3 were determined using a competitive chemiluminescence immunoassay (CLIA, DiaSorin Deutschland, Dietzenbach, Germany) on a Liason automated analyser. The intra- and inter-assay variabilities were < 4.0% and < 7.0%, respectively. Concentrations of intact parathormone were determined using a direct CLIA (Siemens, Eschborn, Germany) on Immulite 2000 automated analyser. The intra- and inter-assay variabilities were < 4.2% and < 8.8%.
Vitamin D deficiency was defined as a serum level of 25(OH)D3 < 10 ng/ml and vitamin D insufficiency as a level of 10–29.9 ng/ml. A normal and sufficient level was defined as ≥ 30 ng/ml. Toxicity levels are ≥ 100 ng/ml. Hyperparathyroidism was defined as serum PTH level of ≥ 65 pg/ml. While vitamin D level was measured in all 87 patients, PTH levels were determined in only 69 patients. Insufficient PTH values were distributed evenly over all genetic subtypes.
Statistical analysis
All data analyses were performed with SPSS version 26, software for statistical analysis, for Windows and Excel. Continuous parameters were shown as median and range [minimum – maximum], and categorical parameters as absolute and relative frequencies. Group comparisons of continuous parameters were performed by Mann–Whitney U or Kruskal–Wallis test (> 2 groups). Correlations were assessed by Spearman’s rank correlation coefficient. Inferential statistics were intended to be exploratory and were interpreted accordingly. Two-sided p-values ≤ 0.05 were considered statistically significant.
Clinical data of the cohort
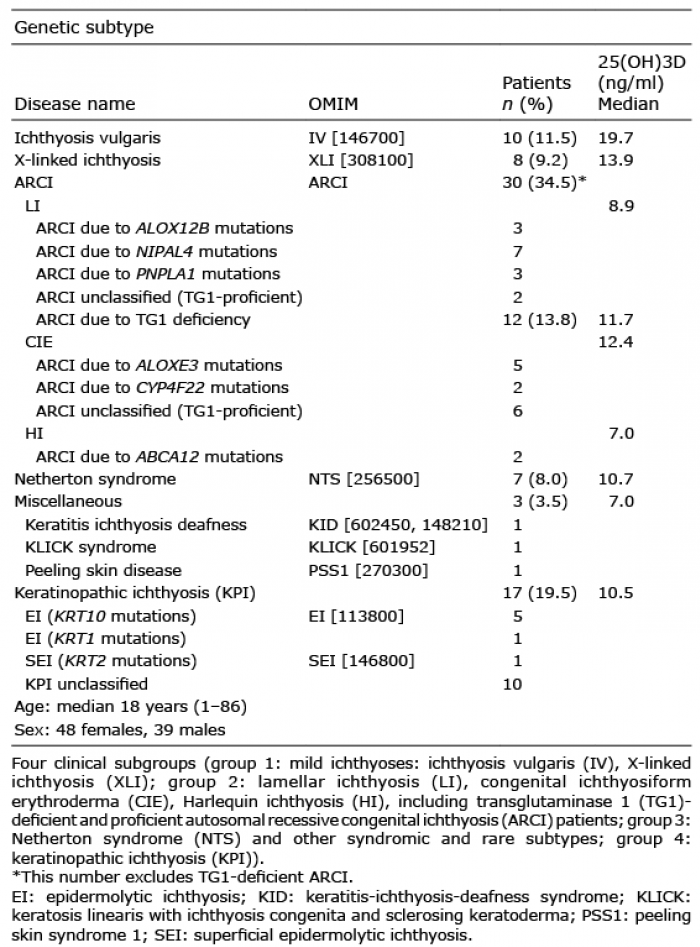
In the study cohort of 87 patients with ichthyosis, 10 patients had been diagnosed with IV, 8 with X-linked ichthyosis (XLI), 42 with ARCI, with 2 of them having the severe subtype of Harlequin ichthyosis (HI), 17 had KPI, and 7 NTS (Table I). Other diagnoses included KID syndrome (n = 1), Keratosis linearis-ichthyosis congenita-sclerosing keratoderma (KLICK) syndrome (n = 1), and peeling skin disease (n = 1). In the group with ARCI, 12 patients showed mutations in transglutaminase 1 (TGM1) (transglutaminase 1 (TG1) - deficient ARCI) and 22 patients had mutations in NIPAL4 (n = 7), ALOXE3 (n = 5), ALOX12B (n = 3), ABCA12 (n = 2), PNPLA1 (n = 3), or CYP4F22 (n = 2). From a clinical point of view, criteria can be used to distinguish between lamellar ichthyosis (LI) and congenital ichthyosiform erythroderma (CIE) within the group with ARCI: patients with LI were characterized by coarse lamellar scaling, CIE was defined by pronounced erythema and finer scaling. Fifteen patients in the current study cohort were categorized as having LI, and 13 patients as CIE. In 8 cases of the ARCI group the exact molecular cause could not be established, but the presence of TGM1 mutations had been excluded (TG1-proficient ARCI). In this group, 2 patients clinically showed LI and 6 patients had CIE. Patient age ranged from 1 to 86 years, with a median of 18 years. There were slightly more females (n = 48) than males (n = 39).
