


Department of Dermatology, University Hospital Heidelberg, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. E-mail: Torben.Ramcke@med.uni-heidelberg.de
Accepted Aug 18, 2021; Epub ahead of print Aug 24, 2021
Acta Derm Venereol 2021; 101: adv00537.
doi: 10.2340/00015555-3903
Mycosis fungoides (MF), as T cell lymphoma, is the most common disease entity among the primary cutaneous lymphomas (1, 2). The current World Health Organization – European Organisation for Research and Treatment of Cancer (WHO-EORTC) classification defines a clinical and histopathological variant of MF, called folliculotropic MF, which is characterized by accentuation of follicular skin lesions (3). In the course of this disease, neoplastic T cells are prone to gather around the hair follicles (4–6). The objective skin manifestations are usually accompanied by moderate to severe pruritus (5, 7). In comparison with classical MF, skin changes in the course of follicular MF tend to occur in the head and neck region, in particular, involvement of the eyebrows was considered a characteristic finding in more than 50% of patients (4–9). We report here a case of a patient with folliculotropic MF in the tumour stage, who presented with ulcers on her lower legs mimicking a venous origin, which resulted in a diagnostic challenge in identifying the neoplastic genesis of the ulcers.
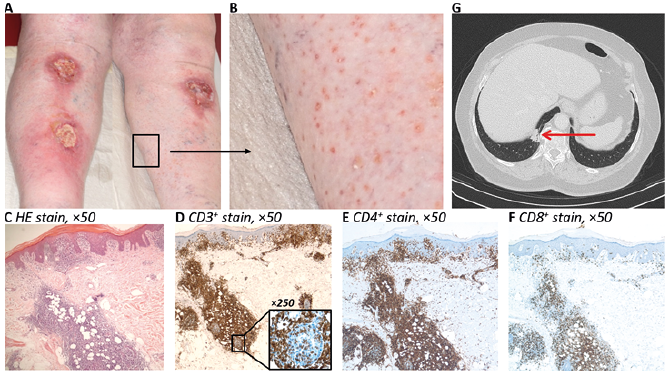
A 64-year-old Caucasian woman with ulcers on both sides of her lower legs visited our hospital. The ulcerations had existed for approximately 1 year and developed spontaneously with no exogenous trauma. Since Doppler sonography revealed pronounced superficial varicosis, the ulcerations were interpreted being due to chronic venous insufficiency. In addition, pre-existing type 2 diabetes and arterial hypertension were considered as co-factors compromising wound healing in this patient. Physical examination revealed 2 ulcerations, with a diameter of approximately 4 cm, on the right lower leg and another ulceration, with a diameter of 6 cm, on the left lower leg (Fig. 1A). Although typical signs of chronic venous insufficiency, such as corona phlebectatica and symmetrical oedema after orthostatic physical stress, were present, the proximal location of the wounds and the co-existing, pronounced pruritus prompted us to challenge this diagnosis. On inspecting the skin around the wounds, follicular bound, pinehead-sized, erythematous maculae and papules were noted, arousing suspicion (Fig. 1B). Similar skin changes were also present on the thighs and upper back. Surprisingly, histological analyses of a representative follicle revealed a pronounced infiltration of predominantly CD3+CD4+ T helper cells gathering around the adnexal structures (Fig. 1C–E). CD8+ cytotoxic T cells (Fig. 1F) or CD20+ B cells (not shown) were detected only to a small extent. Based on these findings, the following T-cell γ receptor rearrangement revealed a biclonal peak at 198 and 227 base pairs, confirming a suspected diagnosis of MF with folliculotropism. Similar findings were observed in specimens of the ulcers, so that a folliculotropic MF in the tumour stage was assumed. The primary staging excluded involvement of lymph nodes; but the right lower lobe of the lung revealed a pulmonary nodule (Fig. 1G). Biopsy of this lesion revealed neoplastic T cells, showing identical peaks in the T-cell γ receptor rearrangement compared with the cutaneous neoplastic infiltrates; consequently a pulmonary manifestation of MF was confirmed. To counteract the disease, combination therapy with psoralen plus ultraviolet A (PUVA) and peginterferon alfa-2a was initiated.
