


1Department of Dermatology, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan and 2School of Health Care Administration, College of Management, Taipei Medical University, Taipei, Taiwan
Atopic dermatitis has a substantial impact on work and activity impairment according to studies from Western communities. Prospective studies of work productivity and activity impairment in Asian patients with atopic dermatitis are lacking. The aims of this study were to investigate the impacts of atopic dermatitis on work productivity and activity impairment among Taiwanese patients, and to stratify the analyses by disease severity. One-third of employed participants reported missing work (absenteeism) in the preceding week due to atopic dermatitis, while 88.5% of the remaining two-thirds reported impaired work effectiveness (presenteeism). In addition, 92.5% of all participants reported impaired daily activities. Overall work impairment (aggregate productivity loss from absenteeism and presenteeism) was 1.8- and 2.6-fold greater in subjects with moderate and severe atopic dermatitis, respectively, compared with those with mild atopic dermatitis. Presenteeism, but not absenteeism, contributes to the majority of total work impairment in this cohort. Daily activity impairment was 1.5-fold greater in moderate atopic dermatitis, and 2.0-fold greater in severe atopic dermatitis, compared with mild atopic dermatitis. Both work and activity impairment showed significant positive correlations with atopic dermatitis severity scores (SCORing Atopic Dermatitis; SCORAD). In conclusion, work productivity and activity impairment is significantly correlated with disease severity in this Taiwanese atopic dermatitis cohort. In order to obtain a full picture of disease burden to patients and caregivers, patients with atopic dermatitis should be monitored for disease activity as well as corresponding impacts on quality of life.
Key words: atopic dermatitis; work productivity and activity impairment; work impairment.
Accepted Sep 2, 2021; Epub ahead of print Sep 7, 2021
Acta Derm Venereol 2021; 101: adv00556.
doi: 10.2340/00015555-3918
Corr: Chao-Hsiun Tang, School of Health Care Administration, College of Management, Taipei Medical University, 250 Wu-Xin Street, Taipei 11031, Taiwan and Chia-Yu Chu, Department of Dermatology, National Taiwan University Hospital and National Taiwan University College of Medicine, 7 Chung-Shan South Road, Taipei 10002, Taiwan. E-mails: chiayu@ntu.edu.tw; chtang@tmu.edu.tw
Pruritus and the negative effect on appearance due to atopic dermatitis have a considerable impact on affected individuals, leading to substantial impairments in work and daily activity. Through analysis of work productivity and activity impairment in patients with atopic dermatitis, the current study demonstrated that presenteeism has a far greater impact on atopic dermatitis-related productivity loss than does absenteeism. Interventions aiming to reduce productivity loss due to atopic dermatitis should prioritize addressing presenteeism-induced work impairment. Detailed work productivity and activity impairment scores could change how health systems and policymakers engage in improving care for patients with atopic dermatitis.
Atopic dermatitis (AD) is a common inflammatory skin disease characterized by a relapsing course of chronic pruritus and eczema. Although AD typically first manifests during childhood and may resolve spontaneously at puberty, some patients have persistence of AD into adulthood, while others first develop AD after adolescence or even in adulthood. The pruritus and negative effect on appearance caused by this disease have a great impact on patients with AD, which lead to work productivity and activity impairment. Typical measures of AD severity, such as severity SCORing of AD (SCORAD) and Eczema Area and Severity Index (EASI) scoring systems, do not adequately reflect the substantial impacts of AD in terms of work productivity and activity impairment. Several tools have thus been developed for evaluation of AD-related quality of life and daily performance impairment (1–3). The WPAI-AD (Work Productivity and Activity Impairment – Atopic Dermatitis) questionnaire is an adequate and feasible tool for reliably assessing an AD patient’s overall health condition. Using WPAI-AD scoring, the work productivity losses of individuals can be quantified as a representative and integrated numerical value/score in addition to the disease status (3).
A total of 200 adult patients with AD were recruited to this study. Their WPAI-AD information was collected. Each patient’s total work productivity loss (TWPL) was calculated, based on their absenteeism and presenteeism, and the total activity impairment (TAI) due to AD was recorded (3). The data indicated significant negative impacts on work productivity and daily activity with increasing AD severity. In addition, the impacts of AD WPAI from different ethnic groups, including Asian and Western patients, were compared. Similar trends were found among patients of different ethnicities, demonstrating incrementally increased WPAI impacts with increased AD severity levels. These findings address the importance of considering these often neglected, but major impacts of AD on work productivity and daily activity.
