EFFICACY OF A FLEXIBLE ORTHOTIC DEVICE IN PATIENTS WITH OSTEOPOROSIS ON PAIN AND ACTIVITY OF DAILY LIVING
Matthias Fink1, Banu Kalpakcioglu2, Matthias Karst3 and Michael Bernateck3
From the Departments of 1Physical Medicine and Rehabilitation and 3Anaesthesiology and Pain Medicine, Hannover Medical School, Hannover, Germany and 2Haseki Training and Research School, Istanbul, Turkey
OBJECTIVE: To study the efficacy of a flexible orthotic device in patients with osteoporosis.
DESIGN: Open observational study.
Patients: Fifty patients with osteoporosis.
METHODS: An open observational study was performed on 50 patients with osteoporosis in order to investigate the efficacy of a new osteoporosis orthotic device, which is an elastic back support with paravertebral air chamber pads. The outcome parameters were pain, activities of daily living, individual compliance and comfort. The observation period was approximately 2.5 months, and the orthotic device was worn continuously during daytime.
RESULTS: There was a highly significant reduction in pain under exertion from mean 6.1 (SD 1.7) to 4.5 (SD 1.4) (p < 0.00001), pain when driving from 5.2 (SD 2.4) to 3.8 (SD 1.9) (p < 0.00001), and pain at rest from 4.1 (SD 2.4) to 3.1 (SD 1.9) (p < 0.0001). About 50% of the patients judged their ability to perform everyday activities as ‘‘much better’’ or ‘‘better’’. If physiotherapy was interrupted upon onset of orthosis treatment, the results were significantly worse than in patients with continued physiotherapy.
CONCLUSION: This orthotic device could be a useful addition to the medical care of patients with osteoporosis and a complement to drug treatment and physiotherapy with regular exercises, which should be continued.
Key words: orthotic device, osteoporosis treatment, physiotherapy.
J Rehabil Med 2007; 39: 77–80
Correspondence address: M. Fink, Hannover Medical School, Department of PMR, Carl-Neuberg-Str. 1, DE-30625 Hannover, Germany. E-mail: fink.matthias@mh-hannover.de
Submitted March 13, 2006; accepted May 10, 2006.
INTRODUCTION
Osteoporosis is regarded as a systemic disease of the skeletal system and involves a reduction in bone mass and changes in the microstructure of bone tissue, resulting in increases in the brittleness of bones and the risk of fracture. Osteoporosis is clinically important because of osteoporotic fractures that frequently affect the vertebral bodies, femoral neck and distal radius, leading to considerable impairment of health and quality of life. Vertebral body fractures mostly tend to occur in the central kyphotic part of the thoracic spine (Th 7–8) and the thoracolumbar transition (1).
By far the most frequent complaint of patients with osteoporosis is pain upon standing and under physical stress, particularly when bending forward (2). The patients’ activities of daily living are considerably limited, not only due to pain and posture alterations, but often also to the fear of falling. Pain reduction and an increase in individual mobility are important goals in the multidisciplinary treatment of patients with osteoporosis. Many patients refuse analgesics, and physiotherapy, although desirable, is often hampered by the pain patients are suffering from. Rigidly constructed orthotic devices, however, are unsuitable for long-term therapy. The aim of using spinal devices in patients with osteoporosis are: (i) decreasing thoracic and lumbar pain, (ii) compensating weakness of erector spinal muscles, (iii) decreasing kyphosis, (iv) reducing compression forces on vertebrae and decreasing an anterior wedging (3). In long-term use of orthotic devices, the mobility of the patients should not be restricted to prevent atrophy of trunk muscles.
The aim of this clinical study was to investigate the efficacy of a highly flexible orthotic device as an adjuvant therapy in the treatment of patients with osteoporosis. Our hypothesis was that this elastic device could reduce pain and improve quality of life of patients with osteoporosis.
MATERIAL AND METHODS
The efficacy of a new orthotic device (Osteomed, Thaemert Ltd, Germany) was investigated in a prospective uncontrolled clinical trial. The outcome parameters were pain, activities of daily living, and individual compliance.
