


1Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Münster and 2Department of Dermatology and Allergy, Technical University of Munich, Munich, Germany
Human hands are complex structures essential for a variety of functions in everyday life. This study prospectively investigated the clinical features of hand pruritus and the resulting functional impairment and disease-related burden in 395 patients with chronic pruritus (210 females, median age 59 years). Moderate to very severe hand pruritus was reported by 91.2% of patients, while 79% perceived additional sensory symptoms, such as burning, pain or tingling. A long duration of pruritus occurred in most cases (> 6 months: 71.4%). A considerable proportion of patients showed moderate to severe impairment in the use of their hands (40.2%), performance of daily activities (65.0%) and quality of life (45.2%). Disease severity and burden is particularly high when both the palms and the backs of the hands are affected, and when pain is present simultaneously. Pruritus located on the hands is impairing and burdensome due to the functional relevance of the hands in everyday life.
Key words: chronic pruritus; itch; hands; burden; quality of life; patient-reported outcomes.
Accepted Sep 8, 2021; Epub ahead of print Sep 13, 2021
Acta Derm Venereol 2021; 101: adv00562.
doi: 10.2340/00015555-3925
Corr: Manuel P. Pereira, Department of Dermatology and Center for Chronic Pruritus, Von-Esmarch Str. 58, DE-48149, Münster, Germany. E-mail: manuelpedro.pereira@ukmuenster.de
Human hands are complex and essential for daily activities. This study investigated the clinical features of hand itch in 395 patients with chronic pruritus. In the majority of cases, long-lasting moderate to very severe hand itch intensity, and additional symptoms, such as burning, pain or tingling, were observed. A considerable proportion of patients showed moderate to severe impairment in the use of the hands, performance of daily activities and in quality of life. Disease severity and burden is particularly high when both the palms and the backs of the hand are affected and when pain is present simultaneously.
The human hand is a complex, sophisticated structure that plays a pivotal role in everyday life. Its proper use is essential for a myriad of functions, such as sensory perception, manipulation of objects and communication. Functional impairment of the hand greatly reduces the use of the affected limb, as is the case, for example, in patients with severe rheumatoid arthritis or systemic sclerosis (1).
Skin diseases affecting the hands represent a substantial toll for affected patients. The impairment of quality of life in patients with dermatoses of the hand, such as hand eczema or psoriasis, is well documented (2, 3). When affecting the hand, skin conditions generally lead to much higher distress and dysfunction compared with lesions located elsewhere in the body (4). Moreover, hand dermatoses, especially chronic hand eczema, constitute a substantial occupational hazard with negative economic implications (5, 6).
Pruritus, the most common symptom in dermatology, may also affect the hands. Pruritus of the hands has been investigated in association with hand eczema (7); however, additional causes, such as other skin conditions (e.g. psoriasis, lichen planus), systemic diseases (e.g. cholestatic disorders), adverse drug reactions, neurological or psychiatric disorders, may also lead to itchy hands (8). Impairment due to hand involvement in patients with chronic pruritus (CP) has never been investigated.
The aim of this prospective study was to investigate the clinical profile of patients affected by CP, and the involvement of the hands, with special focus on pruritus characteristics and associated sensory symptoms, as well as functional impairment and decrease in quality of life. In addition, the study analysed disparities in clinical features and disease-related burden according to the localization of pruritus on the hands and concomitant presence of pain.
Subjects
Consecutive patients with CP were recruited at the Center for Chronic Pruritus, Department of Dermatology of the University Hospital Münster, Germany, between October 2011 and February 2013. Inclusion criteria were the presence of pruritus on one or both hands and age ≥ 18 years. The study was approved by the local ethics committee (2007-413-f-S). All procedures were performed according to the principles of the Declaration of Helsinki and later revisions. The study was registered at the German Clinical Trials Register (DRKS00005238).
