


Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Münster, Germany
Chronic pruritus of unknown origin is established when no underlying origin for pruritus can be determined. This retrospective cohort study aimed to determine the clinical profile and disease-related burden of chronic pruritus of unknown origin. A total of 263 patients (female/male: 154/109, median age 55 years) were included. Moderate to severe itch intensities were recorded (median average itch: 5.5/10, n = 200; median worst itch: 7.5/10, n = 199). In most cases pruritus lasted longer than 1 year (77.6%), occurred daily (68.2%), occurred in attacks (72.8%), and was often accompanied by dysaesthesias, such as burning, tingling and stinging. Quality of life was moderately impaired, while 22.2% and 12.4% of patients showed pathological anxiety and depression scores. Scratch lesions were associated with higher intensities of itch and greater impairment of quality of life, while women were more burdened by the disease than men. Chronic pruritus of unknown origin may occur at any age and the majority of patients endure severe itch with substantial disease-related burden.
Key words: chronic pruritus of unknown origin; itch; prurigo nodularis; visual analogue scale; quality of life; ItchyQol.
Accepted Aug 17, 2021; Epub ahead of print Aug 18, 2021
Acta Derm Venereol 2021; 101: adv00550.
doi: 10.2340/00015555-3892
Corr: Manuel P. Pereira, Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: manuelpedro.pereira@ukmuenster.de
Chronic pruritus of unknown origin is defined as itch lasting for 6 weeks or longer, for which no underlying origin can be determined. This study analysed the clinical profile and burden of chronic pruritus of unknown origin. In most cases itch is of long duration, occurs daily, is of moderate/high intensity and is accompanied by other symptoms, such as burning or stinging. The quality of life of patients with chronic pruritus of unknown origin is impaired, and a subset of patients shows signs of depression and anxiety. Patients with scratch lesions have more severe itch and lower quality of life, while women are more burdened by the disease than are men.
Chronic pruritus (CP), defined as pruritus lasting for 6 weeks or longer, may arise from a variety of heterogenous conditions, including dermatological, systemic, neurological and psychiatric diseases (1). However, in some cases, even after a comprehensive diagnostic work-up, no underlying origin for CP can be determined. The term CP of unknown origin (CPUO), or alternatively CP of undetermined origin, is used to classify these patients (1–3). This condition reflects merely the absence of a known aetiology, but not its dermatological phenotype (for example, absence or presence of scratch-related lesions), clinical profile or treatment response (2). It is estimated that, in approximately 6% of cases of CP, the underlying origin remains unknown (4); however, epidemiological studies are needed in order to establish the exact prevalence of CPUO.
Being a diagnosis of exclusion, an extensive diagnostic work-up is advised in order to rule out an underlying medical condition leading to CP, as recommended in recent guidelines (3, 5). In addition to a detailed medical history and a complete dermatological examination, core laboratory tests should be performed in all patients. Further procedures, such as skin biopsies, malignancy screening tests or neurology referral may be recommended in selected cases (3, 5).
CPUO remains a poorly defined condition with regard to its clinical profile. To address this, a retrospective analysis of patients with CPUO was conducted, focusing on the clinical characteristics of this condition, comorbidities of affected patients, and disease-related burden.
Patients
Patients with CPUO treated at the Center for Chronic Pruritus, University Hospital Münster, Germany, between May 2005 and November 2018 were included in this retrospective observational study. Inclusion criteria were the presence of CP, i.e. pruritus lasting 6 weeks or longer, and the diagnosis of CPUO as defined by the International Forum for the Study of Itch (1). All patients were examined by a board-certified dermatologist. Medical history-taking, dermatological examination and diagnostic work-up were performed according to the European and German guidelines for the assessment and treatment of CP (3, 5). Guidelines recommend a detailed medical history (including pruritus-specific history, as well as a general personal and family history), a complete dermatological and a general physical examination (including palpation of abdominal organs and lymph nodes) and screening laboratory work-up (differential blood count, renal retention parameters, liver parameters, glucose ferritin and thyroid stimulating hormone). Further laboratory work-up, skin biopsies (e.g. for histology and direct immunofluorescence), microbiology or medical imaging are advised in selected cases (3, 5). An aetiology for CP was excluded by medical history, dermatological examination and/or diagnostic work-up, and thus the diagnosis of CPUO was established for all patients included in this analysis. The study was approved by the local ethics committee of Medical Faculty of the University of Münster (2007-413-f-S). All patients provided written informed consent. The study was performed according to the principles of the Declaration of Helsinki 2013 and later revisions.