Table I. Genetic subtypes and demographic data of study cohort
Vitamin D and parathyroid hormone levels
In the study cohort, 32 patients showed 25(OH)D3 serum values regarded as vitamin D deficiency (median 7.0 ng/ml [7.0–9.2]), 49 subjects displayed insufficiency (median 15.2 ng/ml [10.2–29.2]) and 6 patients had vitamin D levels within the normal range (median 32.4 ng/ml [30.0–35.8]). The median 25(OH)D3 level of the entire study cohort was 12.6 ng/ml. Since normal serum 25(OH)D3 levels vary between 30.0 and 100.0 ng/ml, the data from this study generally showed that ichthyosis-affected individuals have a certain risk of either pronounced deficiency or at least insufficiency of vitamin D. A seasonal comparison of vitamin D levels indicated somewhat higher levels of 25(OH)D3 in the summer (median 13.25 ng/ml [7.0–35.8]) compared with measurements in the winter half-year (median 12.4 ng/ml [7.0–24.6]). This difference was not statistically significant (p = 0.272) and does not seem to be relevant from a clinical point of view.
The median serum PTH level for the total study cohort was 40.2 pg/ml. Most patients were within the normal range of 10.0–65.0 pg/ml. Of note, 12 patients showed increased PTH levels associated with deficient or insufficient vitamin D values (median 7.0 ng/ml [7.0–16.8]). These patients did not report any symptoms of hyperparathyroidism. They were not specifically checked for associated diseases by an endocrinologist; however, routine blood and serum parameters were within the normal range. Only one patient with IV showed a reduced PTH level (8.2 pg/ml). The vitamin D level of this patient was insufficient (21.4 ng/ml), regular blood and serum parameters were normal.
A slightly negative correlation was found between 25(OH)D3 and PTH levels (rs=–0.47). The distribution of vitamin D and PTH levels in relation to the severity of scaling are shown in Fig. 1. While higher SCSI scores were significantly associated with lower vitamin D levels (p = 0.03), the high SCSI scores were linked to increasing PTH level (p = 0.04). The extent of erythema tended to be associated with decreasing 25(OH)D3 and increasing PTH levels; however, the association was not significant and not strong (p = 0.32 and p = 0.17) (Table SI).
Fig. 1. Vitamin D, parathyroid hormone (PTH) levels and Scaling and Cornification Score in Ichthyosis (SCSI). (a) Boxplots of vitamin D (25(OH)D3) levels for different degrees of the Scaling and Cornification Score in Ichthyosis (SCSI) showing highest 25(OH)D3 levels in patients with low SCSI. Reference value for vitamin D sufficiency: ≥30 ng/ml. (b) Boxplots of PTH levels for different degrees of SCSI. High SCSI scores are associated with increased PTH levels. Normal range for PTH levels: 10–65 pg/ml.