Study design
Suitable patients were informed about the study and gave their written informed consent. Following verification of the inclusion criteria, a board-certified dermatologist took the medical history and performed a thorough physical and dermatological examination. Study participants were then asked to complete questionnaires related to clinical characteristics, functional impairment and disease-related burden.
Clinical assessment
Demographic data, including age and sex, were recorded for each patient. Following the recommendations of the International Forum for the Study of Itch (IFSI), patients were categorized according to their skin status (IFSI I: CP on lesional inflamed skin; IFSI II: CP on non-lesional skin; IFSI III: CP accompanied by chronic scratch lesions) and to the underlying aetiology of CP (dermatological, systemic, neurological, psychosomatic/psychiatric, multifactorial, or unknown) (9). The likelihood of atopy was assessed using the Erlanger Atopy Score (10).
Questionnaires and scales
Study participants were instructed to complete a questionnaire on hand pruritus, which was developed specifically for this study. First, it was asked whether pruritus was perceived on the hands. If so, further aspects related to pruritus of the hands were assessed, including its topography, duration, intensity (assessed by the numerical rating scale (NRS) 0–10) (11), additional sensory symptoms, emotional response, its impact on the daily routine and on the ability to use the hands. Patients with skin alterations (IFSI group I and III) completed the Dermatological Life Quality Index (DLQI) (range 0–30) (12). The Hospital Anxiety and Depression Scale (HADS) range subscale anxiety 0–21 (13), range subscale depression 0–21) was used to screen for anxiety and depression.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics, v. 26.0 (IBM Corp., Armonk, NY, USA). Data were analysed descriptively. Data are presented as absolute number of observations (percentage) or median [interquartile range; IQR], as appropriate. The Mann–Whitney U test and Kruskal–Wallis test were performed for comparisons between groups. Spearman’s rank correlation test was used for correlation analyses and χ2 test for comparison of frequencies between groups. To analyse differences according to the localization of hand pruritus, patients were divided into 4 groups: (i) patients with pruritus on the palms and back of the hands; (ii) patients with pruritus on the backs of the hands; (iii) patients with pruritus on the palms; (iv) patients with pruritus on the fingers only. No corrections for missing data were performed. Statistical significance was set at p < 0.05.
Subjects
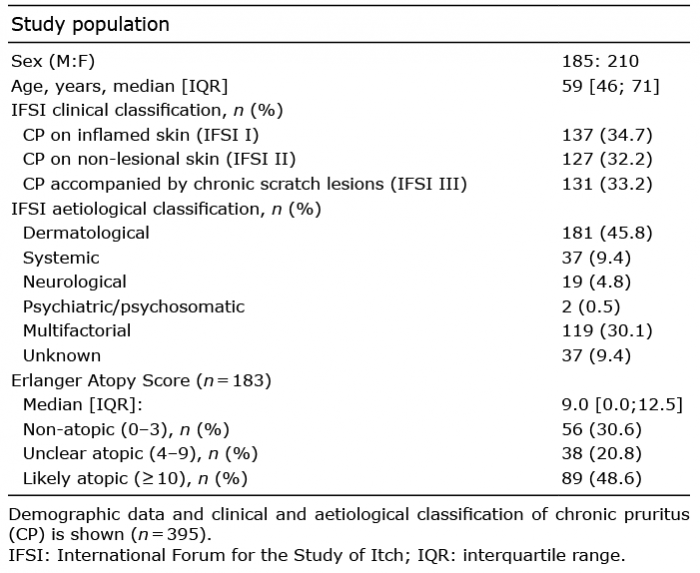
A total of 395 patients were included in this study (median age 59 years [46; 71]; 210 females, 185 males). Taking the CP on the whole body into account, 137 (34.7%) patients showed CP on lesional skin (IFSI I), 127 (32.2%) on non-lesional skin (IFSI II) and 131 (33.2%) presented CP with accompanying chronic scratch lesions (IFSI III), according to the IFSI clinical classification of CP. Almost half of the patients (181/395, 45.8%) had an inflammatory skin condition as the cause for CP, while in a substantial number of cases a multifactorial origin was recorded (119/395, 30.1%; Table I). Of the patients with multifactorial pruritus, 107/119 (89.9%) had a dermatosis in addition to other conditions contributing to the development of CP. Psychological disorders leading to pruritus were recorded in 2 patients as the only cause for CP and in 40 patients with CP of mixed origin.
