OBJECTIVE: The aim of this study was to evaluate a speech synthesizer with respect to patterns of use and satisfaction, during a 2-month trial at home, and the usefulness of the word prediction function.
DESIGN: Prospective study.
PARTICIPANTS: Of the 24 patients with severe dysarthria recruited, 10 completed the study. Five patients had cerebral palsy, 3 amyotrophic lateral sclerosis, one locked-in syndrome, and one anoxic brain damage. Mean age was 32 (standard deviation 21) years (range 9–66 years).
METHODS: Each participant received 10 hours of training with the device (Dialo®) and then used it at home for 2 months. The main outcome measures were: level of use recorded by the device, Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) satisfaction score (maximum = 5), and time needed to take dictations of standard-dictionary and personal-dictionary words with and without word prediction.
RESULTS: Level of use varied widely across participants. Overall satisfaction at the end of the home trial was high, with a mean QUEST score of 3.4 (SD 1) and was related to the level of use of the device. Level of satisfaction at the end of the training session could not predict the level of use at home. No significant differences were found in dictation- taking times with and without word prediction. However, 6 of the 10 patients took dictation faster with than without word prediction.
CONCLUSION: This study provides the first evidence supporting the benefits of a speech synthesizer used at home for several weeks. Word prediction is useful for some patients even if increase in dictation speed did not reach significance.
Key words: dysarthria, augmentative and alternative communication, word prediction, speech synthesizer, cerebral palsy, training.
J Rehabil Med 2007; 39: 399–404
Correspondence address: Isabelle Laffont, Hopital Raymond Poincaré, 104 Boulevard Raymond Poincaré, FR-92380 Garches, France. E-mail: isabelle.laffont@rpc.aphp.fr
Submitted March 13, 2006; accepted November 17, 2006
INTRODUCTION
Dysarthria is defined as speech impairment due to abnormal function of the muscles in the face, throat and/or respiratory system. Speech is slow, uncoordinated and slurred or mumbled; in addition, voice volume is weak and voice quality altered. Chronic dysarthria exists as many variants. Thus, respiration, phonation, resonance, and/or oral articulation may be involved in various combinations (1). Severe dysarthria may result in unintelligible speech, profoundly impairing the patient’s ability to communicate. Dysarthria occurs in many conditions including cerebral palsy, locked-in syndrome, traumatic brain injury, amyotrophic lateral sclerosis, Parkinson’s disease and stroke.
In patients with severe dysarthria that cannot be improved by conventional speech therapy, augmentative and alternative communication (AAC) systems can be used (2, 3). Many such systems are available. Among them, speech synthesizers require the ability to read and write, via a computer. The interface between the patient and the synthesizer can be adapted to the patient’s degree of motor impairment (4); thus modular keyboards, single-switch scanning, special mouse devices and touch screens can be used, allowing even those patients with severe quadriplegia to input information into the computer. The design of AAC systems has benefited hugely from technological advances achieved over the last 30 years. Customized symbol communication systems can be built. For example, a computerized system with several levels of screens, each of which can contain grids of scalable icons, has been devised (5). A variety of features of AAC systems has been assessed in earlier studies. For example, Angelo (6) compared 3 different scanning modes; other studies assessed the intelligibility of speech produced by synthesizers (7, 8). Light & Lindsay (9) studied message-encoding strategies, letter or iconic techniques. Yorkston et al. (10) focused on the vocabulary selection strategies.
Several recent studies have investigated training in the use of AAC systems, as well as the use of these systems on an everyday basis. Criteria used to evaluate the usefulness of AAC systems have included level of participation in conversations (11), number of spontaneous requests (12, 13), and hours of use of the device per day (14). To our knowledge, no studies have investigated a large number of outpatients.
Other recent research has focused on the potential benefits of facilitating functions such as word prediction (15–17). Word prediction is designed to facilitate typing: the program stores words used by the patient; when the first letter of a word is typed, a numbered list of words appears on the screen, and typing the number for the desired word inserts that word in the text. This function has rarely been evaluated in neurological patients. Handley-More et al. (16) reports a study on 3 children in grades 4 and 5 (9–10 years aged) who wrote stories, alternating among handwriting, word processing, and word processing with word prediction. The results were variable and the authors concluded that one method was not clearly preferable to another. Tam et al. (17) studied 3 girls and 1 boy aged 10–12 years with spina-bifida and hydrocephalus over a period of 20 days in a copy task to evaluate the effect of word prediction on written productivity from the users’ perspectives. The Canadian Occupational Performance Measure (COPM) was used to measure changes in perception of written productivity. Analysis of individual participant data showed that participants perceived word prediction to have the potential to influence written productivity on some writing tasks. Quantitative analysis using a randomization test did not reveal any significant changes in COPM scores after using word prediction.
Although word prediction has not often been evaluated previously, some other facilitating functions have been the focus of clinical studies. For example, Yorkston et al. (18) evaluated the usefulness of word sequences in saving keystrokes by users of AAC devices compared with letter-by-letter spelling or single-word retrieval. They concluded that long messages (3 words or more) increase communication efficiency when stored in an AAC device.
The purposes of this prospective study was to evaluate subjective satisfaction with a speech synthesizer used at home, to analyse the correlations between subjective satisfaction and real use and to objective benefits from the word prediction function.
MATERIAL AND METHODS
Device
We tested the Dialo® speech synthesizer developed in 2001 by Proteor (Dijon, France) and available in Europe and the USA since 2002. The device is housed in a box measuring 20 × 15 × 5 cm, weighs approximately 1 kg, and is designed to be attached to a wheelchair. It can synthesize speech in 8 languages. Words can be typed either on the keyboard or by single-switch scanning, in which each letter lights up in turn and is selected by the patient. Adjustments can be made to voice quality, volume, language, typing speed, scanning mode, and other features. The Dialo® word prediction function suggests 5 words for each initial letter; these 5 words are those used most often by the patient. For the present study, use-monitoring software was added to the synthesizer to record the total number of keystrokes typed and the number of times the word prediction function was used during the 2-month test period.
Study participants
Between April 2003 and May 2004, 24 patients receiving follow-up at the Physical Medicine and Rehabilitation Department of our institution were recruited to the study. Patients had to be older than 9 years of age (to be able to read and write). Their dysarthria had to be sufficiently severe that an AAC system was required to improve their vocal communication. Finally, study participation was offered only to patients with good global cognition, defined as a total score > 72 on the Signoret’s Battery of Cognitive Efficacy (BEC 96) (19), which evaluates attention, orientation, thinking, memory, recognition, serial learning, fluency, naming and constructional functions.
The 24 recruited patients were able to read and to write via a computer. Several patients used a speech synthesizer, but were dissatisfied with it and wanted to try another model. Some patients used a manual communication board with pictures or letters. Before inclusion, none of them had used a Dialo®. All study participants received information on the study and then signed an informed consent document. The study was approved by the local ethics committee.
Among the 24 patients recruited, 13 were excluded because of severe visual impairment (5 patients), a preference for using a computer rather than a Dialo® (7 patients), or a perception that the Dialo® was too heavy (1 patient). This left 11 patients, among whom one left the study at the end of the training period. Table I shows the characteristics of the 14 patients who did not complete the study. Among the 14 patients who were excluded, 2 used a speech synthesizer and the other 12 a manual communication board.
