


1Dermatology Deparment, Dermatologic Institute GlobalDerm, Palma del Río (Córdoba), 2Unit of Cutaneous Oncology, Hospital San Juan de Dios, Córdoba, 3Dermatology Deparment, Complexo Hospitalario Universitario A Coruña, Coruña, 4Dermatology Deparment, Hospital Clínic of Barcelona, Barcelona, 5Dermatology Deparment, Central Universitary Hospital of Asturias and Instituto de Investigación Sanitaria of Principado de Asturias, IUOPA, Oviedo University, Oviedo, 6Dermatology Deparment, Universitary Hospital Germans Trias i Pujol, Badalona, Barcelona, 7Dermatology Deparment, Universitary Hospital 12 de Octubre, Madrid, 8Dermatology Deparment, Complejo Asistencial Universitario de Salamanca, Salamanca, 9Unit of Cutaneous Tumors, Universitary Hospital Miguel Servet, Zaragoza, 10Dermatology Deparment, Universitary Hospital Puerta del Mar, Cadiz, 11Dermatology Deparment, Univesitary Hospital Vall d’Hebron, Barcelona, 12Dermatology Deparment, Universitary Hospital of León, León, 13Melanoma Unit, Dermatology Deparment, Universitary Hospital Virgen Macarena, Sevilla, 14Dermatology Deparment, Universitary Hospital Son Llàtzer, Mallorca, 15Department of Dermatology, University Clinic of Navarra, School of Medicine, University of Navarra, Pamplona, 16Dermatology Deparment, Instituto Valenciano de Oncología, Valencia, 17Dermatology Deparment, Universitary Hospital San Cecilio, Granada, 18Dermatology Deparment, Universitary Hospital La Princesa, Madrid, 19Dermatology Deparment, General Universitary Hospital, Alicante, 20Dermatology Area, Clinical Medicine Department, University Miguel Hernandez, Sant Joan de Alicante, Spain, and 21Department of Dermatology, Fundación Universitaria Sanitas, Bogotá-Colombia
The aim of this study was to compare tumour burden in patients who underwent surgery for melanoma and cutaneous squamous cell carcinoma during nationwide lockdown in Spain due to COVID-19 (for the period 14 March to 13 June 2020) and during the same dates in 2019 before the COVID-19 pandemic. In addition, associations between median tumour burden (Breslow thickness for melanoma and maximum clinical diameter for cutaneous squamous cell carcinoma) and demographic, clinical, and medical factors were analysed, building a multivariate linear regression model. During the 3 months of lockdown, there was a significant decrease in skin tumours operated on (41% decrease for melanoma (n = 352 vs n = 207) and 44% decrease for cutaneous squamous cell carcinoma (n = 770 vs n = 429)) compared with the previous year. The proportion of large skin tumours operated on increased. Fear of SARS-CoV-2 infection, with respect to family member/close contact, and detection of the lesion by the patient or doctor, were related to thicker melanomas; and fear of being diagnosed with cancer, and detection of the lesion by the patient or relatives, were related to larger size cutaneous squamous cell carcinoma. In conclusion, lockdown due to COVID-19 has resulted in a reduction in treatment of skin cancer.
Key words: melanoma; cutaneous squamous cell carcinoma; delay; surgery; COVID-19; SARS-CoV-2.
Accepted Aug 13, 2021; Epub ahead of print Aug 16, 2021
Acta Derm Venereol 2021; 101: adv00525.
doi: 10.2340/00015555-3890
Corr: Antonio Tejera-Vaquerizo, Dermatology Deparment, Dermatologic Institute GlobalDerm, Palma del Río (Córdoba), Spain. E-mail: antoniotejera@aedv.es
There is little evidence regarding the impact of COVID-19 lockdown on skin tumour burden. The COVID-19 lockdown resulted in a reduction in surgery for melanoma and cutaneous squamous cell carcinoma and an increase in the proportion of tumours with a worse prognosis. The increase was due to patient-dependent factors; in particular, fear of SARS-CoV-2 infection. Therefore, health education programmes targeting the general population are needed to ensure the prompt treatment of patients with skin cancer.