Table I. Study population
On the hands, the following dermatoses were recorded: atopic eczema (n = 46), dyshidrosis (n = 17), hand eczema not further specified (n = 17), hyperkeratotic rhagadiform eczema (n = 12), nummular eczema (n = 10), prurigo (n = 8), urticaria (n = 5), lichen ruber (n = 2) and psoriasis (n = 1). In addition, 32 patients showed an inflammatory condition that was not further specified.
Almost half of the patients were probably atopic (n = 89/183, 48.6%) according to the Erlanger Atopy Score (Table I). The atopy score correlated positively with the pruritus intensity (r = 0.16, p = 0.04), whereas no differences were observed in atopy score across sex (p = 0.81), IFSI group (p = 0.68) or localization of the pruritus (p = 0.76).
Pruritus characteristics
Most patients reported pruritus on the hands for 1 year or more (203/384, 52.9%), while only a minority had acute pruritus on the hands, i.e. lasting less than 6 weeks (48/384, 12.2%, Table II). The dorsal aspect of the hand and fingers was the most affected area (69.9%, Fig. 1). For further analyses on the impact of the localization of pruritus for disease severity and burden, patients were categorized as having pruritus on the palms and backs of the hands (97/395, 24.6%), or exclusively on the backs of the hand (179/395, 45.3%), the palms (66/395, 16.7%), or the fingers (37/395, 9.4%).
Table II. Pruritus of the hand: clinical characteristics
Fig. 1. Localization of pruritus on the hands (n = 395).
A moderate median pruritus intensity was recorded on the hands (6 [4; 8], n = 388, Table II), which differed according to the localization of the pruritus (p = 0.001). Patients with pruritus affecting both the backs and palms of the hands (7 [6; 8], n = 95) showed higher pruritus intensities compared with patients with pruritus on the backs of the hands (6 [4; 8], n = 178, p < 0.001), palms (6 [3; 8], n = 64, n = 0.004) and fingers only (6 [4; 8], n = 36, p = 0.01, Fig. 2). Pruritus intensity did not differ according to presence of a dermatosis on the hands (p = 0.57), sex (p = 0.61) or IFSI group (p = 0.29).
Fig. 2. Influence of the localization of hand pruritus on symptoms and burden. Pruritus intensity on the numerical rating scale (A; n = 373), presence of pain (B; n = 379), impairment of daily routine (C; n = 368), impairment of the ability to use the hands (D; n = 371), impairment of the quality of life assessed by the Dermatological Life Quality Index (E; n = 238), anxiety score of the Hospital Anxiety and Depression Scale (HADS) (F; n = 348) and depression score of the HADS (G; n = 348) are shown in percentage stratified by the localization of hand pruritus. NRS: numerical rating scale.
Pure pruritus without additional sensations was perceived in 83/395 (21.0%) cases. Most patients reported additional sensory symptoms, such as burning (156/395, 39.5%), painful itch (116/395, 29.4%) and tingling (105/395, 26.6). Of the patients reporting painful sensations and pruritus on the hands concomitantly (n = 181), 104 (57.5%) specified that the pruritus appeared before the sensation of pain, 70 (38.7%) indicated that pruritus and pain occurred simultaneously, whereas 7 (3.9%) answered that they perceived pruritus after the pain. Patients reporting pain in addition to pruritus showed higher pruritus intensity scores (pain: 7 [5; 8], n = 181; no pain: 6 [4; 7], n = 214; p < 0.001, Table III). The concomitant presence of pain did not differ according to presence of a dermatosis on the hands (p = 0.25), sex (p = 0.80), IFSI clinical group (p = 0.10) or pruritus localization on the hands (p = 0.45).