Study designs and patient recruitment
This cross-sectional interview survey recruited adult patients with AD from October 2018 to April 2019 at their regular follow-ups in 3 hospitals located in northern, central, and southern Taiwan. The inclusion criteria required the selected individuals to be at least 20 years old, diagnosed with AD by board-certified dermatologists (according to the 1980 Hanifin and Rajka criteria), and treated regularly by AD specialists for more than 6 months. The patients were stratified into 3 severity groups according to their SCORAD scores, determined by specialist evaluations and patient-oriented symptoms: mild: SCORAD score < 25; moderate: SCORAD score 25–50; and severe: SCORAD score > 50 (4).
All participants provided informed consent prior to being interviewed. The study was approved by the ethics committee of National Taiwan University Hospital (201802007RINA).
Measurement of the adverse effects on work productivity and activity
The impacts of AD were assessed using the WPAI-AD questionnaire (1). This questionnaire is an instrument that has been well validated across different languages and contains 6 questions: Q1 asks if the respondent is currently employed; Q2 asks if the respondent has missed hours at work due to health problems; Q3 asks if the respondent has missed hours at work due to other reasons; Q4 asks how many hours the respondent has actually worked; Q5 asks the degree to which the respondent’s health has affected the respondent’s productivity while working; Q6 asks the degree to which the respondent’s health has affected the respondent’s productivity in regular unpaid activities. The respondent is asked to recall the preceding 7 days in answering questions Q2–Q6. The following 4 impairment scores could be yielded and expressed in percentages, with higher values indicating greater impairment and less productivity. (i) Absenteeism (percentage of work time missed due to AD)=Q2/(Q2+Q4) for those who were currently employed. (ii) Presenteeism (percentage of on-the-job ineffectiveness due to AD)=Q5/10 for those who were currently employed. (iii) Overall work impairment (aggregate of absenteeism and presenteeism)=Q2/(Q2+Q4)+[(1- (Q2/(Q2+Q4)))x(Q5/10)] for those who were currently employed. For those who had not worked at all due to AD during the preceding 7 days, the overall work impairment value is equal to the absenteeism value. (iv) Activity impairment (percentage of daily activity impairment due to AD)=Q6/10 for all participants.
Statistical analysis
Descriptive statistics were used to characterize the patients, by level of AD severity, using numbers and percentages for categorical variables, and means and standard deviations (SDs) for continuous variables. Differences in baseline demographics among groups were assessed by χ2 tests, t-tests, or one-way analysis of variance (ANOVA). Crude values for the 4 types of impairment scores were presented, by level of AD severity, as numbers and percentages for the patients with 0 scores, and as means, SDs, medians, and interquartile ranges (IQRs) for the patients with non-zero scores. Regression-adjusted values of the impairment scores were computed using 2-part generalized linear models with beta distributions with the level of AD severity as the main independent variable and while controlling for sex, age, body mass index (BMI), education, marital status, and household income. Differences in the mean adjusted values of the impairment scores among the different levels of AD severity were then assessed by ANOVA. A statistical significance of 0.05 was adopted.
All analyses were performed using SAS/Stat system for Windows, version 9.4 (SAS Institute, Cary, NC, USA).
Patient characteristics
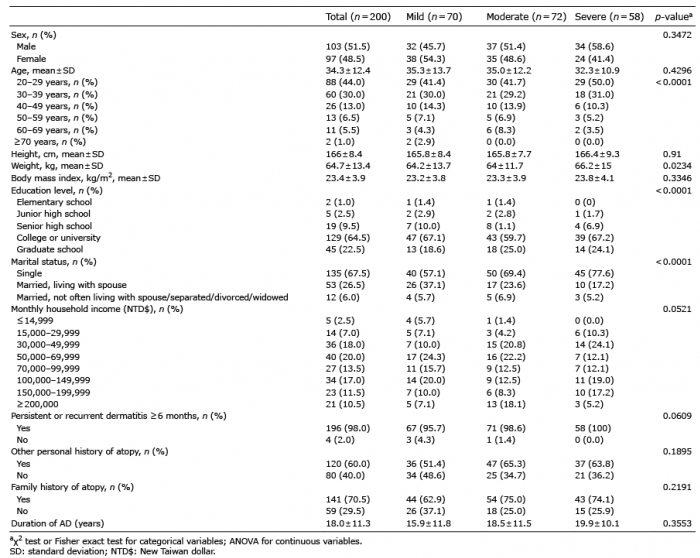
A total of 200 patients with AD were recruited. Of these, 70 had mild AD, 72 had moderate AD, and 58 had severe AD. Overall, the patients had a mean (SD) age of 34.3 (12.4) years, a mean duration of AD of 18.0 (11.3) years, and a mean SCORAD score of 35.8 (18.5). The majority of the patients were single (67.5%) and had a college level of education or above (87.0%) (Table I). Those with more severe AD tended to be younger, to have higher education and lower income levels, and to be single. There were no significant differences in terms of sex, BMI, or the duration of AD among patients with different levels of AD severity.