Study outcomes
Data were retrieved from the patients’ medical records and from the centre’s own database. General patient features, including demographic characteristics and comorbidities, were recorded. Atopic disposition was assessed using the Erlanger Atopy Score (6). The performed diagnostic work-up (laboratory work-up, histology, direct immunofluorescence, determination of the intraepidermal nerve fibre density (IENFD), serum antibodies, medical imaging, microbiology and functional tests) was documented for each patient. To establish the clinical profile of CPUO pruritus characteristics were analysed (duration, localization, intensity using the visual analogue scale (VAS), frequency, dynamic, accompanying sensory symptoms, trigger and alleviating factors) and skin condition (xerosis, dermographism, presence of scratch lesions). To investigate the burden of disease, patients completed the ItchyQol (score range 1–5) (7–9) to assess the impairment of quality of life owing to itch, and the Hospital Anxiety and Depression Scale (HADS; score range for subscales anxiety and depression: 0–21) (10) to screen for depression and anxiety disorders. In addition, the amount of lost sleep (in h per night) due to itch was assessed in order to establish the impact of CPUO on sleep.
Statistical analysis
IBM SPSS Statistics for Windows, version 25.0 (Armonk, NY, USA) was used for statistical analyses. Data were analysed descriptively and are shown as number of cases/total number of assessments (percentage of cases), or as median [interquartile range; IQR]. Group comparisons were performed using the Mann–Whitney U test or the Kruskal–Wallis test for continuous variables and the χ2 test or Fischer’s exact test for categorical variables, as appropriate. No corrections for missing data were performed. A p-value < 0.05 was considered statistically significant.
Demographics and comorbidities
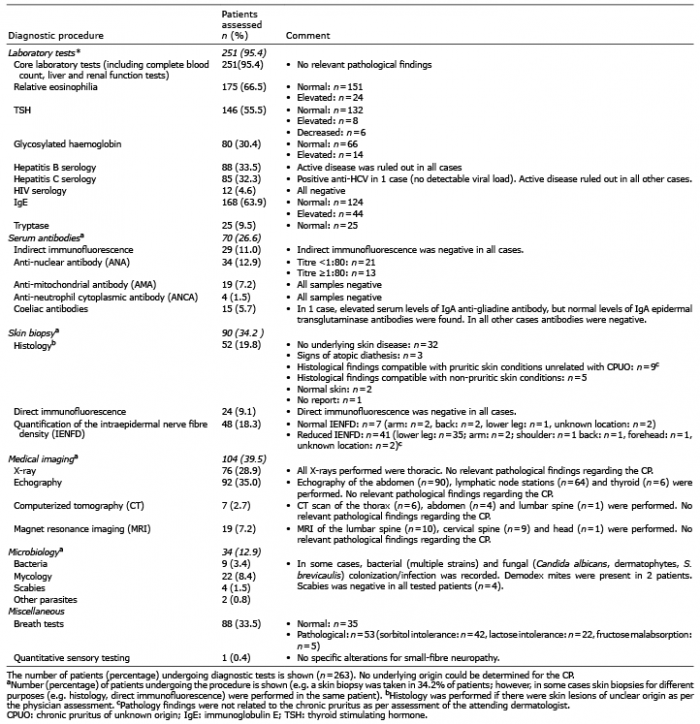
A total of 263 patients (154 female, 109 male; median age 55 years [41; 68], range: 9–97) were included. The number of visits to the centre ranged from 1 to 22. Most patients visited once (55.5%), twice (23.2%) or 3 times (9.5%) the centre, while only a minority of patients (11.8%) had more than 3 visits. All patients included in this study underwent medical history-taking, an oriented physical examination and a comprehensive dermatological examination by a board-certified dermatologist. A vast majority of patients undertook core laboratory tests (95.4%), while medical imaging procedures (39.5%), skin biopsies (34.2%), determination of serum antibody titres (26.6%) and microbiological examinations (12.9%) were performed in selected cases (Table I). The diagnostic work-up revealed no cause for the CP in all cases, as per the assessment of the attending physician.
Table I. Chronic pruritus (CP) of unknown origin: diagnostic work-up
Demographic characteristics, comorbidities and atopic disposition can be consulted in Table II. According to the investigations performed, none of the comorbidities explained the origin of pruritus.
