


1Celiac Disease Research Center, Faculty of Medicine and Health Technology, Tampere University, 2Department of Dermatology, 3Department of Gastroenterology and Alimentary Tract Surgery and 4Department of Internal Medicine, Tampere University Hospital, Tampere, Finland
Dermatitis herpetiformis is a cutaneous manifestation of coeliac disease treated with a gluten-free diet. However, the itching and blistering rash alleviates slowly after gluten withdrawal and occasionally persists despite a long-term gluten-free diet. This study investigated the prevalence and factors associated with prolonged (i.e. > 2 years) and ongoing skin symptoms in 237 patients with dermatitis herpetiformis. Data were gathered from medical records and via questionnaires. Among patients with dermatitis herpetiformis, 38% had prolonged symptoms after diagnosis, and 14% had ongoing skin symptoms at follow-up (median duration of gluten-free diet 24 years). A severe rash at diagnosis was associated with both prolonged and ongoing cutaneous symptoms. In addition, patients with dermatitis herpetiformis with ongoing skin symptoms at follow-up had been on the dietary treatment for a shorter time (median duration 16 vs 25 years) and were less often on a strict diet (53% vs 78%) compared with patients with dermatitis herpetiformis without ongoing skin symptoms.
Key words: dermatitis herpetiformis; coeliac disease; gluten-free diet; skin symptoms; dapsone.
Accepted Sep 2, 2021; Epub ahead of print Sep 7, 2021
Acta Derm Venereol 2021; 101: adv00555.
doi: 10.2340/00015555-3914
Corr: Camilla Pasternack, Celiac Disease Research Center, Faculty of Medicine and Health Technology, PO Box 100, FIN-33014 Tampere University, Finland. E-mail: camilla.pasternack@tuni.fi
Dermatitis herpetiformis is a blistering and itching skin disease and a skin manifestation of coeliac disease. Dermatitis herpetiformis is treated with a life-long gluten-free diet. This study showed that more than one-third of patients with dermatitis herpetiformis on a gluten-free diet have skin symptoms 2 years after being diagnosed, and 14% after long-term dietary treatment. More severe rash at diagnosis was associated with the persistence of skin symptoms, and those having skin symptoms despite a long-term gluten-free diet had a shorter duration and more lapses on their diet. This study emphasizes the importance of a strict and long-lasting gluten-free diet for patients with dermatitis herpetiformis.
Dermatitis herpetiformis (DH) is an autoimmune-based skin disease with an intensively pruritic and blistering rash affecting mainly the elbows, knees, and buttocks. DH is triggered by dietary gluten in genetically susceptible individuals, and it is currently widely recognized as a cutaneous manifestation of coeliac disease (1). In addition to the blistering rash, patients with DH have coeliac-type enteropathy, although this is often milder than in classical coeliac disease (1, 2). Also, approximately one-third of patients with DH have gastrointestinal symptoms, although the symptoms are typically mild, and overt gastrointestinal complaints are rare (2–4).
DH is treated with a life-long gluten-free diet (GFD). The GFD improves the small bowel mucosal pathology, alleviates the clinical symptoms, and reduces the risk of DH-associated complications, such as lymphoma (1, 5, 6). Gastrointestinal symptoms, if present at diagnosis, typically alleviate within 2 weeks of initiation of the GFD (7), but total clearance of the DH rash is much slower and may take several months or even a few years (5, 8). Consequently, additional treatment with dapsone (4,4’-diamino-diphenylsulfone), which reduces the itch and rash within a couple of days, is initiated for the majority of patients with DH at diagnosis (1). Dapsone treatment is gradually discontinued once the rash is controlled with a GFD alone, and the mean duration of dapsone treatment was approximately 2 years in previous studies (6, 9, 10). However, in some patients, much longer treatment periods are required due to the troublesome DH rash. In our previous study, patients with DH regularly using dapsone despite at least 3 years’ adherence to a GFD were defined as non-responsive, i.e. refractory DH patients (11). The condition was shown to occur in only 2% of patients with DH and regardless of ongoing skin symptoms, refractory DH was not associated with persistent villous atrophy or ongoing gastrointestinal symptoms (11), thus differing from refractory coeliac disease, which has a less favourable prognosis (12).