Table I. Demographic and socioeconomic characteristics of participants, stratified by severity level of atopic dermatitis (AD)
Atopic dermatitis severity and impact on work productivity and activity impairment
The WPAI yields 4 types of scores, including absenteeism (work time missed), presenteeism (impairment at work/reduced work-hour effectiveness), work productivity loss (overall work impairment from absenteeism plus presenteeism), and activity impairment (1). The outcome scores are expressed as impairment percentages, with higher numbers indicating greater impairment. Both absenteeism (unscheduled absence) and presenteeism (at work with hampered performance) contribute to loss of work productivity. In this study, of the 139 (69.5%) patients who were currently employed, 51 (36.7%) reported missing work (absenteeism) in the past week due to AD (Table II). Only 16 (11.5%) reported that their actual work was not impaired (presenteeism). The median scores of absenteeism and presenteeism were 9.1 and 40.0, respectively. When absenteeism and presenteeism were both considered, 124 (89.2%) of the employed patients reported either missing work or having impaired work, with the median score of overall work impairment being 50.0. In addition, 185 (92.5%) out of all participants reported regular daily activities had been restricted due to AD, and the median score was 40.0.
Table II. Crude values and regression-adjusted values of absenteeism, presentism, work impairment, and activity impairment, stratified by severity level of atopic dermatitis (AD)
The adjusted score of absenteeism increased from 1.8 ± 1.3 (mean ± SD) for patients with mild AD to 6.3 ± 2.7 for patients with moderate AD and 5.6 ± 3.3 for patients with severe AD. The adjusted score of presenteeism rose steadily from 23.7 ± 13.6 for patients with mild AD to 42.1 ± 10.3 for moderate AD and 63.1 ± 9.0 for severe AD (Table II). Combining the negative impacts of absenteeism and presenteeism, the adjusted score of overall work impairment increased as the AD severity increased, which was 24.7 ± 13.1 for patients with mild AD, 44.8 ± 10.1 for moderate AD, and 65.0 ± 7.8 for severe AD. Similarly, as the AD severity increased, the adjusted score of activity impairment became greater, which was 29.9 ± 10.1 for patients with mild AD, 44.7 ± 9.6 for moderate AD, and 61.2 ± 8.7 for severe AD (Table II).
The mean adjusted overall work impairment scores were 1.8- and 2.6-fold greater, respectively, in those with moderate AD and severe AD compared with those with mild AD (p < 0.001), while the mean adjusted activity impairment was 1.5-fold greater in those with moderate AD compared with mild AD (p < 0.001), 2.0-fold greater in those with severe AD compared with mild AD (p < 0.001), and 1.4-fold greater in those with severe AD compared with moderate AD (p < 0.001) (Fig. 1).
Fig. 1. Atopic dermatitis severity and the impact on work productivity and activity impairment. (a) Regression-adjusted means of work impairment (n = 139) and (b) regression-adjusted means of activity impairment (n = 200), stratified by severity level of atopic dermatitis. SCORAD: SCORing Atopic Dermatitis.
Associations between atopic dermatitis severity scores and impairment
Both adjusted scores for work impairment and adjusted scores for activity impairment showed significant positive correlations with the SCORAD and oSCORAD (objective SCORAD) AD severity scores (p < 0.001) (Fig. 2).
Fig. 2. Associations between atopic dermatitis (AD) severity SCORing Atopic Dermatitis (SCORAD) and objective SCORing Atopic Dermatitis (oSCORAD) scores and impairment. (a, c) Work impairment and (b, d) activity impairment.