Table II. Demographic data and comorbidities
Pruritus characteristics
Patients with CPUO showed a moderate median itch intensity on the VAS at the consultation day (median [IQR]: 5.0 [3.0; 7.5], n = 171]) and, on average, in the 4 weeks prior to the consultation (5.5 [3.3; 7.5], n = 200]), while the median worst itch intensity in the 4 weeks prior to the consultation was severe (7.5 [4.5; 9.0], n = 199]; Fig. 1). Average itch was severe or very severe (i.e. VAS≥7.0) (11) in 34.5% of cases, while worst itch was severe or very severe in most patients (58.8%; Fig. 1).
Fig. 1. Itch intensity. (A) Patients with chronic pruritus of unknown origin showed a moderate median itch intensity at the consultation day (median [interquartile range (IQR)]: 5.0 [3.0; 7.5], n = 171]) and, on average, in the 4 weeks prior to the consultation (median [IQR]: 5.5 [3.3; 7.5], n = 200]). The median worst itch intensity in the 4 weeks prior to the consultation was severe (median [IQR]: 7.5 [4.5; 9.0], n = 199]). Data are shown as median [IQR]. Middle line: median, bottom/top of box: 1st/3rd quartile; whiskers: lowest/highest case within 1.5 times IQR. (B) The number of patients with no (visual analogue scale [VAS]: 0), weak (0<VAS<3), moderate (3≤VAS<7), severe (7≤VAS<9) and very severe pruritus (VAS≥9) is shown.
The majority of patients had pruritus for 1 year or more (156/201, 77.6%). Duration of pruritus was not associated with age (p = 0.75). In most cases, one body site was affected at onset (98/195, 50.3%) and spread to additional body sites in the course of the disease (154/195, 79.0%). The majority of patients reported experiencing pruritus on a daily basis (131/192, 68.2%), during the day and at night (118/178, 66.3%), and described itch occurring in attacks (142/195, 72.8%). Accompanying sensory symptoms, such as burning, tingling and stinging, were common (79.5%), whereas an isolated itch sensation was observed in 20.5% of cases. Pruritus characteristics are summarized in Table III.
Table III. Pruritus characteristics and skin condition of patients with chronic pruritus of unknown origin (n = 263)
Dermatological status
Dermatological examination of the cohort revealed that xerosis was a common finding (180/252, 71.4%), while no patient had a primary pruritic skin disease. Only a minority of patients had a pathological dermographism (urticarial: 15/248, 6.0%; white: 8/248, 3.2%; Table III).
Most patients had no scratch lesions (154/244, 63.1%). Of the patients with scratch lesions (n = 90), 60 (22.7% of the whole cohort) were considered to have chronic scratch lesions (i.e. chronic prurigo or lichen simplex; Table III). Patients with a pruritus duration of less than 6 months showed scratch lesions more often, compared with patients with longer duration of pruritus (p = 0.002). Patients with scratch lesions were older (p = 0.001, n = 244), showed higher average itch intensity scores in the previous 4 weeks (p = 0.003, n = 188) and at the consultation day (p = 0.049, n = 158), and had a higher impairment of sleep (p = 0.03, n = 121) and quality of life (p < 0.001, n = 150) compared with those without scratch lesions.
Burden
Quality of life was moderately impaired due to itch, as assessed by the ItchyQol (median [IQR]: 2.5 [2.0; 3.1], n = 155). Low median anxiety (6.0 [4.0; 9.0], n = 216) and depression (4.0 [2.0; 7.0], n = 217) scores were recorded using the HADS. Only 22.2% and 12.4% of patients had pathological anxiety and depression scores (i.e. ≥ 11), respectively. As for sleep quality, a vast majority of the patients reported sleep impairment owing to pruritus (105/108, 97.2%). A median of 2.0 [1.0; 3.0] (n = 127) h of sleep per night were lost due to itch (Fig. 2).
Fig. 2. Disease burden for male and female patients. (a) Impairment of quality of life due to itch, assessed by the ItchyQol, (b) number of lost h of sleep, (c) anxiety score and (d) depression score assessed by the HADS. HADS-A/D: Hospital Anxiety and Depression Scale – Anxiety/Depression subscale. *p < 0.05.
Influence of sex and age in the clinical profile of chronic pruritus unknown origin
There were no differences between males and females with regard to itch intensity scores (p > 0.05) and presence of scratch lesions (p = 0.54). Females (2.7 [2.1; 3.2], n = 93) showed higher ItchyQol scores compared with males (2.3 [1.9; 3.0], n = 62; p = 0.04). Anxiety scores were higher in women (7.0 [4.8; 11.0], n = 122) compared with men (5.0 [3.0; 8.0], n = 94; p < 0.001), while no differences were recorded for depression scores (p = 0.28) or number of h of sleep lost (p = 0.59). Sex had no influence on the performed diagnostic work-up (p > 0.1).