There are scarce contemporary data on the resolution of skin symptoms after diagnosis of DH and the initiation of a GFD. Furthermore, with the exception of our previous refractory DH study (11), knowledge regarding the persistence of skin symptoms in DH despite a GFD is largely lacking. Moreover, the factors related to the delayed clearance time of the DH rash after commencement of a GFD and the reasons for the ongoing skin symptoms despite the long-term GFD are yet to be elucidated. The aims of this study were to evaluate the prevalence of prolonged DH symptoms after diagnosis, and of the ongoing DH rash after long-term GFD adherence, and to study the associated factors.
Patients and study design
The Department of Dermatology at Tampere University Hospital hosts a special outpatient clinic for patients with DH, where all patients with DH living in the area of the surrounding city of Tampere are diagnosed. From 1970 onwards, data have been prospectively collected from all patients diagnosed with DH at Tampere University Hospital. In this study, follow-up questionnaires (described in detail below) were posted to all patients with DH diagnosed between 1970 and 2014, and the study protocol is explained in more detail elsewhere (13). A total of 237 out of 413 (56%) patients responded to the questionnaires, and these patients with DH comprised the current study cohort. In each patient, the diagnosis of DH had been based on typical clinical symptoms and the demonstration of dermal granular immunoglobulin A deposits in perilesional skin biopsies studied with direct immunofluorescence (14). In addition, all patients diagnosed with DH were routinely recommended to undergo gastroscopy and small-bowel biopsy at the time of the diagnosis according to the national guidelines of the time. After being diagnosed, all patients with DH were advised to adhere to a strict GFD, and a visit to a dietitian was recommended to all patients at the beginning of the diet. Dapsone medication was started for those with troublesome skin symptoms according to normal clinical protocol. The patients were followed up at the DH clinic by dermatologists for at least 1–2 years or until the rash was controlled by the GFD alone.
The study patients’ medical records from the time of diagnosis were reviewed. The duration and severity of skin symptoms, the presence of gastrointestinal symptoms, the severity of small bowel villous atrophy, the results of serum coeliac autoantibody tests at the time of DH diagnosis, and the initiation and duration of dapsone medication were documented from the medical records. The severity of the DH rash was recorded as mild, moderate, or severe according to the presence and amount of blisters, macular eruptions, and erosions in the typical DH rash locations and elsewhere. The severity of the small bowel biopsy finding, interpreted by an experienced pathologist, was graded into 3 groups: subtotal or total villous atrophy (SVA/TVA), partial villous atrophy (PVA), or normal mucosa. The serum coeliac autoantibody results recorded were IgA-class reticulin (ARA), endomysium (EmA), or transglutaminase 2 (TG2) antibodies. In the ARA and EmA tests, titres 1:≥5 were considered positive, and for TG2 antibodies, the reference values were dependent on the test kit used and defined by the test manufacturer of each test kit. The antibody test used was dependent on the time of the testing. These antibody tests have been shown to correlate well with each other in experienced hand (15, 16) and, in this study, all tests are collectively referred to as serum coeliac disease autoantibodies. The patients received a full written explanation of the study and gave their written informed consent. The Regional Ethics Committee of Tampere University Hospital approved the study protocol (R15143).