The coronavirus disease 19 (COVID-19) pandemic, which started in Wuhan, China in December 2019 (1), led to a massive lockdown in Spain and many other countries. Disruptions to healthcare services during this time have raised questions about possible delays in skin cancer treatment. A recent study of the estimated effect of diagnostic delays due to lockdown on tumour size in melanoma and cutaneous squamous cell carcinoma (cSCC), using a tumour growth model, showed that there was a significant increase in the proportion of tumours with a poor prognosis (1, 2). Nonetheless, the true effects of lockdown on skin cancer and the reasons for delayed treatment are unknown. The aims of this study were to analyse the effects of lockdown on tumour burden (thickness and diameter) in melanoma and cSCC, and to investigate factors associated with thicker or larger tumours.
A multicentre observational study was performed of all consecutive patients who underwent surgery for melanoma or cSCC at 18 referral hospitals for skin cancer in different regions of Spain between 14 March 2020, the start of a nationwide lockdown due to COVID-19, and 13 June 2020, the end of lockdown. Patients treated during the same period in 2019 were selected as controls. The study was approved by the ethics committee at Hospital Universitario Reina Sofía de Córdoba (reference 4682).
Study variables
Patient age and sex were recorded, analysing changes in tumour burden of patients during lockdown in 2020 and the same period from 2019. For melanomas, information was collected on Breslow thickness (stratified according to the American Joint Committee on Cancer (AJCC) staging system (4)), the presence or absence of ulceration, and clinicopathological stage. For cSCCs, clinical diameter was recorded (classified as < 20, 20–40, or > 40 mm, as recommended by the AJCC (4)) and clinical stage. This information was obtained from the pathology reports at the participating hospitals.
To analyse factors associated with greater tumour burden following lockdown, a standardized questionnaire was administered in person (Appendix S1) to patients who attended each centre and who consented to participate. The following data were collected:
Statistical analysis
Differences between 2020 and 2019. Differences were analysed using the χ2 test and or the t-test, as appropriate.
Factors associated with greater tumour burden. Because the distributions of Breslow and diameter were skewed, logarithmic transformation was performed to construct the data as normal. Normality of distribution was checked using the Kolmogorov–Smirnov test and visual assessment. Patients with melanoma in situ were excluded from this analysis as it is impossible to transform zero values. To explore univariate factors potentially associated with tumour burden, differences in thickness and diameter were analysed, and the results for the different categories of each study variable were compared. Results were compared using the non-parametric Mann–Whitney U and Kruskal–Wallis tests for 2 or 3 or more categories, respectively. Variables that were significant (p < 0.1) in the univariate analysis were used to fit a linear regression model (with the log-transformed dependent variables) using a forward stepwise selection approach, in which variables with a significance level of p > 0.1 were excluded and included again if p < 0.05 to build a multivariate linear regression model for log-transformed thickness and diameter values. The variables were analysed by groups (medical causes–medical history–cancer awareness vs reasons for delay). Those that were significant (p < 0.05) in the multivariate analysis of each group were included in a combined multivariate analysis. Regression coefficients were calculated with 95% confidence intervals (95% CIs). Analyses were performed in SPSS (Version 21.0. IBM Corp., Armonk, NY, USA).