There were no differences between older (≥ 65 years) and younger patients (< 65 years) with regard to itch intensity scores (p > 0.05), presence of scratch lesions (p= 0.08), impairment of quality of life assessed by the ItchyQol (p = 0.94), or amount of lost sleep (in h) (p = 0.99). Elderly patients (5.0 [3.0; 8.0], n = 69) had lower anxiety scores compared with younger patients (7 [4; 11], n = 147; p = 0.047), while no differences were observed for depression scores (p = 0.46). Compared with younger patients, elderly patients more frequently underwent medical imaging (42/86, 48.8% vs 62/177, 35.0%; p = 0.03) and skin biopsies (37/86, 43.0% vs 54/177, 30.5%; n = 0.045), whereas no differences were recorded for laboratory tests, quantification of serum antibodies and microbiological examinations (p > 0.1).
This study analysed a large cohort of patients with CPUO, which was diagnosed after comprehensive diagnostic efforts. The aim was to improve understanding of the clinical profile and burden of CPUO.
In general, patients with CPUO experience long-lasting moderate to severe itch. Remarkably, the majority of patients experience severe itch attacks, since 58.8% of patients included in the current study reported a worst itch intensity ≥ 7 on the VAS in the previous 4 weeks. Itch is present daily (68.2%), during the day and at night (66.3%), and occurs mostly in attacks (72.8%). Additional sensory symptoms, such as burning, tingling and stinging, accompany the itch in most cases (79.5%).
CPUO starts on non-lesional skin, as no primary dermatosis is present. In the course of the disease, secondary scratch lesions may develop, including chronic nodular prurigo lesions. Interestingly, patients with a shorter duration of pruritus (less than 6 months) seem to show more scratch lesions, suggesting that disease activity may be higher in the first months after onset. Remarkably, patients with scratch lesions are more burdened by the disease, as they perceive more intense itch and a greater impairment of sleep and quality of life. As such, special attention should be paid to this subgroup of patients. Xerosis and urticarial dermographism were common comorbid conditions, but neither related to onset or maintenance of pruritus.
Patients with CPUO show a moderate impairment of quality of life associated with sleep loss, as found in other studies including patients with CPUO (12) and in other cohorts of patients with CP; such as, for instance, CP arising from a small-fibre neuropathy (13). Importantly, almost all patients with CPUO reported sleep loss due to itch (97.2%), with a median of 2 h of sleep lost per night, confirming previous observations (12). Impairment of sleep should therefore be screened in all patients with CPUO, either by enquiring directly of the patients or by use of standardized questionnaires (14).
Even though no difference was recorded between males and females in itch intensity and presence of scratch lesions, women show a higher impairment of the quality of life and higher anxiety scores in the HADS in the current study. These findings are in agreement with previous data, demonstrating that women with inflammatory pruritic skin conditions and with CP accompanied by chronic scratch lesions are more impaired in their quality of life compared with male counterparts (15), and that females with CP of different origins are more anxious (but not more depressed) than men (16).
CPUO has been associated with pruritus in elderly patients. In part, this association is explained by a higher prevalence of CPUO in older patients (17); however, CP (regardless of its origin) is more prevalent at advanced ages (18). Age should not be a criterion for the diagnosis of CPUO, as this condition also occurs in younger patients. In fact, in our cohort the majority of patients (67.3%) were younger than 65 years. Importantly, elderly patients tend to have more comorbidities and may need more extensive diagnostic work-up to rule out a cause of CP. This was the case in the current patient cohort, in which older patients more often underwent skin biopsies and medical imaging.
In the current cohort, the diagnostic work-up revealed pathological findings in some cases. For instance, IgE was elevated in 44 patients, eosinophilia was found in 24 cases, and 9 patients showed histopathological findings compatible with pruritic skin conditions. However, these findings could not explain the CP according to the physician’s assessment, and thus these patients remained classified as having CPUO. Findings obtained from diagnostic investigations should always be interpreted critically, taking the clinical context and history into account. This is essential in order to avoid wrongly diagnosing an underlying condition for CP.