Questionnaires
The follow-up data were collected with 4 self-administered questionnaires. The Disease-Related Questionnaire (DRQ) was designed by dermatologists specialized in DH and was generated in order to gather follow-up data about patients with DH for research purposes. Quality of life was assessed with the Dermatology Life Quality Index (DLQI) and Psychological General Well-Being (PGWB) questionnaires, and the severity of the gastrointestinal symptoms was evaluated using the Gastrointestinal Symptom Rating Scale (GSRS). The DLQI, PGWB and GSRS questionnaires are validated questionnaires. Although they are not coeliac disease- or DH-specific, PGWB and GSRS questionnaires have been widely used in coeliac disease studies (17–20) and DLQI in various studies concerning DH and other skin diseases (21–24). Also the DRQ, although not validated, has been used previously in several DH studies (13, 21, 22, 25).
The DRQ is a questionnaire with both free-text questions and questions with multiple options. In addition to sociodemographic and lifestyle characteristics, the questionnaire includes questions about the duration of the skin and gastrointestinal symptoms prior to and after the DH diagnosis and the strictness of the GFD at the time of follow-up. The strictness of the diet was categorized into 4 groups: strict diet, no dietary lapses; dietary lapses less than once per month; dietary lapses more than once per month; and normal diet. In the DRQ, the use of dapsone and the presence of DH-related skin symptoms at the time of follow-up were also enquired. In addition, the presence of first-degree relatives with coeliac disease or DH, membership of Finnish Coeliac Society, and the height and weight of the patients were enquired. Body mass index (BMI) was calculated from the height and weight reported by the patients.
The DLQI is a 10-item questionnaire focusing on the impact of the skin disease on the patient’s quality of life over the last week. This dermatology-specific index contains aspects such as symptoms and feelings, daily activities, leisure, work or school, personal relationships, and treatment. Each question is scored with a 4-point Likert scale (0–3), giving the total DLQI score from 0 to 30, a higher score indicating worse quality of life (26).
PGWB covers 6 emotional states: anxiety, depressed mood, self-control, positive well-being, general health, and vitality. The questionnaire comprises 22 questions, and all the items use a 6-grade Likert scale, where a value of 1 represents the poorest and 6 the best possible well-being. The total score was calculated as a sum of all items and the subscores as a sum of 3–5 separate items composing each subscore. The PGWB total thus ranges between 22 and 132 points, a higher score representing better quality of life (27).
GSRS is a validated 15-item questionnaire widely used in coeliac disease studies. It covers symptoms in 5 categories: diarrhoea; indigestion; constipation; abdominal pain; and reflux (28). The questionnaire uses a 7-grade Likert scale for each item, with a score of 1 indicating no symptoms and 7 the most severe symptoms. The final scores were calculated as a mean for each sub-dimension and the total GSRS score as the mean of all 15 items. A higher score indicates more severe symptoms.
Prolonged skin symptoms after diagnosis of dermatitis herpetiformis and ongoing skin symptoms at follow-up
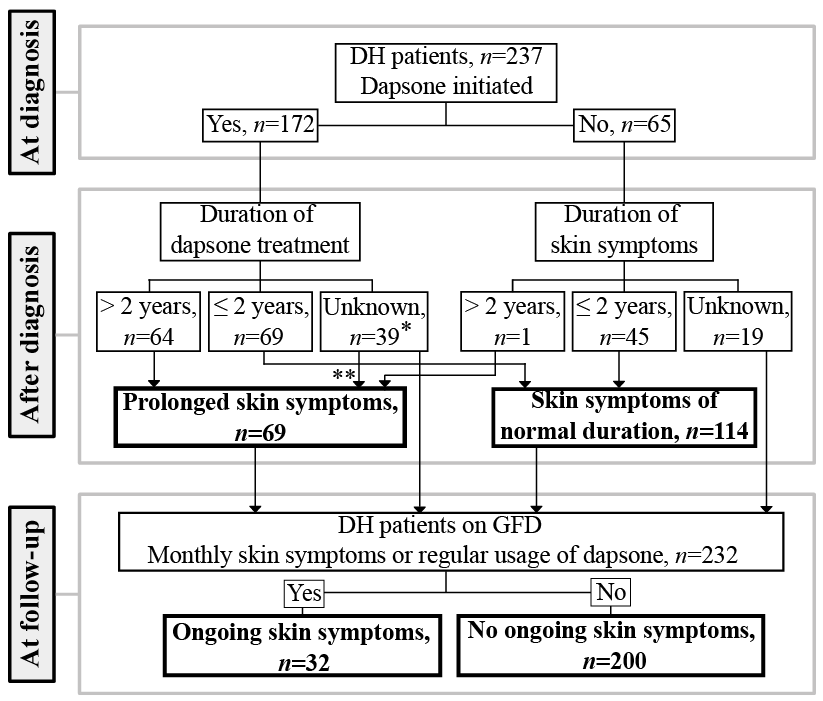