Comparison of 2019 and 2020
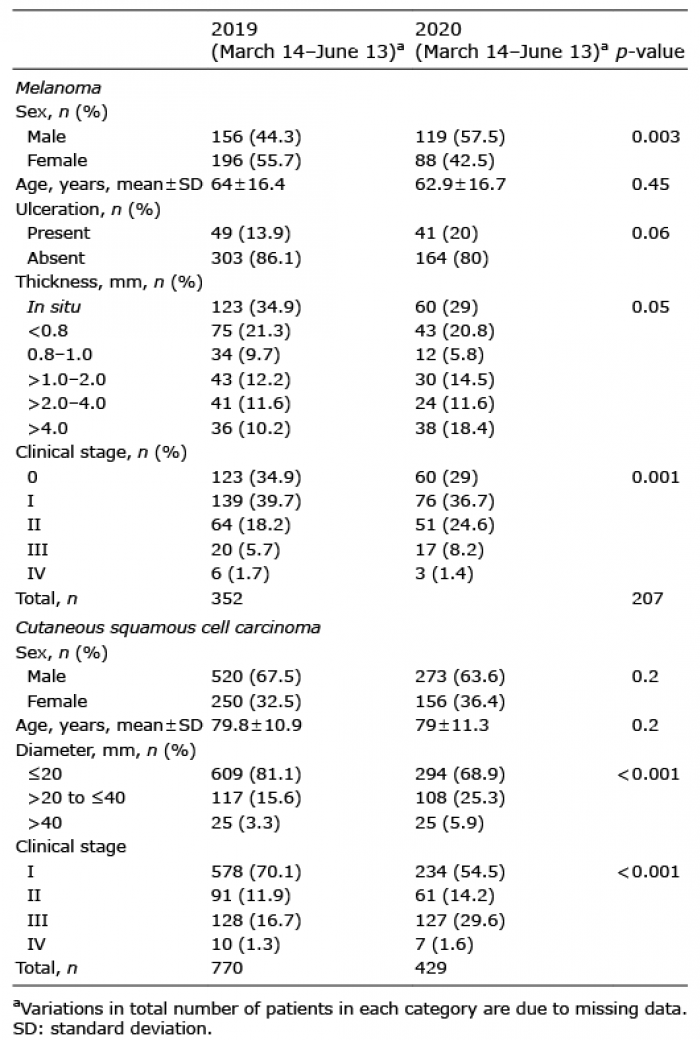
The number of melanomas treated during the periods analysed decreased from 352 in 2019 to 207 in 2020 (41% reduction) (Table I). The proportions of men and women was 44.3% and 55.7% in 2019, and 57.5% and 42.5% in 2020 (p = 0.003). The number and percentage of different Breslow thicknesses also varied significantly from 2019 to 2020, with a reduction in melanomas in situ (n = 123 (34.9%) vs n = 60 (29%)) and a slight increase in thick melanomas (> 4 mm) (n = 36 (10.2%) vs n = 38 (18.4%)) (p = 0.05). Thus, the most relevant changes in clinicopathological stages were observed for stage 0 melanoma. There were also changes in stage II melanoma (n = 64 (18.2%) vs n = 51 (24.6%)) (p = 0.001), and stage III melanoma (n = 20 (5.7%) vs n = 17 (8.2%)). No significant change was observed for stage IV melanoma.
Table I. Comparison of clinicopathological characteristics of melanoma and cutaneous squamous cell carcinoma during the 2020 COVID-19 lockdown and the same period in 2019
The number of cSCCs treated decreased by 44%, from 770 cases in 2019 to 429 in 2019 (Table I). In this case, however, there was no change in the proportions of men and women. The mean age of patients was similar in both periods. The number of cSCCs measuring < 20 mm decreased from 609 (81.1%) in 2019 to 294 (68.9%) in 2020, but there was an increase in the proportions of tumours measuring 20–40 mm (n = 117 (15.6%) vs n = 108 (25.3%)) and > 40 mm (n = 25 (3.3%) vs n = 25 (5.9%)) (p < 0.001). A reduction in stage I cSCCs (n = 578 (70.1%) vs n = 234 (54.5%)) and a proportional increase in stage II (n = 91 (11.9%) vs n = 61 (14.2%)) and stage III (n = 128 (16.7%) vs n = 127 (29.6%)) cSCCs were also observed. As with melanoma, no significant changes were observed for stage IV tumours. The differences between stages were statistically significant (p < 0.001)
Factors associated with tumour burden
Melanoma. Of the 207 patients who underwent melanoma surgery between the start and end of lockdown, 147 (71%) completed the questionnaire. There was no difference in the median of Breslow and age for non-responded and responded patients to questionnaire (data not shown). Of these, only those with invasive melanoma (n = 100) were analysed to investigate factors associated with tumour burden (see Methods). The univariate analysis showed a significant association between age and Breslow thickness (Table II). Other factors associated with a greater median thickness were living in a nursing home, no schooling, living in a rural area, non-performance of skin self-examination or by a doctor in the past year, and detection of the tumour by a doctor. Multivariate analysis of these variables confirmed that living in a nursing home vs a private home was associated with greater median Breslow thickness (4.95; 95% CI: 1.1, 14.1; p = 0.03), while performance vs non-performance of a self skin-examination (0.6; 95% CI: 0.4, 0.9; p = 0.01) and detection of the lesion by a family member/close contact vs the patient (0.4; 95% CI: 0.2, 0.7; p < 0.002) were associated with lower median thickness.