Pruritus of the hands was frequently regarded as persistent (187/395, 47.3%), depressing (156/395, 39.5%) and agonizing (102/395, 25.8%, Table II).
Table III. Influence of pain
Burden
Most patients indicated a moderate to severe impairment of their regular daily routine due to their hand pruritus (249/383, 65.0%, Fig. 3). As for the ability to use the hands, moderate to severe impairment due to the pruritus was recorded in 155/386 of cases (40.2%), while most patients revealed no or only slight impairment (231/386, 59.8%, Fig. 3). The localization of the pruritus affected both the regular daily routine (p < 0.001) and the inability to use the hands (p = 0.001). Patients with pruritus affecting both the back and palm of the hands showed higher impairment of the daily routine compared with patients with pruritus on the back of the hand (p < 0.001), palms (p = 0.02) and fingers only (p = 0.001). As for the ability to use the hands, patients with pruritus on both the palms and back of the hand or only on the palms reported higher impairment compared with patients with pruritus on the back of the hand (p = 0.001) and at the fingers only (p < 0.05, Fig. 2). Patients reporting pain showed higher impairment of the regular daily routine and of the ability to use the hands compared with those without pain (p < 0.001, Table III). There were no sex differences with regard to the impairment of daily routine or of the ability to use the hands (p > 0.1).
Fig. 3. Impairment in daily routine and ability to use the hands due to pruritus.
DLQI was assessed in patients with a dermatosis (IFSI I) or presenting with chronic scratch lesions (IFSI III). Overall, moderate median DLQI scores were recorded (10 [5; 15], n = 250), while 113/250 (45.2%) showed a relevant impairment of the quality of life (DLQI score ≥ 11). The DLQI score correlated significantly with the impairment of the daily routine (r = 0.55, p < 0.001) and with the inability to use the hands (r = 0.47, p < 0.001). DLQI scores differed according to the affected areas of the hand (p = 0.02). Patients with pruritus on both the palms and backs of the hands had higher DLQI scores than patients with pruritus on the backs of the hand (p = 0.02) and fingers only (p = 0.003, Fig. 2). Patients reporting pain showed higher DLQI scores (p = 0.008, Table III), while no sex differences were recorded (p = 0.22).
Using the HADS scale, patients showed low anxiety (7 [4; 11], n = 363) and depression scores (6 [3; 9], n = 363). Pathological scores (≥ 11) were recorded in 26.2% of cases for anxiety and 18.5% for depression. Women showed higher anxiety scores (females: 8 [5; 12], n = 191; males: 7 [4; 10], n = 172; p = 0.03), while no difference was observed for depression scores (p = 0.45). Patients with pruritus on both the palms and backs of the hands showed higher anxiety and depressions cores compared with patients with pruritus on any of the other locations (p < 0.05, Fig. 2). Patients reporting pain in addition to pruritus had higher anxiety (p = 0.005) and depression scores (p = 0.01, Table III).
This prospective study analysed a large cohort of patients with CP and investigated the characteristics of the symptom on the hands. The aim was to establish the clinical profile of this condition, as well as disease-related functional impairment and decrease in quality of life of affected patients.
A homogenous profile was observed regarding the characteristics of pruritus on the hands. In most cases, pruritus on the hands was of moderate to very severe intensity, as reported by 91.2% of patients. Remarkably, almost 1 in 6 patients had very severe pruritus (16%). In addition, most patients perceived other sensory symptoms (79%), such as burning pain or tingling. A long duration of pruritus was seen in the majority of patients, with 71.4% of patients having pruritus for more than 6 months and 52.9% longer than 1 year. Interestingly, this homogenous profile of pruritus features was recorded, even though patients showed a high variance in skin status, aetiological background and atopic disposition (Table I). Common neuronal sensitization mechanisms and the development of an itch-scratch cycle may contribute to similar presentation of pruritus despite heterogeneous underlying clinical features (14).