Remarkably, 41 patients (from 48 tested) in the current cohort showed a reduced IENFD. The determination of the IENFD constitutes the gold standard for the diagnosis of small-fibre neuropathy (19, 20), which can induce painful and pruritic sensations (13). Also, in neuropathic pruritic compression syndromes, such as brachioradial pruritus, nerve fibres in the epidermis are rarefied (21). Determination of the IENFD is not recommended in an initial screening of CP in current guidelines (2, 3). It is possible that diagnostic efforts beyond those advised by guidelines may be needed to unveil the underlying cause of CP in certain instances. Of note, the reduced IENFD alone is not sufficient for the diagnosis of a neuropathic pruritic condition and should be interpreted according to the clinical context, especially whether signs and symptoms of neuropathy (e.g. the presence of dysaesthesias, alleviation of the symptoms with cold or ice application, alloknesis and hyperknesis) are present.
The main limitation of this study is its single-centre design. Data were collected from a dermatological-based itch centre. Thus the clinical profile of CPUO treated at dermatological offices or general practitioners may differ. Most patients included in our analyses visited the centre only once (55.5%). It cannot be ruled out that further diagnostic efforts in subsequent visits would have led to the identification of the cause underlying CP. Another limitation is the missing data in some of the assessed outcomes, due to the retrospective nature of this study.
CPUO is a diagnosis of exclusion reflecting the absence of a known origin for CP. Patients with CPUO experience moderate to severe itch with a high disease-related burden. The presence of scratch lesions is associated with more severe itch and greater impairment in quality of life, while female patients are more burdened than male patients by the disease. Understanding the clinical