Table II. Demographic characteristics and tumour burden in patients with invasive melanoma or cutaneous squamous cell carcinoma during the COVID-19 lockdown in Spain
Among the reported reasons for delays, only fear of infection with SARS-CoV-2 was associated with greater Breslow thickness in both the univariate and multivariate analyses (2.8; 95% CI: 1.7, 5.6; p = 0.005) (Table III).
Table III. Patient-related and medical reasons for delays in treatment and tumour burden in invasive melanomas and cutaneous squamous cell carcinomas during COVID-19 lockdown
In the combined multivariate analysis, age (as a continuous variable) (1.01; 95% CI: 1.005, 1.03; p = 0.01), living in a nursing home (3.4; 95% CI: 1,12; p = 0.05), detection of the lesion by a family member/close contact (0.5; 95% CI: 0.3, 0.8; p = 0.007), and fear of infection with SARS-CoV-2 (2.2; 95% CI: 1.2, 2.4; p = 0.02) were all associated with Breslow thickness. The R2 of the model was 0.3 (Table IV).
Table IV. Combined multivariate analysis of factors associated with melanoma thickness
Squamous cell carcinoma. Of the 429 patients who underwent surgery for cSCC between the start and end of lockdown, 323 (75.2%) completed the study questionnaire. There was no difference in the median of diameter of tumours and age for non-responded and responded patients to questionnaire (data not shown). The univariate analysis showed a significant association between a larger tumour diameter and age, living in a nursing home, and not having seen or heard skin cancer campaign messages or news during lockdown (Table II). Detection of the tumour by a doctor, by contrast, was associated with a smaller diameter. Multivariate analysis confirmed that age (1.01; 95% CI: 1.005, 1.02; p = 0.002), living in a nursing home vs a private home (2; 95% CI: 1.1, 3.3; p = 0.001), and diagnosis by a doctor vs detection by the patient (0.8; 95% CI: 0.7, 0.9; p = 0.004) were associated with cSCC diameter.
Among the reasons reported for delays, fear of being diagnosed with cancer, a delay of over 2 weeks in getting an appointment with a dermatologist, and reopening of surgical activities within one month were associated with a larger diameter. The only factor that retained its significance in the multivariate analysis was fear of being diagnosed with cancer (2.5; 95% CI: 1.6, 3.9; p < 0.001) (Table III).
In the combined multivariate analysis, age (as a continuous variable) (1.01; 95% CI: 1.2, 1.02; p = 0.03), living in a nursing home (1.7; 95% CI: 1, 2.3; p = 0.02), detection by a doctor (0.8; 95% CI: 0.7, 0.9; p = 0.006), and fear of infection with SARS-CoV-2 (2.2; 95% CI: 1.4, 3.6; p = 0.06) were all predictors of cSCC diameter. The R2 of the model was 0.11 (Table V).