The patients with DH were categorized into 2 groups based on whether they had had prolonged skin symptoms after the DH diagnosis (Fig. 1). In this study, the skin symptoms were considered prolonged if they had endured for longer than 2 years after diagnosis. The definition was based on the clinical experience of the authors with a broad knowledge of DH, and on the previously reported data on the median durations of dapsone use in DH (6, 9, 10). Dapsone is initiated at diagnosis for those patients with DH with severe rash or itch, constituting approximately 65% of patients with DH (4, 29, 30), and it is discontinued as soon as the skin symptoms are controlled by the GFD alone. For that reason, dapsone is a reliable marker reflecting the length of DH skin symptoms, and therefore, the duration of skin symptoms after DH diagnosis was based primarily on the length of dapsone usage. In the DH patients not needing dapsone after being diagnosed, the prolongation of skin symptoms after diagnosis was based on the duration of the skin symptoms reported on the DRQ. Patients with an unclear duration of dapsone treatment and with self-reported skin symptoms shorter than 2 years were excluded from this analysis, as it remained unclear whether the skin symptoms had truly resolved within 2 years or been relieved due to ongoing dapsone (Fig. 1).
Fig. 1. Flow chart describing classification of the prolonged skin symptoms after dermatitis herpetiformis (DH) diagnosis and ongoing skin symptoms at the time of the follow-up study among the 237 patients with DH. GFD: gluten-free diet. *Among patients with an unknown duration of dapsone treatment, 2 patients had been followed-up for less than 2 years. **Among patients with an unknown duration of dapsone treatment, 4 patients with DH had had skin symptoms longer than 2 years and were thus categorized as having had prolonged skin symptoms after diagnosis.
In order to analyse the presence of ongoing skin symptoms at the time of follow-up, the patients with DH were further re-categorized based on the presence and occurrence of DH skin symptoms reported in the DRQ (Fig. 1). The skin symptoms were defined as ongoing if the self-reported DH-related skin symptom occurred at least once a month. In addition, patients with DH who reported at the DRQ using regular dapsone at the follow-up were also considered to have ongoing skin symptoms, as dapsone is used after long-term GFD adherence only when skin symptoms persist. Five patients were excluded from follow-up analysis: 4 patients reported not following a GFD and one patient had not responded to the question concerning the prevalence of skin symptoms at follow-up.
Statistical analysis
Median values, interquartile ranges (IQR), and minimum and maximum values were used to describe the continuous variables. All testing was 2-sided, and p < 0.05 was considered statistically significant. The χ2 test and Fisher’s exact test were used in cross-tabulations and the Mann–Whitney U test was used for assessing the differences between groups in continuous variables. All the statistical analyses were performed with SPSS version 26 (IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp. USA).
Of the 237 patients with DH, 47% were female and the median (IQR) age at DH diagnosis was 37 (27–50) years. Of these, 15 patients (6%) had had a prior diagnosis of coeliac disease (≥ 2 years earlier). After the diagnosis of DH, dapsone was initiated in 72% (172 out of 237) of patients, and the median (IQR) duration of dapsone treatment was 24 months (12–72, n = 134).