Pruritus of the hands leads to a high disease-related burden. A substantial proportion of patients were moderately to severely impaired in the use of their hands (40.2%), in the daily activities (65.0%) and in their quality of life (45.2%). The quality of life is especially diminished when the ability to use the hands and the performance of the daily routine is affected owing to the pruritus, as indicated by correlations of moderate strength between these variables and the DLQI score.
The localization of the pruritus on the hands plays an important role in the severity and burden of the disease. In general, patients experiencing pruritus on both the palms and back of the hands experience more severe pruritus, show higher anxiety and depression levels and are more affected in their daily routine. DLQI scores were higher in patients with pruritus on both the palms and back of the hand; however, no causative relationship can be inferred, since the DLQI refers to the impact on quality of life of skin lesions at the whole body, and not specifically on the hands. No disparities were observed between patients with CP exclusively at the back of the hand compared with those with pruritus on the palms only. In contrast, in chronic hand eczema, affliction of the back of the hand was associated with more severe disease and higher impairment in quality of life (15). Different conditions (pruritus vs chronic hand eczema), methodology and sample size may account for the discrepancies across studies. Notably, in the current study, palmar localization of pruritus, alone or in combination with pruritus on the back of the hand, was associated with a higher impairment of the ability to use the hands. Of note, palmar localization of eczema was linked to a more refractory course of disease in chronic hand eczema (16).
One striking point from our analyses is that patients reporting pain in the hands, in addition to pruritus, experience more severe disease. This subgroup of patients experience higher pruritus intensity, is more impaired in daily activities and in the ability to use the hands, and shows higher anxiety and depression scores. Presence of pain on the hands is of particular importance, since painful sensations are perceived more intensely in proximal body parts, whereas pruritus is felt more strongly distally (17). Physicians should thus enquire of patients presenting with pruritic hands whether they also experience pain.
A limitation of this study is that it only included patients presenting at a dermatological clinic specialized in itch. Analysis of patients with hand pruritus presenting at other clinical settings, such as general practitioners and dermatological offices, would be interesting in order to achieve a more comprehensive picture of this patient population. In addition, there was an imbalance of diagnoses in the current patient cohort, with the majority of patients with a hand dermatosis having atopic eczema, while only a minority experienced, for example, hand eczema.
Taken together, pruritus located on the hands is of particular importance, due to the functional relevance of the hands in everyday activities. In general, these patients experience moderate to severe pruritus with substantial functional impairment and disease-related burden. Disease severity is particularly high when both the palms and backs of the hands are affected and when pain is present simultaneously.
This study was supported by a grant from the German Research Foundation (DFG) to SSt (STA1159/4-1) and a grant from the European Academy of Dermatology and Venereology to MPP (EADV 2016-012).
Conflicts of interest: TN and VR declare no conflicts of interest. CZ has received speaker honoraria/travel fees from Beiersdorf and Dermasence. SSt is an investigator for Dermasence, Kiniksa, Galderma, Menlo Therapeutics, Novartis, Sanofi, Trevi Therapeutics and Vanda Pharmaceuticals, and is a consultant, speaker and/or member of the advisory board for Abbvie, Almirall, Beiersdorf, Bellus Health, Benevolent, Bionorica, Cara, Clexio, Escient, Galderma, Grünenthal, Kiniksa, Leo, Lilly, Menlo, Pfizer, Sanofi, Trevi, P.G. Unna Academy, Vifor. MPP is an investigator for Trevi Therapeutics; is a consultant for Galderma; and has received speaker honoraria/travel fees from Galderma, Menlo Therapeutics, Novartis, and Trevi Therapeutics.