Table V. Combined multivariate analysis of factors associated with cutaneous squamous cell carcinoma diameter
The main finding of this study is that the nationwide lockdown imposed in Spain due to the COVID-19 pandemic resulted in a reduction in the number of patients who underwent surgery for melanoma or cSCC and an increase in the proportion of thicker and larger tumours operated on.
During the lockdown Spanish citizens were required to remain in their homes for a mean of 6 weeks, starting on 14 March 2020. The health authorities ruled that all non-deferrable procedures, including cancer treatments, should continue as normal, and that primary care activity, specialist visits, and hospital consultations should be reduced to the minimum to prevent these centres from becoming foci of infection. In addition, surgical activity was either cancelled or drastically reduced in order to redirect all necessary resources to the care of patients with COVID-19. The sum of these actions, combined with variable reopening times for the different public healthcare services, resulted in fewer skin cancer surgeries and a greater proportion of thick melanomas and large cSCCs.
Three societies have published recommendations for the management and treatment of skin tumours in the context of the current COVID-19 pandemic. With regard to melanoma, the National Comprehensive Cancer Network (NCCN) recommends a delay of up to 3 months in T0 and T1 cases, even if the margins are affected. However, it mentions the possibility of excision of up to 1 cm in cases of in situ/invasive melanoma if possible (3). This 1-stage management of in situ or thin invasive melanomas was beginning to gain acceptance in our country before the SARS-Cov-2 pandemic in an attempt to simplify the management of melanomas (4, 5). The British Association of Dermatologists and the British Society for Dermatological Surgery (6) have made similar recommendations for delay in the management of thin or in situ melanomas. With respect to SCC, the recommendations of these societies are similar with respect to SCC in situ or of the well-differentiated histological variety, with a recommendation for a delay of 2–3 months if necessary. Logically, fast-growing, symptomatic or ulcerated tumours, or tumours with perineural invasion or poorly differentiated tumours, especially in immunocompromised patients, should be prioritized (7).
A number of recent studies have reported a significant reduction in the treatment of melanoma at Italian hospitals during lockdown in Italy (8, 9) According to a recent study by our group, which modelled tumour growth based on the kinetics of melanoma and cSCC (2), a diagnostic delay of 2 months would result in a doubling of the proportion of thick melanomas (> 4 mm) and a 60% increase in that of large cSCCs (> 40 mm). The current study also observed a doubling of the proportion of thick melanomas (18.4% in 2020 vs 9.3% in 2019), despite the 41% reduction in the number of cases. Similarly, despite a 47% reduction in the number of cSCCs treated, the number of large tumours (> 40 mm) was the same in 2019 and 2020. In this case, however, the proportion of large cSCCs (3.3% vs 5.9%) and stage III cSCCs doubled (16.7% vs 29.6%). While the current findings appear to indicate that a considerable proportion of patients with skin tumours with a worse prognosis received care as usual, they also suggest that we can expect to see an increase in cases with a worse prognosis in the coming months, as more than a third of patients who would usually have been seen during the study period were not.
It is worth mentioning that the melanoma group that has decreased the most is that of melanomas in situ, while invasive melanomas have increased proportionally. This could indicate that, over a period of months, melanomas in situ can become invasive in many cases.
Age was associated with thicker melanomas and larger cSCCs, particularly in the subgroup of nursing home residents, although this group was small. Older age is a known risk factor for thicker skin tumours, as well as a predictor of poor prognosis (8, 9). Nevertheless, because elderly patients with comorbidities are at the greatest risk of SARS-CoV-2 infection and its complications, they are much more likely to experience treatment delays (10). The dangers of neglecting melanoma during the COVID-19 pandemic have already been highlighted (11).
One important finding of the current study is that of all the possible reasons for treatment delays analysed, fear of infection with SARS-CoV-2 was the only factor associated with greater melanoma thickness. Widespread fear of COVID-19 and its consequences among the general public is already recognized in the literature (12).