Vitamin D status of ichthyosis subtypes
The distribution of 25(OH)D3 levels for different genetic subtypes of ichthyosis is shown in Fig. 2. The best vitamin D status was found in patients with a mild ichthyosis phenotype, such as IV. For this group (n = 10; 19.7 ng/ml [13.3–32.1]) only 50% of patients were vitamin D deficient. In XLI, usually presenting with a mild or moderate ichthyosis phenotype, 5 out of 8 patients exhibited deficient 25(OH)D3 levels (median 13.9 ng/ml [7.0–35.1]). Lowest 25(OH)D3 values were observed in patients with KPI (n = 17; median 10.5 ng/ml [7.0–21.3]) (Fig. 2). In this group only one patient showed a vitamin D status that was higher than 20 ng/ml. A pronounced deficiency was observed in patients with TG1-deficient lamellar ichthyosis (n = 12; median 11.7 ng/ml [7.0–32.6]) and NTS (n = 7; median 10.7 ng/ml [7.0–30.6]). In each of these groups, only one patient had a sufficient vitamin D level. The heterogeneous group of TG1-proficient ARCI, including LI with ALOX12B or NIPAL4 mutations and patients with CIE, but excluding HI patients showed a low vitamin D level (n = 28; median 11.15 ng/ml [7.0–35.8]). LI with other than TGM1 mutations usually show a milder phenotype compared with TG1-deficient lamellar ichthyosis (median SCSI: 2 vs 3). However, the median vitamin D level in this group was lower than in the TG1-deficient group (8.9 vs 11.7 ng/ml). In the group with ARCI, most severe vitamin D deficiency was observed in HI. Both patients with HI had a severity score of 4 points and showed the lowest vitamin D levels (both 7.0 ng/ml). PTH levels were the highest measured in our cohort (109 and 169 pg/ml) (Fig. 3).
Fig. 2. Vitamin D levels in genetic subtypes of ichthyosis. Keratinopathic ichthyosis (KPI), Harlequin ichthyosis (HI), lamellar ichthyosis (LI), Netherton syndrome (NTS) and other syndromic ichthyoses show lowest vitamin D values, patients with milder types of ichthyosis (ichthyosis vulgaris (IV), X-linked ichthyosis (XLI)) only have a moderate insufficiency. Reference value for vitamin D sufficiency ≥30 ng/ml. CIE: congenital ichthyosiform erythroderma; HI: Harlequin ichthyosis; ARCI: autosomal recessive congenital ichthyosis.
Fig. 3. Parathyroid hormone (PTH) levels in genetic subtypes of ichthyosis. PTH levels in genetic subtypes of ichthyosis, with highest PTH levels in patients with Harlequin ichthyosis. Normal range for PTH levels: 10–65 pg/ml. IV: ichthyosis vulgaris; XLI: X-linked ichthyosis: LI: lamellar ichthyosis; CIE: congenital ichthyosiform erythroderma; HI: Harlequin ichthyosis; ARCI: autosomal recessive congenital ichthyosis; KPI: keratinopathic ichthyosis; NTS: Netherton syndrome.
From a clinical point of view, the cohort was differentiated into 4 groups: group 1 (mild ichthyoses: IV, XLI); group 2 (LI, CIE, HI; including TG1-deficient and -proficient ARCI patients); group 3 (NTS and other syndromic and rare subtypes); group 4 (KPI) (Table I). A notable difference was found between these 4 groups regarding vitamin D status (17 vs 10.95 vs 9.5 vs 10.5 ng/ml; p = 0.01). The difference between these groups concerning PTH levels was not significant (35.3 vs 45.75 vs 44.1 vs 36.3 ng/ml; p = 0.11). There was no strong correlation between serum vitamin D levels and age (rs=–0.229) (Fig. S1).
Data on vitamin D status in inherited ichthyoses in Europe is rare. A study of 53 patients in France revealed that more than 80% of patients did not have an optimal vitamin D status. The study showed ichthyosis severity, dark skin, and winter/spring seasons as independent risk factors (12). In a recent Spanish study on malnutrition in 50 patients with ichthyosis vitamin D serum levels below the reference value were detected in only 22% of patients. However, 20% of patients had already received supplements, and the authors refer to the geographical location of their cohort. The authors could not show a correlation between insufficient vitamin D values and disease severity or undernutrition (20). To study the vitamin D status in ichthyosis, the current study further distinguished between genetic and clinical subtypes. Of note, 16 out of 17 patients with KPI had a highly severe vitamin D insufficiency or deficiency, and 1 patient had a moderate insufficiency. A large proportion of patients with TG1 deficiency with pronounced scaling and hyperkeratosis, as well as those with NTS with variable and (in most cases) mild to moderate scaling exhibited a marked deficiency of vitamin D. Vitamin D deficiency was present, but less significant, in the group with ARCI (23 out of 28 cases). Finally, vitamin D deficiency was less pronounced in clinically mild types of ichthyosis, such as IV and XLI. Nonetheless, even for IV it was established that half of the patients with FLG mutations had vitamin D deficiency. This is in contrast to a population study from Denmark and Germany, in which 9 compound heterozygous or homozygous carriers of FLG mutations had even higher 25(OH)D3 concentrations than the normal population (21). This discrepancy is surprising, but the clinical status of the 9 IV patients in the Danish population study was not described, and they were possibly less severely affected by scaling than the 10 patients in the current study cohort.