After the diagnosis of DH, 38% (69 out of 183 with available data) of the patients were found to have prolonged skin symptoms, and 64 out of those 69 had used dapsone longer than 2 years after diagnosis (Fig. 1). The patients with prolonged skin symptoms after diagnosis were diagnosed at a younger age and during an earlier diagnostic period than those without prolonged skin symptoms (Table I). The duration of skin symptoms prior to the DH diagnosis did not differ, but the skin symptoms had been more severe at the time of the diagnosis in those patients with prolonged skin symptoms compared with those without (Table I). The presence of gastrointestinal symptoms, the degree of small-bowel damage, and the serum coeliac disease autoantibody positivity at the diagnosis did not differ between the groups (Table I). Also, there were no differences between the groups in the previous diagnosis of coeliac disease or in the duration of gastrointestinal symptoms after the initiation of a GFD.
Table I. Diagnostic findings and factors at the time of the diagnosis associated with prolonged skin symptoms after diagnosis in 183 patients with dermatitis herpetiformis (DH)
At the time of the follow-up, the median duration of the GFD was 24 years (range 2–53 years) among the 232 patients with DH analysed for ongoing skin symptoms. Ongoing skin symptoms despite a long GFD were present in 14% (32 out of 232) of patients with DH at the follow-up (Fig. 1). Among patients with ongoing skin symptoms, 56% (18 out of 32) were using regular dapsone at the follow-up. The duration of skin symptoms prior to the diagnosis of DH did not differ between those with or without ongoing skin symptoms at the follow-up, but patients with ongoing skin symptoms had had a more severe rash at the time of the diagnosis (Table II), and they had more often had prolonged skin symptoms after diagnosis than those without ongoing symptoms (61% vs 34%, p = 0.011). Also, the median duration of the GFD was statistically significantly shorter (16 vs 25 years) and the adherence to the GFD less strict at the time of the follow-up among the patients with ongoing skin symptoms compared with those without (Table II). However, there were no statistically significant differences between the groups regarding the presence of first-degree relatives with DH or coeliac disease (41% vs 31%, p = 0.421) or in membership of the Finnish Coeliac Society at the time of follow-up (73% vs 65%, p = 0.386). In addition, the presence of gastrointestinal symptoms, the degree of small-bowel damage, and the serum coeliac disease autoantibody positivity at the diagnosis or the self-reported BMI at the time of the follow-up, did not differ between the groups (Table II).
Table II. Factors associated with ongoing skin symptoms at the time of the follow-up in 232 patients with dermatitis herpetiformis (DH) on a gluten-free diet (GFD)
Health-related quality of life measured with DLQI was lower in patients with ongoing skin symptoms compared with those without (Table II), although the majority of patients in both groups reported that the skin symptoms had no impact on their quality of life (Table II). The quality of life investigated with the PGWB questionnaire was statistically significantly lower only in the vitality subscore in those with ongoing skin symptoms compared with those without (Table II). The severity of the gastrointestinal symptoms measured with GSRS did not differ between the groups (Table II).
This study established that, in more than one-third of patients with DH, the skin symptoms endure longer than 2 years after the initiation of dietary treatment, and a more severe rash at diagnosis predicts prolongation of the skin symptoms after diagnosis. In addition, 14% of patients with DH had ongoing skin symptoms at follow-up despite long-term dietary treatment, and the duration of, and adherence to, a GFD were shown to have important roles in continuation of the skin symptoms.
Contemporary data concerning the duration of skin symptoms in DH after diagnosis and the onset of a GFD is scarce, and the few recent studies covering the subject have produced conflicting results (4, 31, 32). In the current study, 38% of patients with DH had skin symptoms enduring longer than 2 years after diagnosis and, among them, the majority (64 out of 69) were using dapsone longer than 2 years after diagnosis. The prevalence of prolonged skin symptoms in this study is rather high compared with our more recent study, in which only 13% of patients with DH were using dapsone after 2 years of adherence to a GFD (33). However, the few recent studies from other countries have reported that, despite strict adherence to a GFD, the majority of patients have been unable to stop dapsone during the first 2 years after diagnosis of DH (4, 32), giving even a higher prevalence of prolonged skin symptoms than in the current study.