Patients
The study population included 50 female patients of an outpatient clinic specializing in the treatment of osteoporosis. Patients were recruited according to the in- and exclusion criteria.
Inclusion criteria: DXA T-score < –2.5 measured ≤ 12 months before the study and typical osteoporosis-related back pain syndrome.
Exclusion criteria: other diseases with joint pain, e.g.
• rheumatoid arthritis;
• osteoarthritis of weight-bearing joints.
Patients from the database of the practice were contacted by telephone in alphabetical order. Twenty-two recruited patients could not be included due to the following reasons:
• 3 patients had moved their accommodation in the meantime;
• 4 patients were not interested in participating in the study;
• 11 patients reported exclusion criteria that were not on file upon questioning (3 rheumatoid arthritis, 5 osteoarthritis of the hip and 3 osteoarthritis of the knee)
• 2 patients had suffered a stroke;
• 2 intercurrent deaths.
The study population is described in Table I.
| Table I. Study population data of the 50 female patients | |
| Characteristics | |
| Age, (year), mean (SD); range | 72.6 (7.1); 52–90 |
| Height, (cm), mean (SD); range | 160 (7); 147–172 |
| Weight, (kg), mean (SD); range | 70.4 (11); 49–100 |
| Waist circumference (cm); mean (SD), range | 93 (11); 71–114 |
| BMI, (kg/m2), mean (SD) | 27.6 (3.8) |
| Normal | 30% |
| Slight obesity | 36% |
| Moderate obesity | 32% |
| Marked obesity | 2% |
| Vertebral body fractures: (number of patients in each category) | |
| 0 | 6 |
| 1 | 9 |
| 2 | 28 |
| 3 | 4 |
| > 3 | 3 |
| DXA mean (SD) | –3.01 (0.44) |
| Duration of complaints: (number of patients in each category) | |
| ≤ 1 year | 4 |
| 1–2 years | 4 |
| 3–5 years | 13 |
| 6–10 years | 13 |
| 11–20 years | 7 |
| > 20 years | 9 |
| Pre-treatment: | |
| (a) Operation | 1 |
| (b) Other braces/orthoses | 23 |
| (c) Without pre-treatment | 26 |
| SD: standard deviation, DXA: dual X-ray absorptiometry. | |
All patients were exposed to a mixture of everyday stresses, including lifting and carrying, walking, standing and sitting (domestic and free time). Only one patient was still at work and one patient had been previously operated (tertiary prophylaxis); all other patients had been treated with drugs for the secondary prophylaxis of osteoporosis. All patients were treated with bisphosphonates, calcium, and cholecalciferol. Fourteen patients received non-steroidal anti-inflammatory drugs (NSAIDs) (ibuprofen 800 mg or diclofenac 50 mg) as a demand medication. Average bone density values were –3.01 (SD 0.44) (range –4.25 to –2.48). The number (0, 1, 2, 3, > 3) of vertebral fractures before treatment was nil (n = 6), one (n = 9), two (n = 28), three (n = 4), or over three (n = 3), respectively.
The patients were enrolled within 6 months in the context of normal medical care in a specialized outpatient clinic for osteology. Patients were informed about the study protocol, and consent was obtained before the start of the trial. Patients were then supplied with the osteoporosis orthotic device. Neither additional expenditure nor any monetary benefit arose for the patients. Monitoring and data evaluation were performed by the authors. Data were collected before the start of the observation period and after 10 weeks. There were slight individual differences in the length of the observation period owing to the time of inclusion in the study. The mean duration of observation was 2.5 (SD 0.7) months.
The outcome parameter ‘‘pain’’ was measured with a 11-point numerical rating scale (between 0 = no pain and 10 = unbearable pain), changes in the ‘‘activities of daily living’’ with a 5-point verbal rating scale (much better – better – no change – worse – much worse). Comfort, handling, fit, skin tolerability and feeling of safety and of warmth were rated subjectively on a 6-point numerical rating scale, a range comparable to the grading in the German school system (1 = ”very good’’, 6 = ‘‘unacceptable’’).
Intervention
The Osteomed orthotic device is intended as an orthopaedic adjuvant for the treatment of osteoporosis. Its external appearance resembles a Total Lumbar Spine Orthosis (TLSO), however there are no rigid construction details and it is worn like a body stocking. On the back section of the device air chamber pads are fixed and filled to about 75% of their capacity. The pads are arranged in a symmetrical pattern in the lumbosacral and the thoracic area. There are two paired Velcro tabs in the lateral lumbar region, enabling a tight fit of the lumbosacral pads to the shape of the body. The osteoporosis orthosis is made of elastic material to ensure optimal pressure on the lumbar pads. When the patient moves, the air in the pads is displaced, providing a continuous back massage (Fig. 1). The device has no stabilizing element, and hence exerts no direct bio-mechanical effect. The pain reduction is rather based on a motion-induced stimulation of subcutaneous mechanoceptors (massage-like effect) and an improvement of proprioception due to traction-compression stimuli from the elastic canvas, which should lead to an improved posture of the trunk.
The device is available in different sizes. An orthosis of the individual size was handed over to each study patient during a regular outpatient consultation and was then worn during the day.
Before the Osteomed orthotic device was prescribed, 23 patients used to wear an elastic lumbar corset (Reversa Classic, Thamert Ltd, Germany) for at least 6 months.

Fig. 1. ‘‘Osteomed’’ osteoporosis orthosis (Thaemert Ltd, Germany). The air chamber pads are shown on the outside of the device for better understanding in the left-hand photograph.
Statistics
The data were analysed with the STATISTICA package (StatSoft, Inc., Tulsa, OK, USA) employing the following tests: Spearman’s rank correlation test (correlation between two continuous variables), Wilcoxon test for pair differences (difference in continuous parameters between paired samples), Mann-Whitney U test (difference in continuous parameters between unpaired samples), and χ2-test (difference between frequency distributions of discrete characteristics). The level of significance was consistently set at p < 0.05.
RESULTS
All 50 patients enrolled in the study appeared for the follow-up investigation, and all had worn the orthosis during the daytime for the entire observation period. Treatment effects on the intensity and frequency of pain were measured under the conditions of ‘‘exertion’’, ‘‘car driving’’ and ‘‘at rest’’. At the end of the observation period, a highly significant mean reduction in pain of roughly 25% was found with respect to all three pain qualities (Fig. 2).
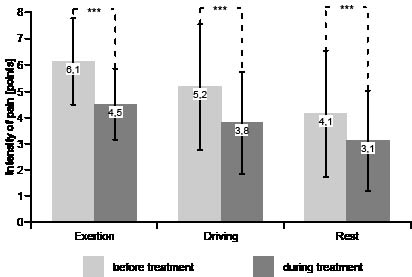
Fig. 2. Intensity of pain (mean and SD) before and during orthosis usage (***p < 0.0001; Wilcoxon-test).
The patients were asked to decide whether their ability to perform everyday activities (as far as sports, car driving, hobbies and domestic work were concerned) was ‘‘much better’’ or ‘‘better’’ then before treatment. This question was answered positively by more than 50% of patients (Fig. 3).
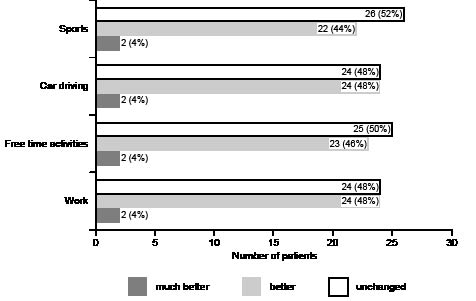
Fig. 3. Everyday activities during orthosis usage (percentage distribution).
There was a trend towards a greater treatment-related improvement in pain under exertion for patients, who had been previously treated with a lumbar spine orthotic device; the corresponding difference for pain when driving a car was statistically significant (p < 0.05; U-test). The subjective parameters, such as wearing comfort, handling, fitting, skin tolerability, feeling of security and feeling of temperature, all got good ratings from the patients and the pre-treated subgroup rated these comfort parameters even better (Table II).
| Table II. Rating of subjective parameters (U-test) | |||||
| No pre-treatment with braces or bandages | Pre-treatment with braces or orthoses | ||||
| n | Mean (SD) | n | Mean (SD) | ||
| Wearing comfort | 27 | 2.00 (0.48) | 23 | 1.48 (0.51) | |
| Handling | 27 | 2.22 (0.64) | 23 | 1.61 (0.66) | |
| Fit | 27 | 2.85 (0.82) | 23 | 2.30 (0.82) | |
| Skin tolerability | 27 | 1.96 (0.44) | 23 | 1.57 (0.51) | |
| Feeling of security | 27 | 1.93 (0.55) | 23 | 1.65 (0.65) | |
| Feeling of temperature | 27 | 2.67 (0.68) | 23 | 2.43 (0.90) | |
Furthermore, possible influences on the regression of symptoms during treatment with the orthotic device were investigated. Pain under exertion showed a significant correlation with the duration of symptoms (p = 0.0062, r = 0.200): the longer the duration, the more markedly the pain under exertion regressed during treatment with the orthosis. The same correlation was found for the improvement in pain when driving a car (p = 0.0011, r = 0.234) and – less, but still significant – at rest (p = 0.0083, r = 0.083).
Bone density and number of fractures showed no significant correlation (p = 0.37 and p = 0.87 (ANOVA), respectively). However, physiotherapy before treatment onset and its continuation during orthosis treatment yielded a substantial benefit (p = 0.019 (ANOVA)): Whereas patients without previous physiotherapy (n = 14) achieved a reduction of only 1.85 points on the pain score, the improvement in patients with previous and continued physiotherapy was 2.28 points (p > 0.05). The worst result was obtained in patients who had discontinued a previous physiotherapy after orthosis prescription, with only 0.83 points improvement; the difference between the two latter groups was statistically significant (p = 0.023).
Side-effects
No side-effects of any kind, such as poor tolerability of the material, were observed or reported by a patient at any time during the observation period.
DISCUSSION
Orthotic devices have repeatedly been recommended as a possible adjuvant in conservative therapy of manifest osteoporosis. The main indication for the use of such devices on the trunk is secondary prevention, that is, to avoid or to treat the acute phase after vertebral body fractures (4–7). Most orthotic devices employed are stable frame constructions or semi-rigid trunk orthoses.
Although recommended, currently available rigid devices have been reported to have substantial disadvantages. In particular, rigid braces are uncomfortable to wear, restrict movement and their unattractive appearance results in low compliance. Moreover, stable orthotic devices should be used only for a limited period of time. Kaplan et al. (8) pointed out that orthotic devices impose a risk of reduction in muscular strength. Their controlled pilot study with a 4-week observation period demonstrated that the strength of the back extensors was reduced to below the initial value in 40% of female patients wearing a stable orthotic device.
The availability of pre-emptive treatment modalities supporting pain restriction and perhaps maintenance of an erect posture without the described disadvantages would be beneficial for many patients with osteoporosis. The kyphotic changes in posture not only accelerate the development of chronic postural back pain, but also impair the function of the back musculature, resulting in increased stiffness and trunk ataxia as well as a lack of stability when standing or walking (9). Lynn et al. (10) have performed a controlled clinical study using a postural graphic method of measurement and were able to demonstrate that the risk of falls was greater for female patients with both osteoporosis and kyphotic malposture compared with patients with osteoporosis without malposture or with healthy controls, respectively.
One substantial point that remained unclear was the effects of this osteoporosis orthotic device on the development of pain during a longer treatment period and the subjective evaluation by the patients of handling and comfort. In the present study, the device was worn for 2.5 months and, during this period, there was a statistically significant and clinically relevant reduction in chronic back pain by approximately 25% in this group of female patients with osteoporosis. The patients also rated the comfort and handling of the orthosis as ‘‘good’’ or ‘‘very good’’. More than half of the patients could perform everyday activities ‘‘better’’ or ‘‘much better’’. Patients suffering for a longer period had better treatment results. The correlation was rather loose, which is to be expected, because the symptom duration is at best a co-factor for the therapy success, but statistically significant, suggesting a somewhat stronger effect of the device in patients with long-lasting disease.
A trend to a better result on pain reduction in patients, who had been previously treated with an orthotic device for low back pain may derive from a pain-reducing effect of the new orthotic device on the thoracic and lumbar region, whereas conventional lumbar braces act only on the lumbar area. The soft construction of the new orthosis in contrast to the lumbar brace from the pre-treatment period also may explain the better rating in this subgroup with respect to the comfort parameters.
As the patients were instructed to wear the orthotic device throughout the day for the whole observation period of 2.5 months, side-effects (e. g. skin intolerance or hygiene problems) should have been noted, if present, but were not reported by any patient. In addition, the follow-up investigations found no signs of skin irritation in possible stress zones (groin or arm-pit). Although, part of the study was performed during summer, warm temperatures did not reduce wearing comfort in any of the patients.
A high percentage of patients with osteoporosis received physiotherapy upon evaluation; thus it seemed worthwhile to examine the possible impact of concurrent physiotherapy on the effect of orthosis treatment. Prior to the present study, 36 of our patients had received physiotherapy twice per week, 18 of whom discontinued this treatment before they began wearing the orthosis. Comparison of these two subgroups clearly showed an advantage of continued physiotherapy; the results in these patients were substantially better than after discontinuation of physiotherapy. Thus, physiotherapy should be complemented rather than replaced by the new orthosis.
Limitations of this study are the open, observational design without a control treatment or an untreated study group on a waiting list. Additionally, inclusion and exclusion criteria should have been considered more rigorous, and a pain diary might have provided further insight on the effectiveness of the new device. Considering these shortfalls, these results have to be regarded as preliminary and should be reassessed in a randomized controlled clinical long-term trial.
In conclusion, the application of the novel orthosis achieved a substantial pain reduction. Furthermore, about half of the patients rated everyday activities as improved. Before this new treatment modality can be generally recommended, it would be desirable to perform controlled studies and to investigate possible effects on the strength and coordination of the trunk musculature.
Acknowledgement
We thank Dr. Michael Fischer, Department for Physical Medicine and Rehabilitation, Hannover Medical School, for translating the manuscript into English language and also to have some essential comments on the presentation of the study data.
REFERENCES
1. Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ. Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res 1992; 7: 221–227.
2. Leidig G, Minne HW, Sauer P, Wuster C, Wuster J, Lojen M, et al. Study of complaints and their relation to vertebral destruction in patients with osteoporosis. Bone Miner 1990; 8: 217–229.
3. Pfeifer M, Sinaki M, Geusens P, Boonen S, Preisinger E, Minne HW; ASBMR Working Group on Musculoskeletal Rehabilitation. Musculoskeletal rehabilitation in osteoporosis: a review. J Bone Miner Res 2004; 19: 1208–1214.
4. Sinaki M. Nonpharmacologic interventions. Exercise, fall prevention, and role of physical medicine. Clin Geriatr Med 2003; 19: 337–359.
5. Schroeder S, Rossler H, Ziehe P, Higuchi F. Bracing and supporting of the lumbar spine. Prosthet Orthot Int 1982; 6: 139–146.
6. Bajaj S, Saag KG. Osteoporosis: evaluation and treatment. Curr Womens Health Rep 2003; 3: 418–424.
7. Lin JT, Lane JM. Nonmedical management of osteoporosis. Curr Opin Rheumatol 2002; 14: 441–446.
8. Kaplan RS, Sinaki M, Hameister MD. Effect of back supports on back strength in patients with osteoporosis: a pilot study. Mayo Clin Proc 1996; 71: 235–241.
9. Folz TJ, Sinaki M. A nouveau aid for posture training in degenerative disorders of the central nervous system. J Musculoskel Pain 1995; 3: 59–69.
10. Lynn SG, Sinaki M, Westerlind KC. Balance characteristics of persons with osteoporosis. Arch Phys Med Rehabil 1997; 78: 273–277.