 Click to show fullsize
Click to show fullsize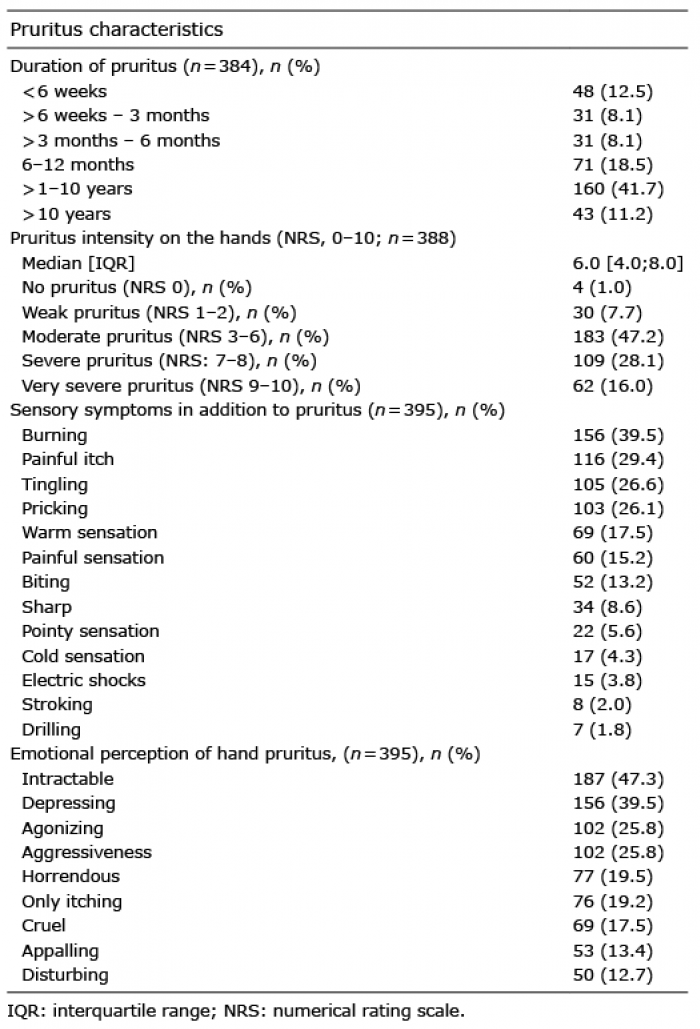 Click to show fullsize
Click to show fullsize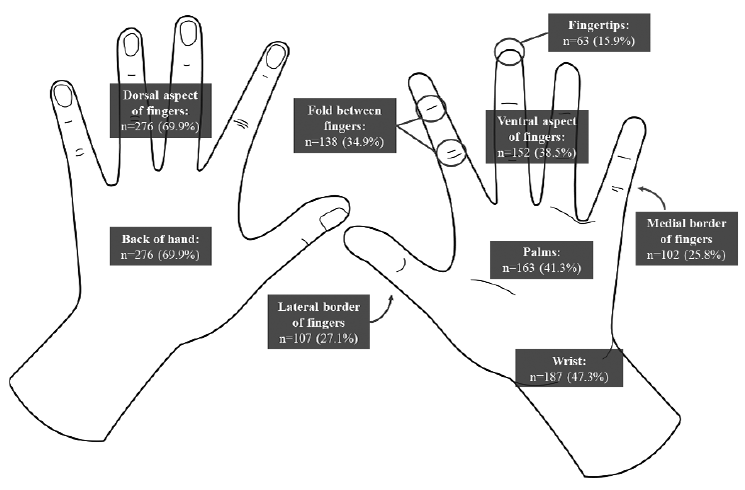 Click to show fullsize
Click to show fullsize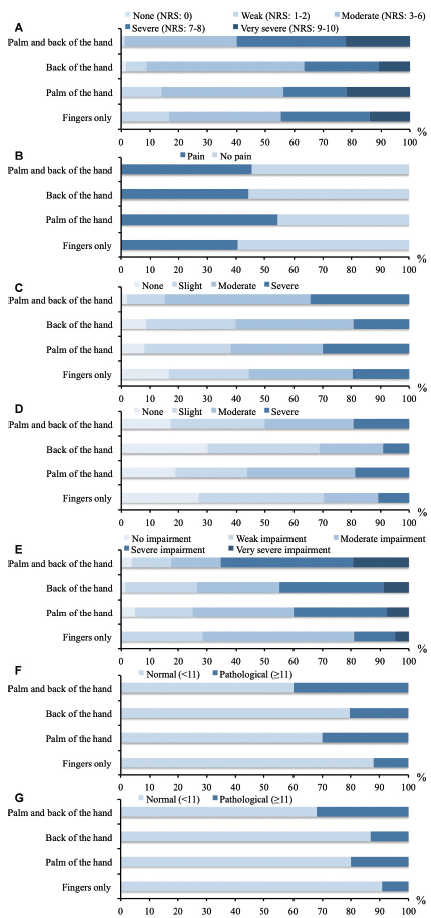 