Fear of being diagnosed with cancer was associated with larger size cSCCs. Cancer fears are relatively common in the general population and can lead to avoidance behaviours and delays in seeking care (13). In some cases, this behaviour has been associated with the diagnosis of large tumours (14).
Compared with tumours detected by the patient, melanomas detected by a family member/close contact were more likely to be thinner, while cSCCs detected by a doctor were more likely to be smaller. The findings of the current study support reports that melanoma thickness at diagnosis varies according to the person who detected the lesion (15).
Although patients with cSCC in hidden part of the body have been found to be more likely to have large tumours, this was not the case in the current study.
Finally, despite the organizational changes implemented at each of the study hospitals, none of the medical reasons for delayed surgery (misdiagnosis by a doctor, delays in getting an appointment with a dermatologist, surgical delays, or time to reopening of surgical activity) was associated with tumour burden.
The main strength of the current study is that it is a multicentre study of referral hospitals for skin cancer in different regions of Spain. In addition, the fact that the analysis was based on general demographic and clinical variables and not on specific factors will have reduced the risk of bias.
A limitation of the current study is that it analysed only the first 3 months of lockdown, and therefore may have underestimated the effect of disruptions to healthcare services on tumour burden. Since melanoma and cSCC incidence rates do not vary substantially from year to year, it is likely that more patients than usual will present with larger-than-expected tumours in the coming months. A further limitation is that it is not a randomized sample.
In conclusion, this study showed that there was a reduction in the number of melanomas and cSCCs treated in the 3 months of nationwide lockdown in Spain, as well as an increase in the proportion of tumours with a poor prognosis.
In the case of melanoma, patient-related factors, such as age, living in a nursing home, and fear of infection with SARS-CoV-2, were associated with greater Breslow thickness, while detection of lesions by a family member/close contact was associated with lower thickness. In the case of cSCC, age, living in a nursing home, and fear of being diagnosed with cancer were associated with a larger diameter, while detection of the tumour by a doctor was associated with a smaller diameter. None of the medical reasons for delay were associated with greater tumour burden.
Fear of infection with SARS-Cov-2 and of being diagnosed with cancer were both predictors of tumours with a worse prognosis. As these are modifiable factors, they should be included in skin cancer awareness and screening programmes.
The authors thank M. A. Descalzo-Gallego from the Research Unit of the Spanish Academy of Dermatology and Venereology (AEDV) for reviewing the study methodology and statistical analyses, and the pathology laboratories at the different hospitals for helping to identify cases.
Reviewed and approved by Hospital Reina Sofía de Córdoba IRB; approval #4682.
The current study was presented at the European Academy of Dermatology and Venereology (EADV) 2020 congress.
Conflicts of interest: CG-D reports other from Lilly, grants and other from Novartis, outside the submitted work. SP reports grants and other from Amgen, personal fees and other from Avene, other from Abbvie, grants, personal fees, non-financial support and other from Almirall, personal fees from BSM, grants, personal fees and non-financial support from ISDIN, grants, personal fees and non-financial support from La Roche Posay, grants, personal fees and non-financial support from Leo Pharma, non-financial support from MSD, personal fees and non-financial support from Pierre Fabre, personal fees and non-financial support from Pfizer, personal fees, non-financial support and other from Regeneron, grants, personal fees and non-financial support from Roche, personal fees and non-financial support from Sanofi, grants and personal fees from Sunpharma, grants from Castle, personal fees from Canfield, non-financial support from Lilly, non-financial support from Novartis, grants from Melagenix, outside the submitted work.