The earlier diagnostic period was linked to the prolongation of cutaneous symptoms in DH in this study. During the earliest diagnostic period (1970–1984), even though the awareness of GFD as the main treatment for DH was increasing (5, 6, 34), the importance of strict adherence to a GFD was less obvious and, furthermore, the availability and selection of gluten-free products was not as good as during the later years. Thus, poorer adherence to a GFD after diagnosis might explain at least partly the prolongation of skin symptoms among those diagnosed during the earlier diagnostic period in the current study. Unfortunately, this assumption cannot be confirmed, as the data concerning GFD adherence during the immediate years after diagnosis were lacking. Also, a younger diagnostic age was linked to prolonged skin symptoms after diagnosis. However, we have previously shown an increase in the diagnostic age across the diagnostic periods in the DH population in this area (13), and it is plausible that the diagnostic period and possibly worse adherence to a GFD discussed earlier are more significant factors relating to prolonged skin symptoms than the diagnostic age. Furthermore, the study established that severe skin symptoms at diagnosis were linked to the prolongation of skin symptoms after diagnosis. Also, in coeliac disease, the severity of the gastrointestinal symptoms at diagnosis has been shown to predict the persistence of gastrointestinal symptoms despite a strict GFD (35). However, intriguingly the duration of skin symptoms prior to diagnosis of DH was not associated with prolonged skin symptoms after diagnosis, although in coeliac disease the long duration of gastrointestinal symptoms also predicted the persistence of such symptoms (35). Moreover, the prolongation of skin symptoms was not linked to the severity of gastrointestinal disease in DH, as the presence of gastrointestinal symptoms and the degree of small bowel mucosal damage at diagnosis did not predict the resolution time of skin symptoms after diagnosis.
The prevalence of skin symptoms in DH after a long-term dietary treatment has been described in a study by Lheure et al. (4), who found that, among their study cohort, 13% of patients with DH treated for a median of 14 years had skin symptoms despite a GFD. In addition, in a different series we have shown that 17% of patients with DH treated with a GFD for a median of 18 years had skin symptoms at the time of the study (36). The results of this study are consistent with the previous findings, although this study had a significantly longer follow-up time than the others. The current study also revealed that patients with ongoing skin symptoms at follow-up were more likely to have had severe skin symptoms at diagnosis and prolonged skin symptoms after diagnosis. Also, the duration of the diet was significantly shorter among those with ongoing skin symptoms compared with those without. These findings suggest that, occasionally, skin symptoms in DH resolve extremely slowly with a GFD, and that the severity of the skin symptoms at the time of the diagnosis might be a factor predicting the time for symptom resolution on a GFD. Moreover, the self-reported adherence to a GFD at the time of follow-up was markedly worse among those with ongoing skin symptoms compared with patients with DH without such symptoms, despite that factors affecting the awareness of GFD, such as being a member of a coeliac society or having first-degree relatives with DH or coeliac disease, did not differ between the groups. Adherence to a GFD is generally very good in the study area, as over 90% adherence rates have been reported in patients with DH and coeliac disease in previous studies (30, 35–37). However, among those with ongoing skin symptoms, only 56% reported following a strict GFD at the follow-up, and this finding further highlights the importance of a strict GFD in DH, and shows that even occasional lapses in the diet might lead to the activation of skin symptoms.