WPAI has been used widely in evaluating disease burden, such as in psoriasis and psoriatic arthritis (5–8). In psoriasis, WPAI has been consistently found to correlate with disease severity, quality of life, and socioeconomic burden. Recent studies have also attempted to use this measure to compare the therapeutic responses in psoriatic diseases (9–11) from varying treatments as well as varying ethnic backgrounds. As a major inflammatory skin disease, AD would have an impact in WPAI. However, regional treatment recommendation has not considered WPAI in the development of consensus for the management of AD (12). The importance of understanding the impact is not solely for physicians to recognize the severity on patients’ lives, but also for healthcare systems and policymakers to engage in the improvement in AD care. It is very important to demonstrate the substantial impacts on work and daily life of patients with AD by direct feedback from affected individuals (13). To explore the real-world burden of AD, patients were recruited from different regions of Taiwan. To avoid overestimations of absenteeism and reduced performance at work caused by unexpected medical appointments due to the aggravation of AD, all participants were recruited from their already scheduled regular follow-up visits. Possible confounders were adjusted to avoid statistical biases affecting the primary variables of interest. It was found that, with or without the control of confounding variables, the trends of impact of AD on work and daily activity across mild to moderate to severe AD remained consistent.
Two major components of disease burden in this cohort, presenteeism and activity impairment, showed consistently higher impacts with greater severity levels of AD. Overall, the employed AD subjects reported 43.8% work impairment (or lost work productivity). And the severe AD group experienced lost productivity nearly 3 times greater than that of subjects with mild AD. Similarly, there was a distinct incremental trend in activity impairment across the 3 severity groups, indicating that more severe AD has greater impacts on daily activity. The significantly high activity impairment scores reflect the adverse effects of AD in maintaining the basic activities of daily life among patients with severe AD. Significant differences in absenteeism and work impairment were also observed when comparing moderate or severe AD with mild AD, although moderate AD and severe AD did not appear to have a statistically significant difference in absenteeism compared with each other (6.3 ± 2.7 vs 5.6 ± 3.3) (Table II).
To further demonstrate the relationships between severity of AD and the impacts of the disease on work and daily life, the strengths of the relationships between relevant quantitative variables were evaluated, namely, SCORAD and oSCORAD (objective SCORAD) with work impairment scores and with activity impairment scores. The adjusted scores for both work and activity impairment showed significant positive correlations with severity of AD (p < 0.001), indicating that the more severe the AD, the greater the impacts the disease had on the work productivity and daily activity of the patients with AD. These findings from our study were consistent with studies of patients with AD from other ethnic groups with the same conclusion: the more severe the AD, the worse the impacts on work and daily life (3, 12, 13).
It should be noted that absenteeism was not the major culprit in work productivity losses. Presenteeism contributed nearly 90% of the total weekly work impairment due to AD, while only 10% of the impairment came from absenteeism. In other words, presenteeism, which is measured by self-reported occupational efficacy loss (when employees attend for work, but are unable to perform at full capacity), has a far greater impact on AD-related productivity loss than does absenteeism. These results suggest that interventions aiming to reduce productivity losses should prioritize addressing presenteeism-induced productivity losses.
The data presented in this study reveal the impact of AD on work productivity and daily activity in Taiwan. Studies from East Asian (Japan) and Western societies (European countries and the USA) showed comparable impacts on work and daily life (3, 12). Similar to the current study, working productivity impairment due to presenteeism is a major burden to employers and employees in both Asian and Western societies. However, although seemingly consistent in presenteeism-predominant productivity loss among Taiwanese, Japanese, and Western societies, the comparison might be skewed, requiring rectification due to the intrinsic demographic and job type differences of the participants in the studies.
These findings regarding patients with AD from different ethnic groups simply reflect, to some extent, that the current treatments for AD remain insufficient for overcoming the burdens brought by AD around the world. The results of the current study reveal that AD-related productivity loss and activity impairment is a major issue that greatly impacts affected individuals and the working environment in Taiwan. The overall impact on work productivity and daily activity due to AD correlates with the severity of the disease. Therefore, with the help of detailed WPAI records and the underlying significance, more aggressive therapeutic strategies and interventions for improving AD care should prioritize the restoration of work performance and daily activity.
