


1Division of Dermatology, Tel Aviv Sourasky Medical Center, and 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. E-mail: shamirg@smile.net.il
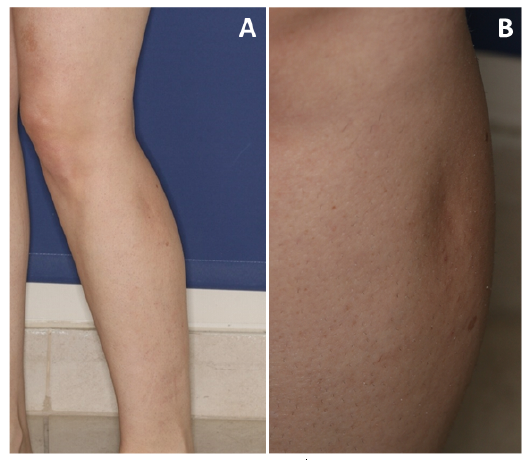
A 36-year-old woman with medical history of polycystic ovary syndrome presented with a 2-year history of an asymptomatic semi-circular depression on her left calf (Fig. 1). The patient denied any preceding local inflammation or trauma to the area and any systemic manifestations. Physical examination revealed a skin-coloured, semi-circular depression, 7-cm long, on her proximal lateral left calf. Routine laboratory work-up revealed no abnormalities.
High-frequency ultrasound (HFUS) examination of the semi-circular depression revealed preserved epidermis and dermis, while subcutaneous fat was diminished, with a 4-mm decrease compared with the right calf. Moreover, the septa of the subcutaneous tissue were more hyperechoic and prominent compared with their normal state (Fig. 2). No evidence of oedema or increased vascularity on colour Doppler were detected. The patient confirmed a long-standing history of frequent leg crossing while sitting at home and at work. The site of the skin depression correlated with the area on her left calf resting over the patella of the right knee.
What is your diagnosis? See next page for answer.
Fig. 1. Clinical photographs. (A) Skin-coloured, 7-cm long depression on the proximal-lateral left calf. (B) Close-up view.
Fig. 2. Grey-scale high-frequency ultrasound (HFUS) longitudinal view images, showing a decrease in subcutaneous tissue in (a) left calf compared with (b) right calf. There was no evidence of oedema or hyper-vascularity on colour Doppler (not shown).
Acta Derm Venereol 2021; 101: adv00524.
Diagnosis: Semi-circular lipoatrophy (leg crossers’ dimple)
Semi-circular lipoatrophy (SCL) presents as a semi-circular skin depression due to localized loss of subcutaneous fat. SCL is usually diagnosed on the lower limbs in middle-aged women. Repeated external pressure is the most common cause of this localized lipoatrophy, and, in most cases, avoiding the precipitating repetitive trauma results in complete remission (1–5). SCL is usually diagnosed and followed by evaluating the clinical appearance of the skin. Skin biopsies may reveal non-specific histological findings of lipoatrophy (2–5). We present here the benefit of using high-frequency ultrasound (HFUS) as a non-invasive tool in SCL diagnosis and assessment of response to pressure avoidance. In the current case a diagnosis of SCL was made and the patient was advised to avoid crossing her legs.
Over the last 2 decades HFUS has emerged in the field of dermatology, with new variable high-frequency transducers enabling real-time, non-invasive imaging of the skin. The usefulness of HFUS in recognizing dermatoses involving the subcutaneous tissue is well acknowledged (6) and the imaging characteristics of several subcutaneous disorders have been described in recent years. Table I summarizes the sonographic characteristics seen in septal and lobular panniculitis, morphea in both active and atrophic phases, subcutaneous granuloma annulare, nodular fasciitis, and now also SCL.
In the case of SCL, the use of HFUS may aid diagnosis, as well as circumvent the need for a biopsy or other imaging modalities, e.g. magnetic resonance imaging (MRI) (7). Viskovic et al. demonstrated that ultrasound is a clinically useful tool for the diagnosis of lipoatrophy compared with clinical assessment (8). The sonographic image can identify changes in the skin layers, allowing detection of inflammation. Thinning of the subcutaneous tissue without an increase in its echogenicity or its vascularization points to the lack of inflammation found in the active stage of morphea (9). Furthermore, the absence of sonographic changes in the dermis in SCL is less characteristic of the atrophic stage of connective tissue diseases, as seen in morphea. In contrast to septal panniculitis, which demonstrates hypoechoic septa due to oedema and inflammation (10), in SCL the septa appear hyperechoic and more prominent, which may correspond to the septal fibrosis found on histology. Another major advantage of use of HFUS in cases of SCL is the opportunity for monitoring the resolution of the atrophy after avoiding the identified cause.
In summary, this case exemplifies the usefulness of HFUS as an adjunct tool for the diagnosis of subcutaneous pathologies.
The authors have no conflicts of interest to declare
Table I. Sonographic characteristics of selected dermatoses involving the subcutaneous tissue


 Click to show fullsize
Click to show fullsize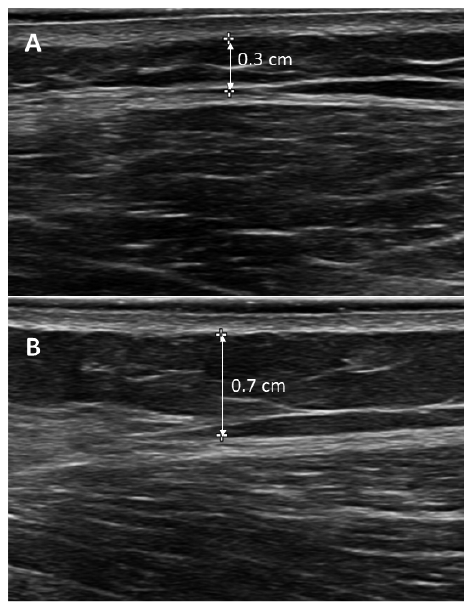 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize