


1Department of Dermatology and 2Department of Rheumatology and Clinical Immunology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, China
Persistent eruption occurs in a subset of patients with adult-onset Still’s disease. In our experience, a considerable proportion of these patients present with peripheral eosinophilia. The aims of this study were to summarize the clinical and histological features of patients with adult-onset Still’s disease with persistent eruption in the current study cohort, and to assess the association between peripheral eosinophil levels and disease characteristics. A total of 21 patients with adult-onset Still’s disease with persistent eruption were included in this retrospective study. Koebner signs, an important diagnostic clue, were found in 85.7% of patients. The proportion of patients presenting with eosinophilia within the disease course was 57.1%. Skin histology revealed infiltration of eosinophils in 90.5% of patients. Peripheral eosinophil levels were positively associated with involved body surface area. Patients with normal peripheral eosinophil counts were more likely to achieve complete remission than those with abnormal peripheral eosinophil counts. Eosinophils may be involved in the pathogenesis of skin eruption. Abnormal peripheral eosinophil counts in these patients may indicate a more refractory disease course.
Key words: persistent eruption; adult-onset Still’s disease; eosinophilia; body surface area; clinical characteristics.
Accepted Sep 8, 2021; Epub ahead of print Sep 13, 2021
Acta Derm Venereol 2021; 101: adv00564.
doi: 10.2340/00015555-3927
Corr: Dong-Lai Ma, Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing 100730, China. E-mail: mdonglai@sohu.com
Adult-onset Still’s disease is an autoimmune disease with multi-organ involvement. Some patients with adult-onset Still’s disease present with a specific, persistent skin rash. This study examined 21 patients with adult-onset Still’s disease with persistent skin rash and found that the rash took a linear form in more than 80% of patients; therefore the presence of a linear rash has diagnostic value. Moreover, the blood eosinophil level correlated positively with involved body surface area. A high eosinophil level in adult-onset Still’s disease may indicate a disease course that is less responsive to treatment.
Adult-onset Still’s disease (AOSD) is a systemic inflammatory disorder characterized clinically by pharyngodynia, high spiking fever, polyarthralgia, evanescent skin eruption, lymphadenopathy, and hepatosplenomegaly (1). Laboratory examinations reveal leukocytosis with neutrophilia, liver dysfunction, elevated serum ferritin and erythrocyte sedimentation rate (2, 3). The classic evanescent skin eruption presents as salmon-pink, non-pruritic, macules or maculopapular erythema in parallel with the onset of increasing fever, and resolves in accordance with the reduction in fever (4). The presentation of evanescent eruption has long been accepted as a major diagnostic finding.
Persistent eruption has been reported in patients with active AOSD, with an incidence of 14.5–78% (5, 6). AOSD with persistent eruption (PE-AOSD) has been reported to be associated with a poorer outcome and the requirement for more potent immunosuppressive therapy to control the disease (7). Although skin rash usually presents in the early stage of disease with a distinct histological presentation (6), PE-AOSD is commonly misdiagnosed due to polymorphisms of the skin eruption. The authors have noticed that peripheral eosinophilia occurs in some patients with PE-AOSD. Therefore, the aims of the current study were: to perform a detailed clinicopathological evaluation and analysis to further understand PE-AOSD and; to determine the relationship between eosinophilia and clinical characteristics in patients with PE-AOSD.
This retrospective study was approved by the ethics committee of the authors’ institutions (Peking Union Medical College Hospital: ethics number K-S1532) in accordance with the Declaration of Helsinki. All clinical data were obtained after the patients provided informed consent.
Patients
All patients diagnosed with PE-AOSD from January 2015 to January 2020 in our hospital were included. Their first visit to hospital was at the Department of General Internal Medicine, Dermatology, Infectious Disease, Emergency, and Rheumatology. All patients met Yamaguchi’s criteria (8) for AOSD and presented with persistent skin eruption. Relevant laboratory tests, imaging studies, and bone marrow and lymph node biopsies were conducted to exclude infection, malignancies, and other rheumatological diseases, when indicated. The clinical diagnosis was confirmed by 2 senior dermatologists and 1 rheumatologist. All 21 patients underwent skin biopsies. Clinical images of all visible skin lesions were captured before skin biopsy.
Assessments
Detailed documentary clinical histories and all available clinical images were reviewed and summarized, including clinical presentations, relevant laboratory test results, percentage of involved body surface area (BSA), initial diagnosis, therapeutic agents, complications, time interval between disease onset and the appearance of skin eruption, time interval between primary treatment and first time of achieving complete remission.
The location and morphology of skin eruptions were described by 2 dermatologists. The Koebner phenomenon was considered positive when 3 or more linear skin lesions were observed, including linear erythematous or brownish urticarial lesions, linear lesions formed by continuously arranged papules, and linear erythematous or hyperpigmented scratches. The percentage of affected BSA was evaluated by 2 dermatologists separately, based on clinical images. Mean BSA scores were used for the final analysis. Pathology slides were reviewed and described by 2 dermatopathology specialists. Disease complications included serositis, co-infections, reactive haemophagocytic lymphohistiocytosis, coagulation disorders, and cardiopulmonary abnormalities. Complete remission was defined when clinical symptoms completely resolved and laboratory test values had all returned to normal.
Statistical analysis
Data are expressed as mean (standard deviation; SD), number (percentage), or median (interquartile range; IQR). SAS 9.4 (SAS Institute Inc., Cary, NC, USA) software was used for all statistical analysis. Data were analysed by Spearman’s correlation, univariate Cox’s proportional hazard regression, multivariate Cox’s proportional hazard regression, Student’s t-test, Kruskal–Wallis test, and variance analysis, where appropriate. Survival curves were calculated using the Kaplan–Meier method based on the length of time between primary treatment and final follow-up or complete remission. The log-rank test was used to assess statistical differences between curves. Hazard ratio (HR) and 95% confidence interval (95% CI) were calculated by univariate and multivariate analyses. A p-value < 0.05 was considered statistically significant.
Patients’ characteristics
Twenty-one patients (17 females, 4 males) with a mean age of 45.4 ± 14.8 years (age range 26–73 years) were included in the study. Median (IQR) follow-up duration was 87.5 days (36.5, 159). Yamaguchi criteria presented in the following proportions of patients: high fever 100%; polyarthralgia/arthritis 81.0%; evanescent eruption 28.6%; leukocytosis with neutrophilia 76.2%; hepatosplenomegaly 57.1%; lymphadenopathy 100%; liver dysfunction 100%, sore throat 61.9%, and negative antinuclear antibody (ANA) and negative rheumatoid factor (RF) 95.2%.
Among all patients with abnormal liver function, the most common elevated liver enzyme was lactate dehydrogenase (LDH, 21/21, 100%), followed by aspartate transaminase (15/21, 71.4%), γ-glutamyl transpeptadase (10/21, 47.6%), alkaline phosphatase (10/21, 47.6%), and alanine transaminase (6/21, 28.6%). All patients had remarkably elevated ferritin levels, ranging from 362 to 25,461 ng/ml.
Fifteen (71.4%) patients received moderate to high doses of corticosteroids isolated or combined with immunosuppressant agents. The mean dosage of prednisone equivalents was 59.3 ± 30.1 mg/day (range 30–120 mg/day). The immunosuppressive drugs were methotrexate (6 patients), tacrolimus (1 patient), cyclophosphamide (1 patient), and cyclosporine A (1 patient). Three cases were well controlled by non-steroidal anti-inflammatory drugs (NSAIDs), and 2 cases by disease-modifying antirheumatic drugs (DMARDs). One case had spontaneous remission without any treatment.
Notably, 12 (57.1%) patients presented with eosinophilia within the disease course with an eosinophil count range from 0.58 to 3.7×109/l (normal range 0.02–0.5×109/l). Eight (38.1%) patients showed elevated eosinophil counts at the time of admission, with a range from 0.66 to 2.3×109/l.
Skin eruption description
All 21 patients presented with persistent skin eruption. Twenty (95.2%) patients reported mild to severe pruritus, and 6 (28.6%) patients had a typical evanescent rash during the disease course. Twenty of the 21 patients had a documented onset time of skin eruption. Skin eruption occurred within the first month of the disease course in 19 (95%) patients, 12 (60%) presented with skin eruption as the initial symptom, and in 16 (80%) skin eruption occurred within the first week. Only 1 (5%) patient developed skin eruption on the 11th month of her disease course.
Skin eruption can be localized, scattered, or widely distributed, with a median involved BSA of 10% (4, 22). Upper chest (15, 71.4%), upper limbs (12, 57.1%), upper back (12, 57.1%), waist (10, 47.6%), abdomen (8, 38.1%), neck (7, 33.3%), lower extremities (6, 28.6%), bottom (5, 23.8%), and face (4, 19.1%), in descending order, were commonly affected.
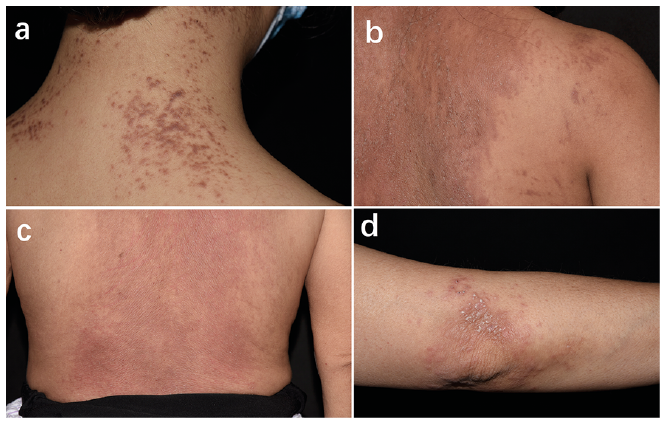
The morphology of skin eruptions was pleomorphic. Skin manifestations included plaques (13, 61.9%), keratotic papules with scales (8, 38.1%), flat-top papules (6, 28.6%), and erythematous or brown patches (4, 19%) (Fig. 1). Various skin lesions can occur in the same patient. The Koebner phenomenon may be prominent or subtle, but occurred in 85.7% (18/21) of patients (Fig. 2).
Fig. 1. Polymorphic cutaneous presentations of persistent eruption adult-onset Still’s disease. (a) Uniform, flat-top brownish papules on the neck. (b) Lichenoid dusty-red and brownish plaques on the back. (c) Diffuse erythema on the lower back. (d) Erythematous patch with keratotic papules on the elbow.
Fig. 2. Different presentations of Koebner signs in persistent eruption adult-onset Still’s disease. (a) Multiple linear erythema on the back. (b) Red, keratotic papules with linear configuration. (c) Extensive dusty-red patches and plaques with prominent linear scratches. (d) Subtle brown linear scratches on the back. (e) Dusty-red flagellate erythema on the waist and abdomen.
Detailed clinical data for each patient are summarized in Table I.
Table I. Detailed data for enrolled patients
Histological findings regarding eosinophilia
Prominent dyskeratosis was revealed in the upper layers of the epidermis (upper and middle stratum spinosum, stratum granulosum and stratum corneum) and sparse superficial dermal infiltration, which could be perivascular or interstitial and mainly consisted of histocytes, lymphocytes, eosinophils and neutrophils (Figs 3 and 4).
Perivascular and interstitial eosinophils were observed in 19 (90.5%) patients. All patients with eosinophilia showed eosinophil infiltration on skin slides; however, eosinophils were absent on skin slides in only 2 of 9 patients without peripheral eosinophilia.
Fig. 3. Characteristic histological pattern of persistent eruption in adult-onset Still’s disease. (a) Hyperkeratosis, multiple dyskeratotic keratinocytes scattered in the stratum corneum and stratum spinosum, sparse perivascular infiltration. (b) Dermal infiltration composed of lymphocytes, neutrophils and eosinophils. (c) Perivascular infiltration composed of lymphocytes, neutrophils (blue arrows), and eosinophils (black arrows). (d) Focal basal cell vacuolation (black arrow). (Haematoxylin and eosin stain; original magnifications: a, ×10; b, ×20; c, ×40; d, ×40).
Fig. 4. Diverse forms of dyskeratosis in the upper epidermis. (a) Mounds of dyskeratotic keratinocytes in the stratum corneum. (b) Diffuse dyskeratotic keratinocytes in cornified layers and upper stratum spinosum. (c) Subcorneal, “pustular-like” cluster of dyskeratosis. (d) Scattered dyskeratotic keratinocytes in the stratum corneum. (Haematoxylin and eosin stain; original magnifications: a, b, c, d ×40).
Association between peripheral eosinophil levels and clinical characteristics
To investigate the relationship between absolute peripheral eosinophil levels and the involved BSA of PE-AOSD, a correlation analysis was performed. Peripheral eosinophil counts were observed to correlate positively with BSA involvement (r = 0.56, p = 0.009; Fig. 5). Correspondingly, peripheral eosinophil counts were significantly higher in patients with BSA involvement ≥ 10 (0.83 ± 0.68 vs 0.26 ± 0.21×109/l, p = 0.022; Fig. 6).
Fig. 5. Peripheral eosinophil counts correlated positively with involved body surface area (BSA). Spearman’s correlation, p = 0.009.
Fig. 6. Peripheral eosinophil counts were significantly higher in patients with body surface area (BSA) involvement ≥ 10%. Student’s t-test, p = 0.022.
Time to complete remission was compared by Kaplan–Meier analysis of all 20 patients with detailed documentation regarding disease remission. Patients with normal peripheral eosinophil counts ≤ 0.5×109/l on admission were more likely to achieve complete remission than those with peripheral eosinophil counts > 0.5×109/l (p = 0.029; Fig. 7a). However, there was no significant difference between patients with BSA involvement ≥ 10% and those with BSA involvement < 10% (p = 0.467; Fig. 7b). In univariate Cox proportional hazard regression, a significantly higher likelihood of non-complete remission was observed in patients with peripheral eosinophil counts > 0.5×109/l (HR 4.23; 95% CI 1.04–17.27; p = 0.044) relative to those with normal peripheral eosinophil counts. In multivariate Cox proportional hazard regression, abnormal peripheral eosinophil group still revealed a significant higher likelihood of non-complete remission (HR 7.75 [95% CI 1.25–48.06], p = 0.028) relative to normal peripheral eosinophil counts group (Table II). No difference was observed in patients with BSA involvement ≥ 10% vs those with BSA involvement < 10% (HR 0.65; 95% CI 0.20–2.15; p = 0.483).
Fig. 7. Kaplan–Meier estimate of complete remission curve. (a) Statistical difference was noted between eosinophil count > 0.5×109/l (n = 8) group and eosinophil count ≤0.5×109/l (n = 12) group. (b) No significant difference was noted between body surface area (BSA) ≥ 10% (n = 11) group and BSA < 10% (n = 9) group.
Table II. Multivariate Cox proportional hazard regression (HR) including age, eosinophil count and body surface area (BSA)
Association between peripheral eosinophil levels and various treatments
Treatment methods were divided into 3 groups: (i) spontaneous remission or with NSAIDs/DMARDs only; (ii) corticosteroids only; (iii) corticosteroids in combination with immunosuppressants. A Kruskal–Wallis test to analyse the eosinophil counts among groups did not reveal any statistical difference (F=0.12, p =0.890). Variance analysis was conducted to analyse the involved BSA among different treatment groups. No significant difference was revealed (F = 0.56, p = 0.581).
Complications
Three patients developed reactive haemophagocytic lymphohistiocytosis, 2 developed pericardial effusion, 2 had cytomegalovirus infection, 1 developed pleural effusion, 1 revealed pulmonary hypertension, 1 developed implacable hypoxemia, and 1 died 3 months after diagnosis due to Pneumocystis carinii pneumonia infection and septic shock. No comorbidities with peripheral eosinophilia, such as asthma or allergic rhinitis, were reported. No accompanying malignancy was reported during the disease course.
The difference in admission peripheral eosinophil count was not statistically significant between patients with or without complications (0.70 ± 0.73 vs 0.42 ± 0.39×109/l; p = 0.92).
AOSD is a systemic inflammatory disorder with multi-organ involvement characterized by spiking fever, usually exceeding 39°C, evanescent cutaneous eruption, arthralgia or arthritis, leukocytosis with neutrophilia, lymphadenopathy, hepatosplenomegaly, and liver dysfunction. Seventy- five percent of AOSD onset occurs between 16 and 35 years of age, and women seem to be affected more often than men (9). Yamaguchi’s criteria are most commonly used in clinical practice, with a sensitivity of 96.2% and specificity of 92.1% (8). The classic skin rash occurs in up to 87% of patients with AOSD (10). Histological findings of classic skin lesions show normal epidermis, with mixed mild perivascular inflammation of the superficial dermis composed of lymphocytes and neutrophils (4).
Persistent cutaneous lesions in AOSD were first described by Kaur et al. in 1994 (11). To date, approximately 116 cases of PE-AOSD have been reported. Linear pigmentation, flat-topped papules and plaques, and urticarial lesions are frequently reported among atypical skin lesions of AOSD (6, 11, 12). Less common manifestations include angioedema, acne-like lesions, pustules on hands and feet, and persistent generalized erythema (13–15). The histopathology of persistent eruption was characterized by dyskeratotic keratinocytes, singly or in clusters, in the upper half of the epidermis, and a neutrophil-containing infiltrate in the upper dermis (6, 16). Eosinophils were considered to be a less common finding in previous research, occurring in 15.4% (2/13) to 38.5% (10/26) of patients (6, 16, 17).
In the current study, the morphology and location of persistent eruption were similar to those reported in the literature. The most common presentation was lichenoid plaque, followed by keratotic papules, flat-top papules, and erythematous patches. Acne-like lesions and pustules on the hands and feet were not encountered in our patients. In 2001, Suzuki et al. (5) reported scratches and linear lesions in 60% (11/18) of patients with PE-AOSD. In the current study, 85.7% of patients presented with a positive Koebner phenomenon, obvious or subtle, which manifested as either linear erythema, papules, scratches, or hyperpigmentation. The upper back, lumbosacral area, and bottom were frequently involved, while the difficult-to-reach midback areas were usually spared, leading to a classic “butterfly” sign, indicating that the linear lesion came from vigorous scratching. The bizarre appearance of linear skin eruption is highly distinctive and can serve as an important diagnostic clue. Similar flagellate lesions may occur in dermatomyositis, flagellate erythema caused by bleomycin, and shiitake dermatitis (18). The pertinent history, systemic syndromes, and skin histological presentation can provide sufficient evidence in differential diagnosis.
In the current study, histological examinations of all 21 patients with PE-AOSD showed remarkable dyskeratotic keratinocytes in the upper and mid epidermis. Eosinophil infiltration was encountered in 90.5% of patients. Moreover, peripheral eosinophilia was noticed in 57.1% of patients with PE-AOSD in the current study. Peripheral eosinophil counts correlated positively with the involved BSA, and patients with abnormal eosinophil counts showed a more refractory disease course, which provides an intuitive method for disease evaluation. However, the exact pathogenesis of this phenomenon is unknown. Eosinophil derives from bone marrow hematopoietic stem cells and is an immunological modulation and effector cell involved in inflammatory reactions by releasing cytokines and toxic proteins (19). Eosinophilia occurs most commonly in allergic or parasitic diseases. In other situations, such as granuloma faciale, Ofuji disease, eosinophilic granulomatosis with polyangiitis, and haematological malignancy, blood and tissue eosinophilia can also be observed (19, 20). Circulating eosinophil counts correlate with the severity of various skin diseases, including bullous pemphigoid, atopic dermatosis, of which the involved BSA is an important parameter for assessment of severity (21, 22). In the current study, the larger BSA involvement and more refractory disease course in patients with PE-AOSD with elevated peripheral eosinophil count probably associated with a more intensive inflammatory reaction caused by immunological effector cells. The role of eosinophils in the pathogenesis of AOSD has rarely been discussed. Macrophage and neutrophil activation are a hallmark of AOSD (23). Interleukin (IL)-18 and IL-1β are key factors in the pathogenesis of AOSD. Meanwhile, elevated IL-18 expression is also noticed in many allergic diseases. The development of urticaria, dermatitis, and eosinophilic disorders has demonstrated correlations with increased IL-18 levels either in the tissue or systemically (24). In a mouse model, IL-18 increases IL-5 levels, which can induce the rapid proliferation of eosinophils (24). IL-1β was also reported to be significantly higher in patients with active asthmatic symptoms and is a potential biomarker for active allergic diseases (25). It is possible that elevated serum and tissue IL-18 and IL-1β in PE-AOSD recruit eosinophils, resulting in persistent, pruritic skin eruption in AOSD. In light of the eosinophil involvement in disease pathogenesis, we assume that anti-IL-5 therapies may theoretically help to treat particular refractory cases with abnormal peripheral eosinophil count, which should be further examined in the experimental study.
PE-AOSD is easily misdiagnosed. Only 9.5% (2/21) of the patients were initially suspected of having Still’s disease in the current study. Incorrect primary diagnosis included dermatomyositis, connective tissue disease, drug eruption, drug rash with eosinophilia and systemic symptoms (DRESS), fever of unknown origin, prurigo pigmentosa, and hyperimmunoglobulin-E syndrome (HIES). The distribution of persistent eruption in AOSD could be highly consistent with dermatomyositis, which may present as erythematous patches or lichenoid plaques with photoaccentuation, keratotic papules on the extensor limbs, and flagellate rashes. Meanwhile, both diseases could have fever, arthralgia and myalgia. Laboratory examination revealed an elevated LDH level in all the PE-AOSD patients in the current study, which also presents common abnormalities in dermatomyositis. However, spiking fever is less common in dermatomyositis. Moreover, the skin histological presentations of these 2 diseases are distinct. Dermatomyositis shows sparse inflammatory infiltrations with dermal mucin deposition. In contrast, prominent dyskeratosis in the epidermis was seen in PE-AOSD. Eosinophil and neutrophil infiltrate are also less common in dermatomyositis (17). As patients with PE-AOSD are commonly treated with antipyretic agents or antibiotics in the early stage, drug eruption, especially DRESS, is easily confused. PE-AOSD and DRESS may both present spiking fever, lymphadenopathy, leukocytosis with neutrophilia, eosinophilia, elevated inflammatory markers, and liver dysfunction. Both may present symmetrical, generalized, erythematous, pruritic skin eruptions. Early or mild PE-AOSD may display only subtle pathological changes, and is difficult to differentiate from DRESS. However, clinically, DRESS usually presents with maculopapular eruption, which rapidly progresses into erythroderma. Facial oedema is distinctive in DRESS (26), while the persistent eruption in AOSD is more localized, with linear lesions caused by the Koebner phenomenon. Polyarthralgia occurred in 81% of patients with PE-AOSD and was not a prominent manifestation in DRESS. Atypical lymphocytosis > 5%, which is a diagnostic criterion for DRESS, is absent in AOSD (26). Histologically, dyskeratotic keratinocytes preferably localize to the superficial epidermis in PE-AOSD, while they can be observed throughout the whole epidermis in drug eruption (7). Focal basal cell vacuolation is more prominent in drug eruption than in PE-AOSD (17). HIES is also a common misdiagnosis. Lichenoid brown papules and plaques mimic skin lesions in HIES, especially in hyperimmunoglobulin-E dermatitis (HIED). However, fever and arthralgia are uncommon in HIES. In HIED, histological examination showed perivascular lymphocytes and eosinophils but lacked dyskeratotic cells in the epidermis. In PE-AOSD and prurigo pigmentosa, the upper chest and interscapular region are commonly affected. The cutaneous lesions could both manifest as dusky-red or brownish papules and plaques, with severe itching. However, persistent eruption in AOSD was accompanied by systemic involvement, while prurigo pigmentosa was more related to diabetes or violent rubbing by nylon textiles. Morphologically, PE-AOSD usually presented with prominent linear lesions, while prurigo pigmentosa showed a reticular distribution. Histologically, they both had dyskeratosis in the epidermis and a dermal infiltration of perivascular and interstitial neutrophils, lymphocytes, and eosinophils. However, in prurigo pigmentosa, neutrophil infiltration into the epidermis and liquefaction of basal cells is highly remarkable (27).
Treatment of AOSD is largely empirical (23). In mild cases, NSAIDs may be enough to achieve long-term disease control, while in refractory cases, a large or even impulse dose of corticosteroid is needed, alone or in combination with immunosuppressants. PE-AOSD was suggested to need more potent immunosuppressive therapy to control the disease (5, 7). The persistent rash was reported to improve only after systemic corticosteroid treatment (16). In the current study, skin eruptions and systemic symptoms were relieved with corticosteroid treatment as well as with NSAIDs, DMARDs, or even spontaneous remission. However, disease with spontaneous remission or disease control with NSAIDs occurs only in patients with normal peripheral eosinophils. In general, the mortality rate and complication rate in the current series were similar to those in previous reports. The mortality rate in AOSD varies in the literature, ranging from 0% to 9.8% (28). In the current study, patients with PE-AOSD had a mortality rate of 4.8% (1/21). Complications in AOSD can be severe or even life-threatening. Reactive haemophagocytic lymphohistiocytosis, a lethal complication in AOSD, with a reported prevalence of 2.8–12% in different retrospective studies (29, 30), presented with an incidence of 14.2% (3/21) in the current series. Pulmonary arterial hypertension (PAH) is a rare AOSD complication that usually occurs in patients who have persistent and severe disease, with a reported incidence of 4.8% (2/41), showing a similar incidence in the current study (31). Other severe complications, including coagulation disorders, fulminant hepatitis, cardiac tamponade, and amyloid A amyloidosis, were not encountered in the current series. Although there was no significant difference between the 2 groups, the number value of mean eosinophil count in patients with PE-AOSD with complications increased by nearly 65.7% compared with those without complications, which may relate to the limited sample size in the current study.
Study limitations
This study has several limitations. The primary limitation is the retrospective design, limiting the ability to determine causality. A prospective study is needed to provide more persuasive evidence regarding causality. Due to the low diagnostic rate of PE-AOSD and the fact that this is a single-centre study, the sample size is limited. A larger cohort may lead to a better understanding of the nature of PE-AOSD. Further research is needed to elucidate the role of eosinophils in the pathogenesis of this disorder.
Conclusion
PE-AOSD has a unique clinical and histological pattern. A comprehensive understanding of the disease may avoid misdiagnosis and inappropriate treatment in clinical practice. In the current study cohort, a high proportion of patients developed skin eruption during the early stage of the disease course. Koebner sign was an important clue leading to diagnosis. Blood and skin eosinophilia was frequently encountered. The peripheral absolute eosinophil count was positively associated with involved BSA. Patients with peripheral eosinophilia may have a more refractory disease course. In this study cohort, patients with PE-AOSD showed a similar mortality and complication rate to patients with classic AOSD, with no accompanying malignancy.
The authors thank all of the patients involved in this study. The patients provided written informed consent to publication of their case details.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize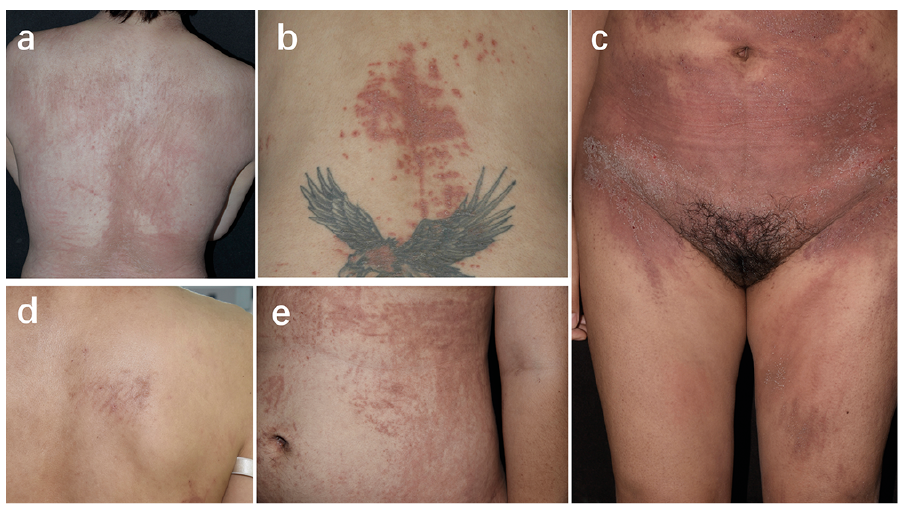 Click to show fullsize
Click to show fullsize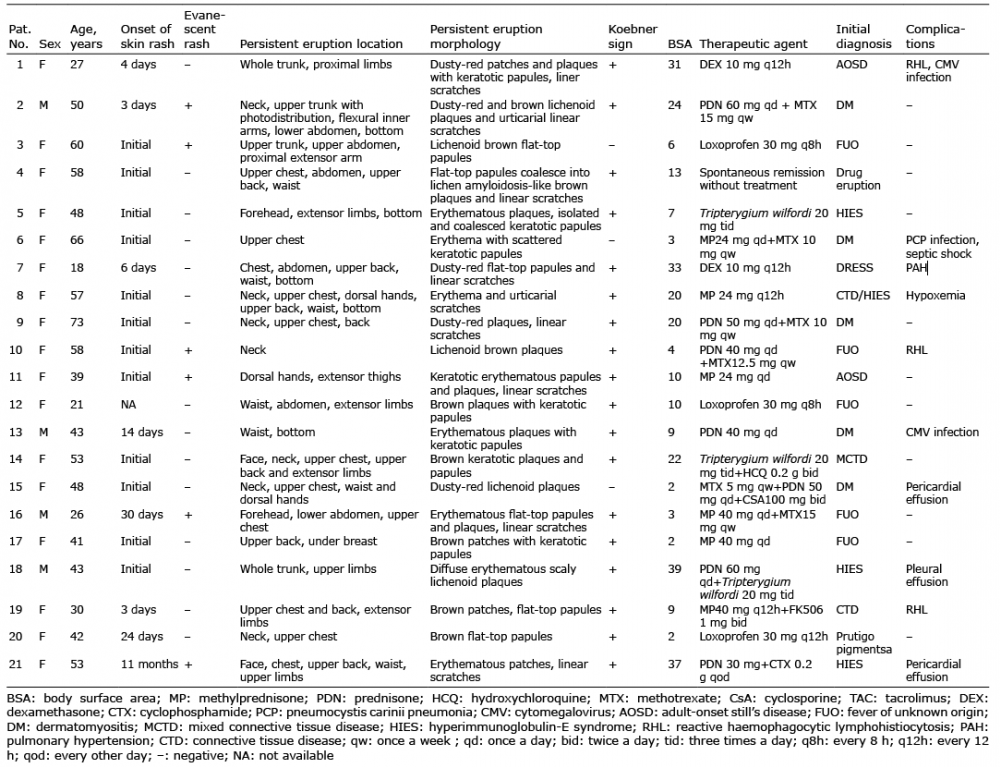 Click to show fullsize
Click to show fullsize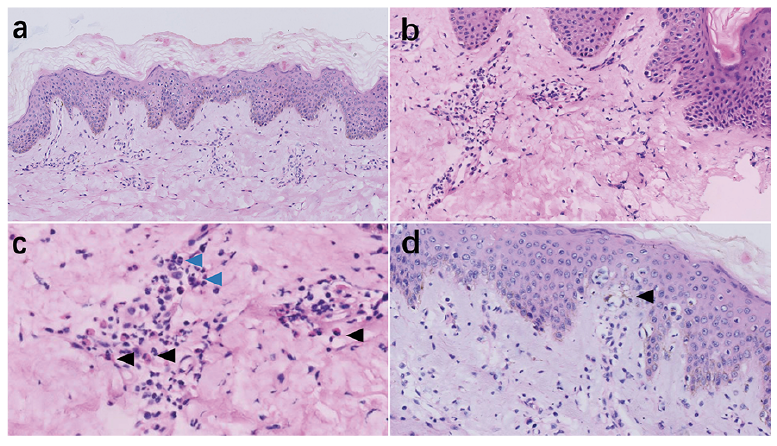 Click to show fullsize
Click to show fullsize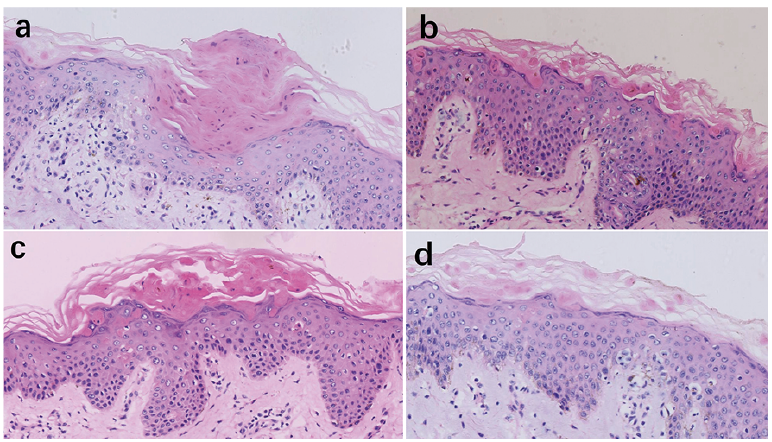 Click to show fullsize
Click to show fullsize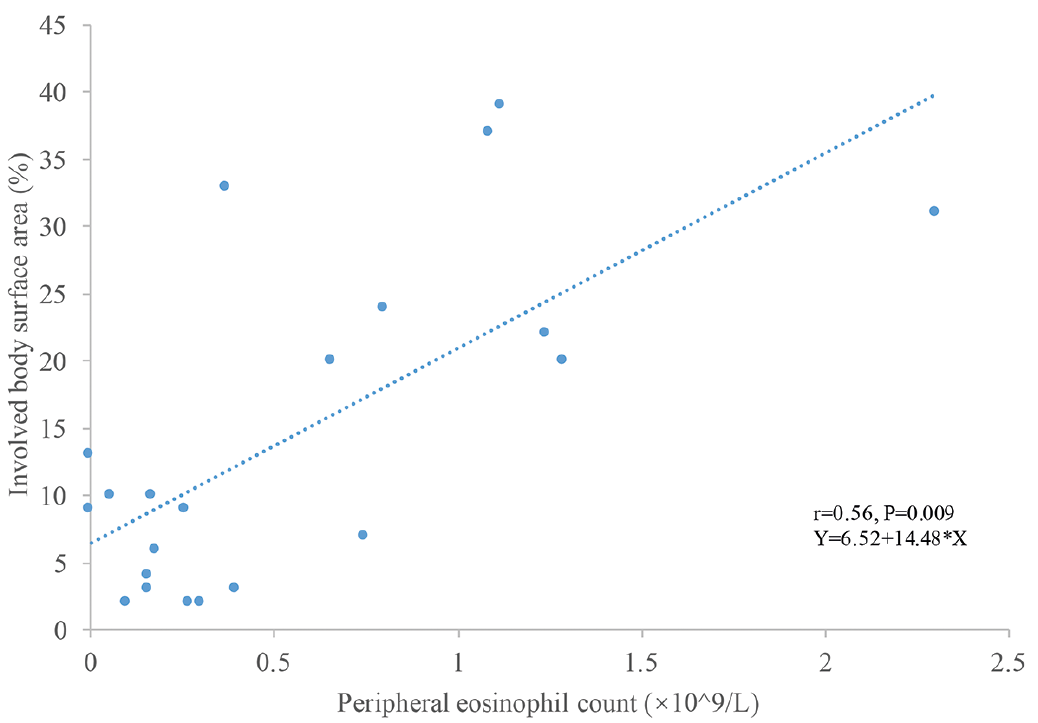 Click to show fullsize
Click to show fullsize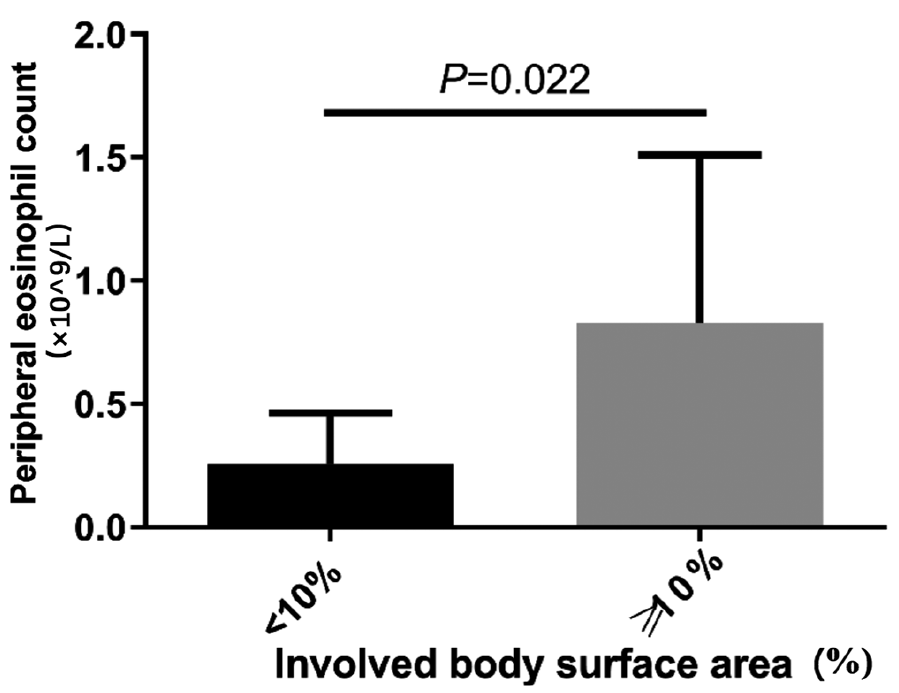 Click to show fullsize
Click to show fullsize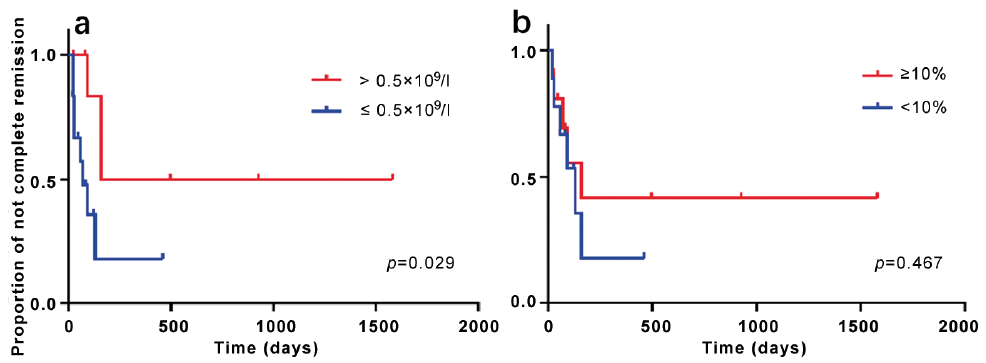 Click to show fullsize
Click to show fullsize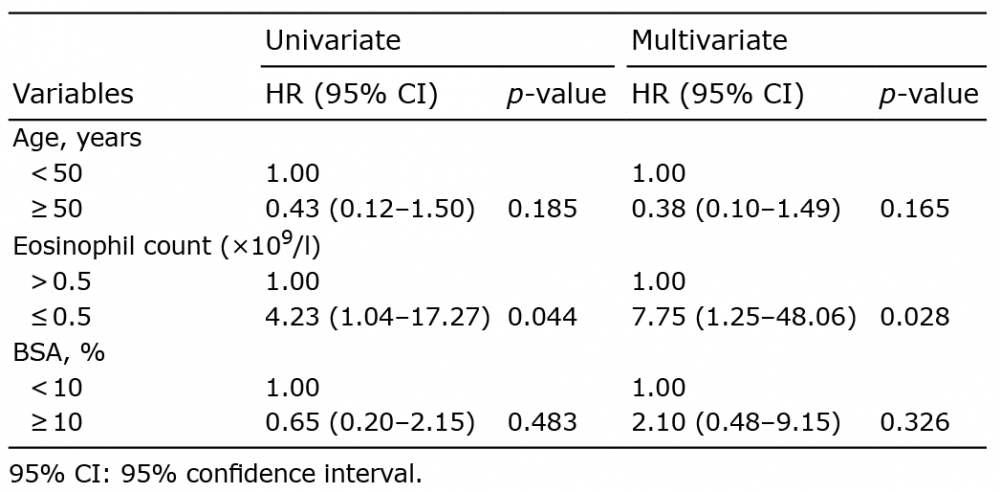 Click to show fullsize
Click to show fullsize