profile and disease-related burden of CPUO is an important first step towards recognizing the impact of this condition on affected patients and the need for better care. Current guidelines recommend the use of several therapy options, including emollients, antihistamines, gabapentinoids and antidepressants, for the treatment of CPUO (3). However, high-quality data from longitudinal observations or randomized controlled trials are needed to establish which therapeutic approach is best suited to treat patients with CPUO. Physicians should be mindful of this condition and guideline recommendations in order to improve care.
Conflicts of interest. MPP is an investigator for Trevi Therapeutics; is a consultant for Galderma; and has received speaker honoraria/travel fees from Galderma, Lilly, Menlo Therapeutics, Novartis, and Trevi Therapeutics. AF has no conflicts of interest to declare. CZ has received speaker honoraria/travel fees from Beiersdorf and Dermascence. SSt is an investigator for Dermasence, Kiniksa, Galderma, Menlo Therapeutics, Novartis, Sanofi, Trevi Therapeutics and Vanda Pharmaceuticals, and is a consultant and/or member of the advisory board for Almirall, Bayer, Beiersdorf, Bellus Health, Bionorica, Cara Therapeutics, Celgene, Clexio Biosciences, DS Biopharma, Galderma, Menlo Therapeutics, Novartis, Perrigo, and Trevi Therapeutics.
This study was supported by a grant from the German Research Foundation (DFG) to SSt (STA1159/4-1). The funding agency had no role in the design of the study or in interpretation of the results.


 Click to show fullsize
Click to show fullsize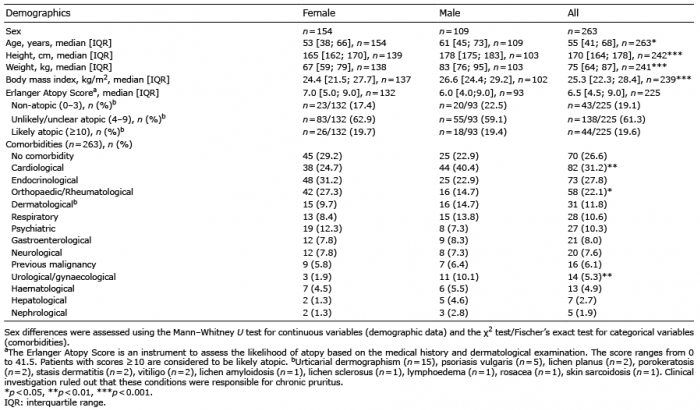 Click to show fullsize
Click to show fullsize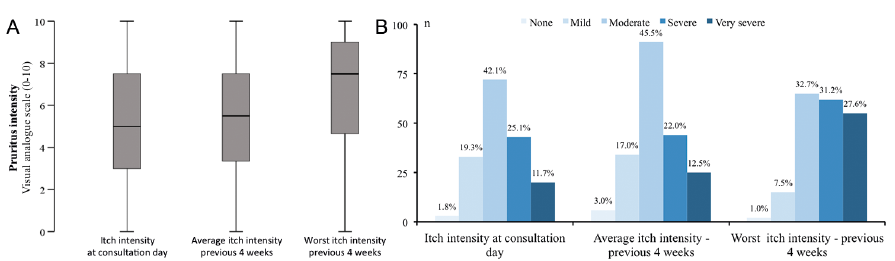 Click to show fullsize
Click to show fullsize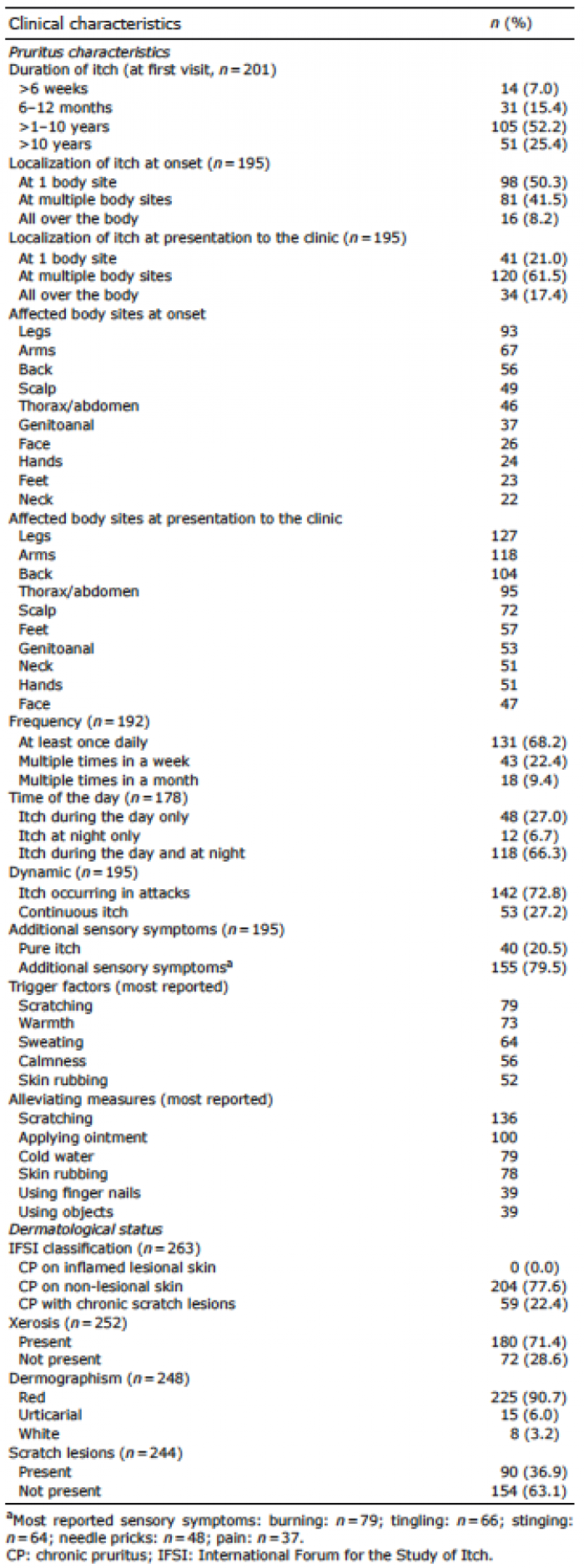 Click to show fullsize
Click to show fullsize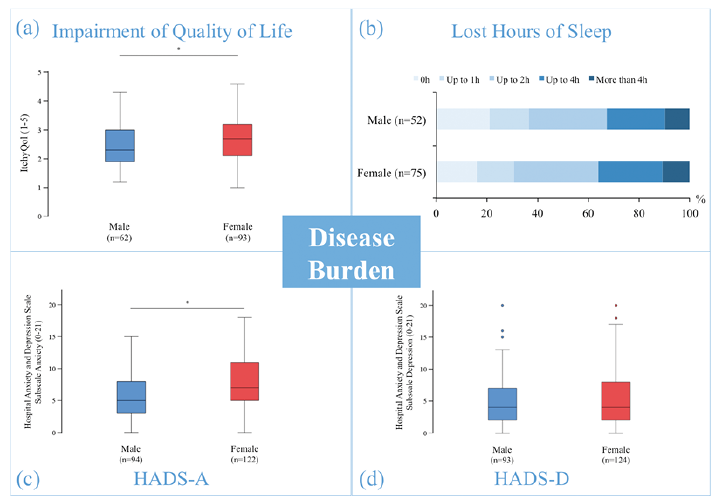 Click to show fullsize
Click to show fullsize