Study limitations
While WPAI serves as a useful reference of the socioeconomic burden of patients with AD, it should be noted that the financial and life quality impact due to AD may vary significantly from job to job. Since the majority of Taiwan’s workforce is made up of white-collar workers, most of the participants in the current study were employed in an office-based or indoor environment. In consideration, WPAI analysis in this study may not reflect and accurately apply in labour-intensive populations. Furthermore, the current study population, although randomly selected from clinics, aiming to be representative of the demographic composition of the general population, may not reflect well on stratified groups, such as elderly patients or less-educated populations, as the proportion of college or above education levels is 87% (which is higher than that of the general population in Taiwan).
Conclusion
Given that AD is one of the leading causes of skin disease-related burdens worldwide, it is unsurprising that the current results indicate profound negative impacts of AD on work productivity and daily activity among Taiwanese patients with AD. From a public health perspective, improving the healthcare efforts aimed at reducing the impacts of AD on daily productivity and general activity is a key strategy that needs to be implemented on larger nationwide and worldwide scales in order to decrease the negative personal and economic impacts of the disease.
The authors would like to thank Ms Wen-Ting Hsieh, Ms Li-An Hsu, and Mr Dereck Shen for scientific discussions during all phases of the study, and the staff of the Eighth Core Laboratory, Department of Medical Research, National Taiwan University Hospital, for their support.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize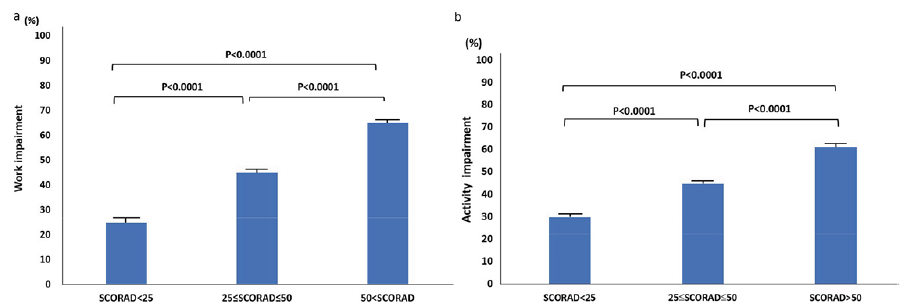 Click to show fullsize
Click to show fullsize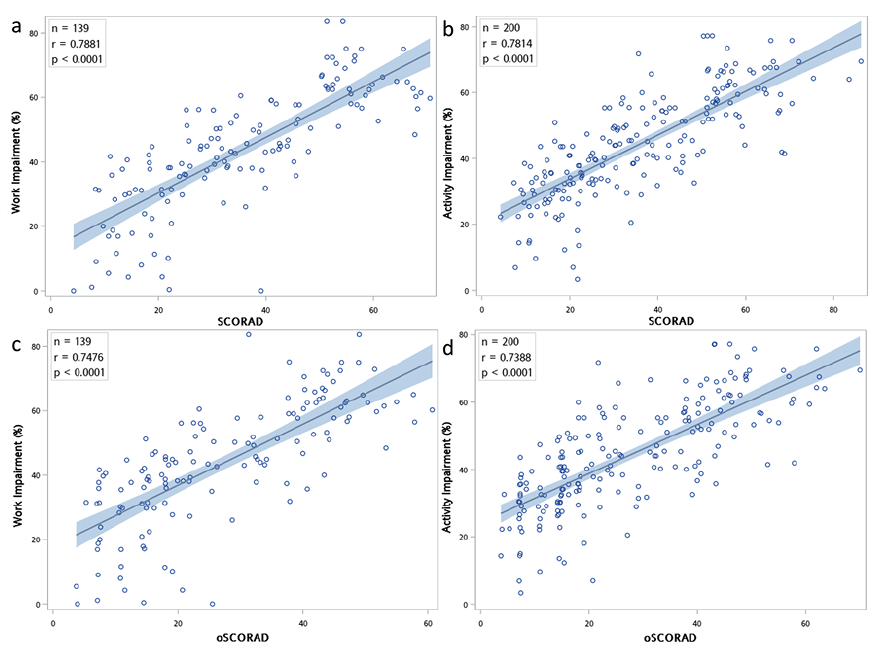 Click to show fullsize
Click to show fullsize