 Click to show fullsize
Click to show fullsize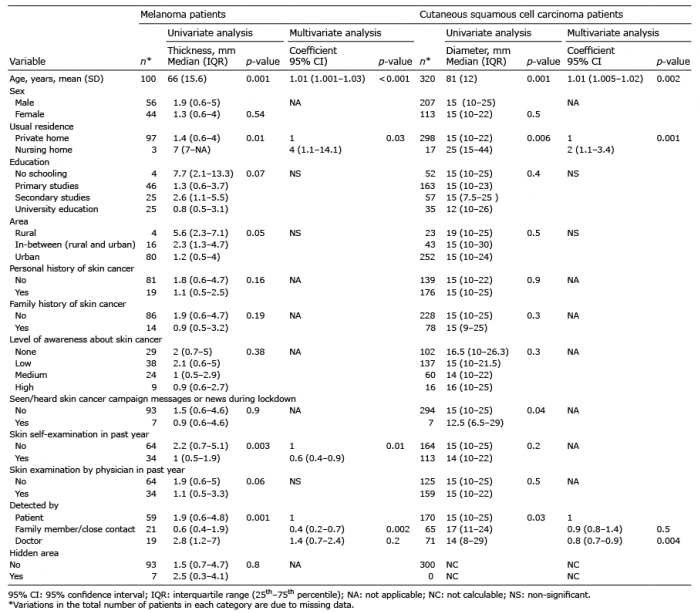 Click to show fullsize
Click to show fullsize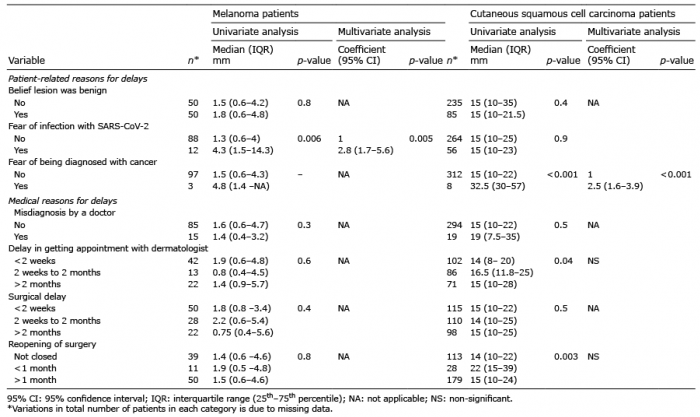 Click to show fullsize
Click to show fullsize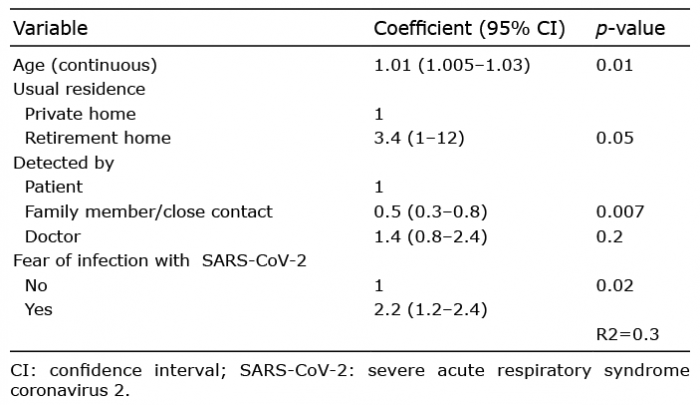 Click to show fullsize
Click to show fullsize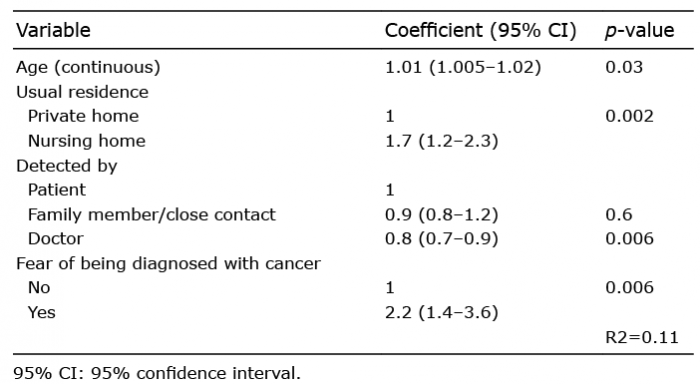 Click to show fullsize
Click to show fullsize