Previously, patients with DH with untreated skin symptoms have been shown to have decreased quality of life (3), but with treatment the life quality increases to a level comparable to the general population (36). This study showed that, despite a long-term GFD, ongoing skin symptoms impacted slightly on the DH patient’s quality of life, as the DLQI score was higher and PGWB vitality subscore was lower among the patients with DH with ongoing skin symptoms compared with those without. However, the majority of patients considered the skin symptoms to have no effect on their quality of life, which was surprising, as generally skin diseases are considered to greatly impact the quality of life of patients (38). Nevertheless, in this study, patients regarded as having ongoing skin symptoms were, for the most part, those using dapsone despite long-term adherence to a GFD, and it is presumed that regular dapsone usage effectively controls the skin symptoms and minimizes the quality of life effects of the dermatological symptoms.
Strengths and limitations
The strengths of this study were the large cohort of patients with a biopsy-proven diagnosis of DH followed-up by dermatologists specialized in DH. Moreover, the patients were gathered from an area with a high prevalence of DH, good GFD adherence rates, and a wide availability of gluten-free products (30, 39). Also, the follow-up time was long, up to 50 years. A limitation of this study is that the follow-up data were gathered with questionnaires, which might have caused a selection bias, as the population willing to respond to the questionnaires might differ from those not participating. In addition, recall bias might affect the results due to the very long follow-up times in this study. There are also some studies reporting spontaneous remission in patients with DH on a gluten-containing diet (40, 41). However, since spontaneous remission in DH was shown to be rare in our recent study demonstrating a 95% relapse rate among