Fig. 1. Clinical and diagnostic findings of a patient with folliculotropic mycosis fungoides (MF) in the tumour stage. (A) Clinical presentation of the ulcers on the lower legs at first visit. (B) Enlarged illustration of the follicular-bound skin changes. (C) Haematoxylin and eosin (HE) staining showing a medium-wide epithelium. Below: there are dense infiltrates of lymphocytes, which have a tendency to exocytosis into the overlying epithelium and into the incised adnexal ducts. (Original magnification ×50). Immunohistochemical staining of (D) CD3+ T cells, (E) CD4+ T cells, and (F) CD8+ T cells (brown cell-surface staining, original magnification ×50). At the lower right edge of Fig. 1 (D), a hair encased by CD3+ T cells is shown at 400× magnification. The lymphocytic infiltrates predominantly reveal a CD3+CD4+ T helper cell phenotype. (E) Contrasted-enhanced arterial phase axial CT scan of the thoraco-abdominal region reveals a 23-mm diameter lung nodule in the right paravertebral costophrenic angle (red arrow).
This case shows tumour stage follicular MF with clinically apparent ulcerations on the lower legs and subtle, follicular-associated, skin lesions. Considering the absence of typical MF plaques and patches, diagnosis was difficult, especially as pronounced venous insufficiency was a plausible explanation for the leg ulcers. Eventually, follicular bound skin lesions led us to the correct diagnosis. In general, folliculotropic MF is prone to affect the skin of the neck and head (5, 6, 9); however, in the current case the lesions predominantly present on the lower extremities and lower back. Retrospectively, we speculated that the neoplastic T-cell lymphoma seen in the current case may have developed on the site of a pre-existing chronic wound in the context of venous insufficiency due to persistent immunostimulation. However, taking into account that, anamnestically, the ulcerations endured for only a short time (approximately 1 year), we favoured a primary origin for MF associated with chronic venous insufficiency. In line with recent reports attributing an unfavourable prognosis to follicular MF (7, 9, 10), the current patient had ulceration indicating a progressive tumour stage. Nevertheless, the short disease history, pulmonary manifestation and lack of MF-typical patches and plaques, was surprising, and highlights the aggressive potential of this MF subvariant. There is no standard therapy regime available for treatment of folliculotropic MF. In agreement with MF in general, it is believed that early-stage patients benefit from skin-directed therapy rather than aggressive, highly toxic chemotherapeutic approaches. Thus, the early stages of (follicular) MF are usually treated with topical corticosteroids and ultraviolet light therapy (PUVA and narrow band ultraviolet B). In the case of therapy resistance and in advanced stages of the disease, a combination of PUVA and interferon alpha and/or retinoids, local X-rays or, in very advanced stages, a (poly-) chemotherapy are used (7, 9). In the current case, due to the tumour stage with lung involvement, a combination therapy was started consisting of PUVA and peginterferon alfa-2a. This combination resulted in only a moderate response of the skin lesions and the lung nodule. Consequently, the therapy was changed, replacing peginterferon alfa-2a with bexarotene and initiating a topical radiotherapy of the lower legs, in the hope of disease control. The ulcerations on the legs have improved, a CT-morphological staging examination has not yet been carried out.
The case presented here highlights the differential diagnostic challenge clinicians face in treating chronic wounds. Last, but not least, although arguments for the common diagnosis of ulcers due to venous insufficiency were present, detailed inspection of the skin areas around the wounds led us to the correct diagnosis. In line with the recommendation of the European Wound Management Association (EWMA), this case report strongly supports that biopsy specimens should be taken from all atypical wounds and, in case typical-appearing wounds do not respond to topical treatment after 4–12 weeks, used to exclude a neoplastic origin (11). Secondly, although follicular MF is a rare disease entity, it should be integrated as a differential diagnosis in cases of follicular bound skin changes.
The authors thank the patient for approving the release of her medical data for use in this case report.
Conflicts of interest. AE received advisory honoraria from Biotest AG, MSD Oncology, Galderma, Janssen Cilag, AbbVie, and speaker’s honoraria from Roche Pharma.


 Click to show fullsize
Click to show fullsize