Similar to a previous French study (12), the current study observed that higher SCSI scores were associated with lower vitamin D levels (Fig. 1a). The study group included 7 patients with NTS who had a markedly lower median vitamin D level. These patients did not have severe scaling, but severe erythema (mean and median: 2). Concerning the severity of scaling, a median SCSI of 1 was observed for these patients compared with a median SCSI of 2 in other patients in the current cohort. These findings imply that erythroderma or skin inflammation may also contribute to vitamin D deficiency. Of note, a positive correlation was observed between SCSI and PTH levels, which is in line with an American study (22).
The influence of skin pigmentation was not analysed within the current study group, as the study included only patients with fair skin types (primarily type II and III). Data from patients with black skin types in India support the notion that ichthyosis of black skin represented a much higher risk for vitamin D deficiency (13).
To examine whether extremely high levels of PTH in patients with HI are a random finding, and to analyse possible causes for such high levels through screening of larger cohorts of HI for vitamin D serum levels and further endocrinological parameters are necessary.
In the literature there is a report on improvement of scaling after vitamin D supplementation in patients with ichthyosis and vitamin D deficiency (23). Since we have not systematically followed up our patients after beginning a vitamin D substitution, we need further studies to evaluate whether vitamin D substitution not only prevents secondary diseases but also has direct effects on scaling and inflammation of the skin.
The protective role of vitamin D is not yet fully understood. Although there are no international guidelines concerning vitamin D substitution as a prophylaxis against COVID-19 the Robert Koch Institute in Germany recommends vitamin D substitution for patients with deficient levels and higher risk for or active COVID-19 infections. This recommendation is based on the knowledge of an anti-inflammatory and immunomodulatory potential of vitamin D (24, 25). However, a causality is not proven, and a deficiency may be caused by inflammation and severe disease (26–28). There is still a need for clinical trials and studies analysing links between vitamin D deficiency and pathogenesis or worsening of disorders, especially infectious diseases.
We conclude that all patients with ichthyosis are at risk of having a deficient or insufficient level of vitamin D. This risk seems most pronounced in patients with KPI. Although we did not compare our data with an age- and sex-matched healthy control cohort, it is known that vitamin D deficiency is common in the German population. Data from the Robert Koch Institute revealed vitamin D deficiency in 30.2% of German adults between 18 and 79 years of age. Sufficient values (defined as > 50 nmol/l) were detected in 38.4% of the study population (29). Another study that examined vitamin D levels in patients ≤ 16 years with juvenile idiopathic arthritis detected sufficient serum values (defined as ≥ 30 ng/ml) in only 16.0% of healthy controls (30). Of note, in our cohort only 6.9% were measured as having sufficient serum levels.
The current study showed that the degree of scaling and cornification represents a risk factor for vitamin D deficiency. Avoidance of outdoor activity in patients with severe scaling and/or erythema and associated hypohidrosis may be considered as an additional explanation for low vitamin D status and minor differences in the values between the seasons.
In summary, measurement of vitamin D levels should be recommended in patients with ichthyoses, especially for individuals with severe scaling and cornification or inflammatory forms. This recommendation does not refer to distinct age groups. Monitoring of PTH levels and further endocrinological diagnostic may be considered only in patients with extremely low vitamin D status. Vitamin D supplementation for patients with insufficient or deficient vitamin D serum levels is recommended to prevent secondary diseases.
The authors thank the patients and the whole team of the Reference Center for Ichthyosis in Münster, including Brigitte Willis, Dieter Metze, Tatjana Tarinski. This study was supported by the Selbsthilfe Ichthyose e.V., the Medical Faculty of the University of Münster (OJI120817 & OJ111409) and of the German Research Foundation (DFG OJ 53/3-1). It is part of the medical thesis of Mi-Ran Kim.