gluten-challenged patients with DH within 12 months (42), it is unlikely that this would have contributed significantly to the results of this study. Another limitation was that no clinical or laboratory evaluations were conducted at the time of the follow-up, and thus the nutritional status and presence of circulating coeliac autoantibodies at the time of follow-up could not be evaluated, and the management of GFD was based solely on patients’ self-reported estimation. Furthermore, a relatively high proportion of patients with DH were excluded from the classification concerning the prolongation of symptoms, due to insufficient data, which might bias the estimate about the prevalence of prolonged skin symptoms in this study group.
Conclusion
This study found that prolonged skin symptoms after diagnosis are common in DH, and the slow resolution of the DH rash seems to be more likely in those having severe skin symptoms at diagnosis. Also, ongoing skin symptoms despite long-term GFD adherence affected 14% of patients with DH, and in addition to a more severe rash upon diagnosis, GFD duration and adherence were significant factors associated with ongoing skin symptoms. The study thus suggests that, in a minority of patients with DH, resolution of DH rash is a remarkably delayed process, and also, even slight dietary transgressions can result in an ongoing rash. In conclusion, patients with DH who have a severe DH rash when diagnosed should be followed up with care. Life-long, strict adherence to a GFD is of utmost importance in patients with DH.
This research was funded by the Academy of Finland, the Emil Aaltonen Foundation and Competitive State Research Financing of the Expert Responsibility Area of Tampere University Hospital (grants 9X051, 9AA026, 9AA070).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize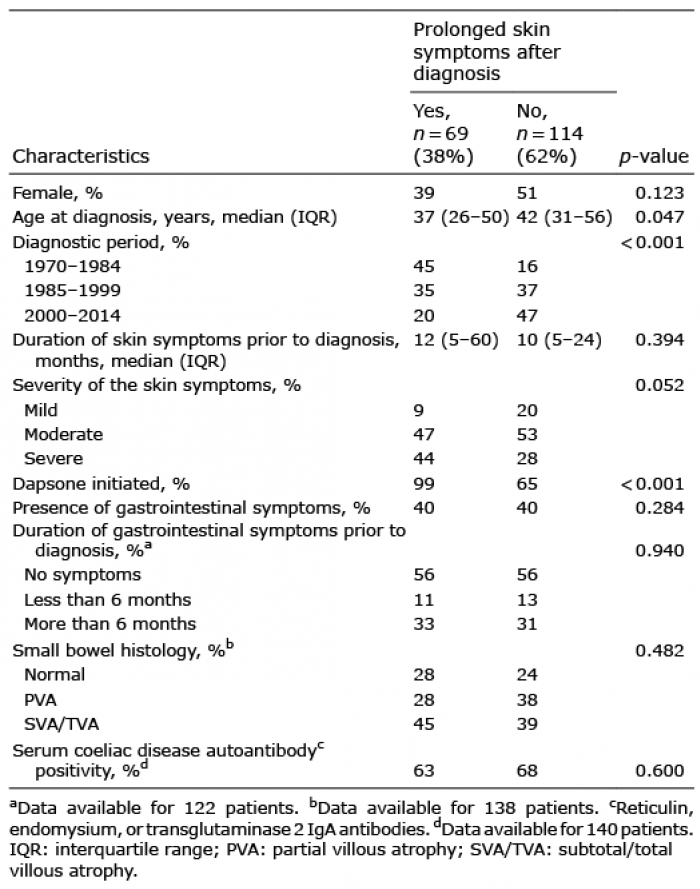 Click to show fullsize
Click to show fullsize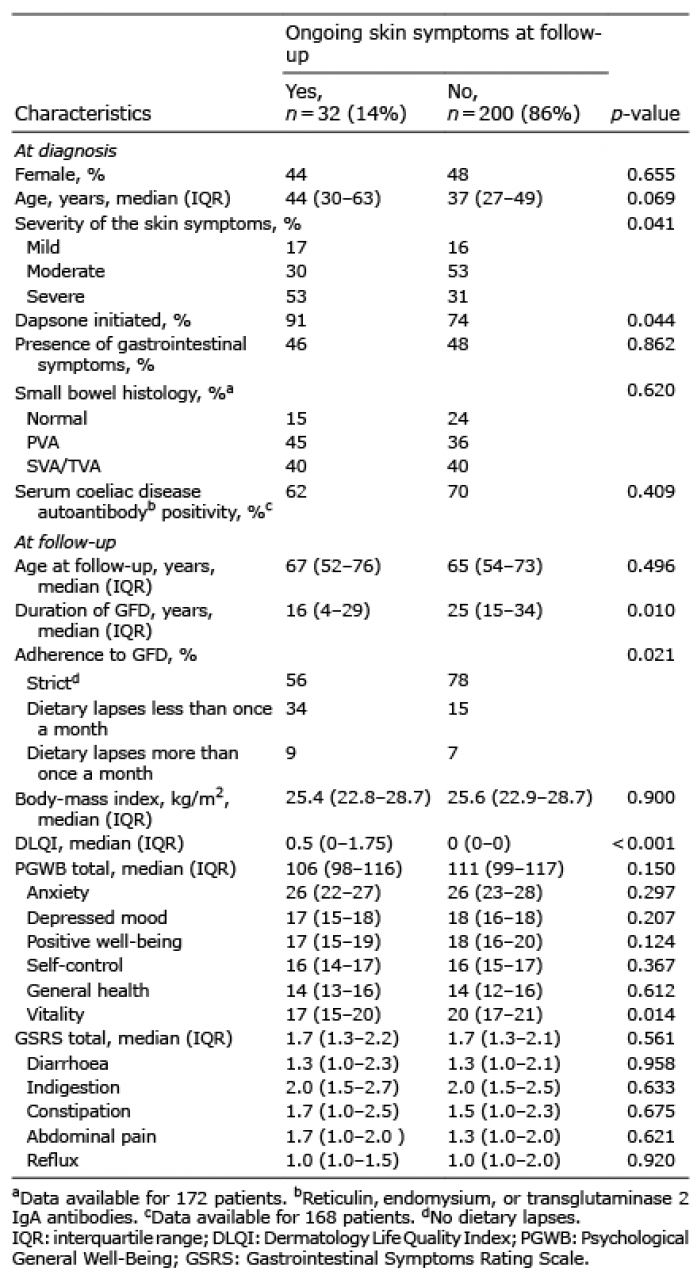 Click to show fullsize
Click to show fullsize