Click to show fullsize
Click to show fullsize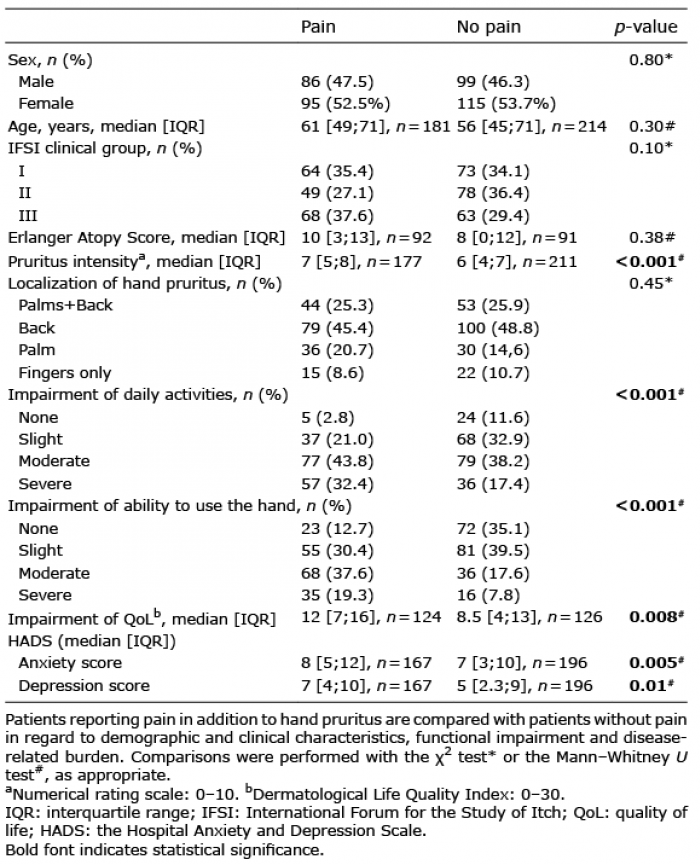 Click to show fullsize
Click to show fullsize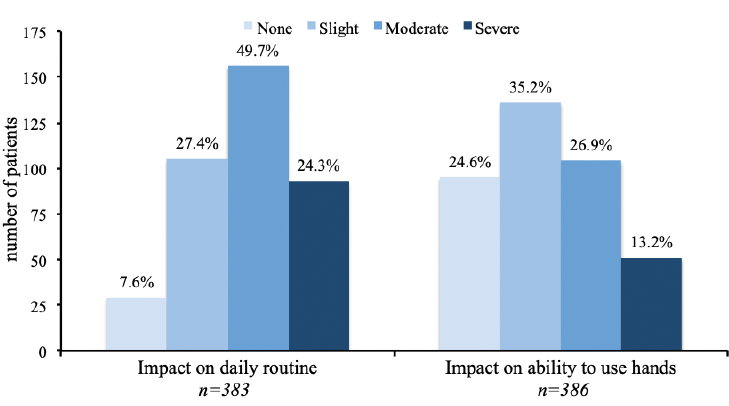 Click to show fullsize
Click to show fullsize