The work was supported by the Selbsthilfe Ichthyose e.V., the Medical Faculty of the University of Muenster (OJI120817 & OJ111409) and by the German Research Foundation (DFG OJ 53/3-1). Furthermore, we cooperated with members of the European Reference Network (ERN, subgroup ERN-skin). The cohort of this paper was also part of a project funded by the programme “Innovative Medizinische Forschung” (IMF); project number: SÜ212007.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize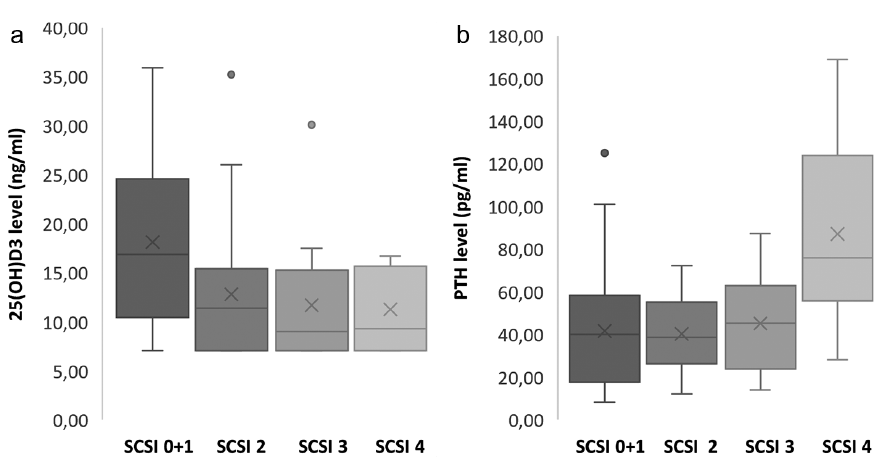 Click to show fullsize
Click to show fullsize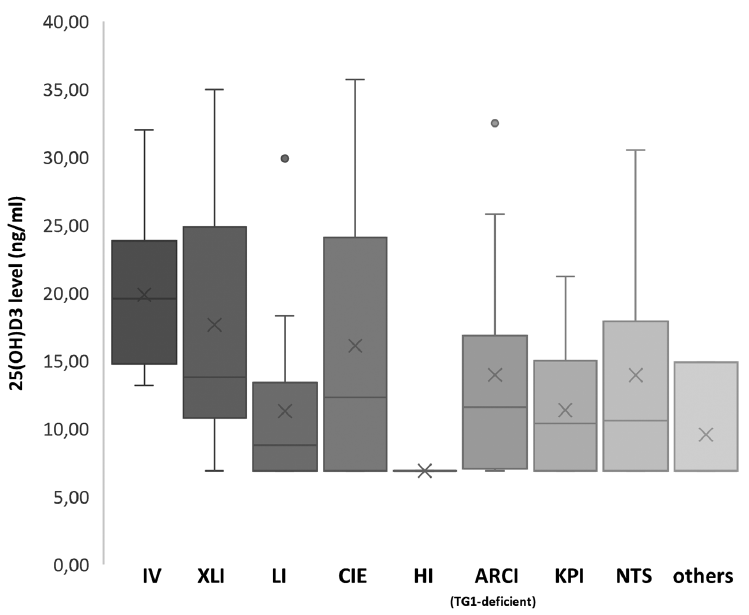 Click to show fullsize
Click to show fullsize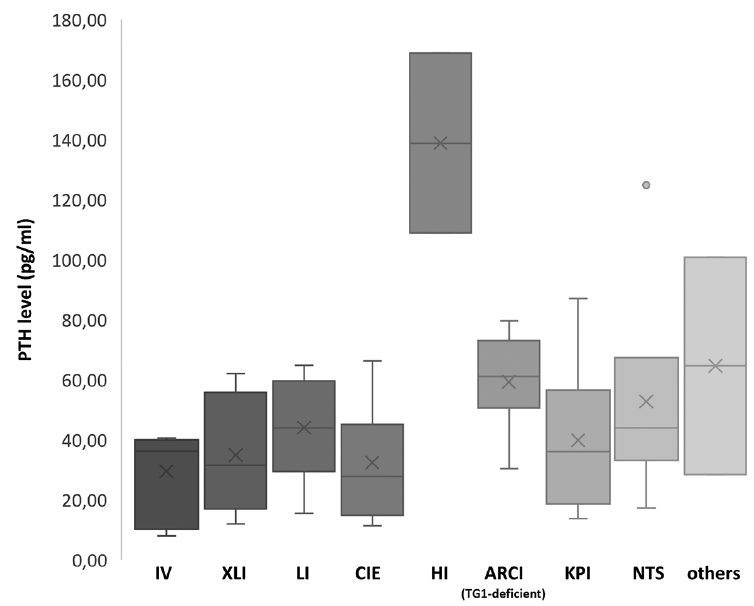 Click to show fullsize
Click to show fullsize