| Table I. Clinical characteristics of the 13 patients excluded from the study, and of the patient who left the study prematurely. |
| Patient | Gender/ age (years) | Diagnosis | Exclusion criteria | Input method |
| 5 | M/19 | TBI | Stopped the study | Keyboard |
| 12 | M/36 | Stroke | Visual impairment | Keyboard |
| 13 | F/67 | Brain tumour | Visual impairment | Keyboard |
| 14 | F/25 | MS | Visual impairment | Keyboard |
| 15 | F/72 | ALS | Visual impairment | Keyboard |
| 16 | M/61 | ALS | Visual impairment | Keyboard |
| 17 | M/30 | TBI | Refusal (prefers computer) | Scanning |
| 18 | M/28 | CP | Refusal (prefers computer) | Scanning |
| 19 | M/63 | ALS | Refusal (prefers computer) | Scanning |
| 20 | F/69 | ALS | Refusal (prefers computer) | Keyboard |
| 21 | M/24 | CP | Refusal (prefers computer) | Scanning |
| 22 | M/43 | ALS | Refusal (prefers computer) | Scanning |
| 23 | M/61 | ALS | Refusal (prefers computer) | Scanning |
| 24 | F/19 | CP | Refusal (felt the synthesizer was too heavy) | Keyboard |
| TBI: traumatic brain injury; MS: multiple sclerosis; CP: cerebral palsy; ALS: amyotrophic lateral sclerosis. |
The 7 women and 3 men who completed the study had a mean age of 32 (standard deviation (SD) 21) years (range 9–66 years) (Table II). The diagnosis was cerebral palsy in 5 patients, amyotrophic lateral sclerosis in 3 patients, incomplete locked-in syndrome in one patient, and anoxic brain damage in one patient. All 10 patients typed directly on the keyboard. Among them, 4 (3 with cerebral palsy and one with anoxia) used a speech synthesizer prior to the study, but none was familiar with the word prediction function. The others used a manual communication board.
| Table II. Clinical features of the 10 patients who completed the study. |
| Patient | Gender/age (years) | Diagnosis | Input method |
| 1 | F/42 | Cerebral anoxia | Keyboard |
| 2 | M/32 | LIS | Keyboard |
| 3 | F/13 | CP | Keyboard |
| 4 | M/12 | CP | Keyboard |
| 6 | F/57 | ALS | Keyboard |
| 7 | F/50 | ALS | Keyboard |
| 8 | M/66 | ALS | Keyboard |
| 9 | F/31 | CP | Keyboard |
| 10 | F/9 | CP | Keyboard |
| 11 | F/9 | CP | Keyboard |
| LIS: locked-in syndrome; CP: cerebral palsy; ALS: amyotrophic lateral sclerosis. |
Methods
Each of the patients received familiarization with the Dialo® device. Patients who were unable or unwilling to use the device were excluded. The other patients received one hour of training in using the device each day for 10 days. Training was delivered by an occupational therapist and a speech-language pathologist. Patients were evaluated at the end of the 10 training sessions (for satisfaction with the synthesizer). Then, a Dialo® device was lent to the patient for use at his or her home for 2 months. At the end of the 2-month trial, a second evaluation was performed (of satisfaction, level of use and dictations).
Level of use was evaluated by software incorporated into the device. Overall use was assessed based on the total number of keystrokes, and the level of use of the word prediction function was assessed based on the total number of keystrokes involving word prediction keys, during the 2-month period. To evaluate patient satisfaction with the device, we used the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) (20, 21), a questionnaire designed to evaluate satisfaction with assistive devices. Of the 12 items in the questionnaire, 8 are related to the device and 4 to customer support; only the device sub-score was determined for the present study, as customer support was not used. Each of the 8 items in the device sub-score is rated from 1 to 5 (Table III). Patients completed the QUEST at the end of the training period and at the end of the 2-month study period. To evaluate the effectiveness of the word prediction function in increasing speed of communication, each patient performed 2 typing exercises at the end of the 2-month trial period. The occupational therapist dictated words from the Dialo® standard dictionary. The patient typed the words twice, once with and once without the word prediction function, in random order. In addition to a test with the Dialo® standard dictionary, a test with the patient’s personal dictionary as compiled by Dialo® was administered; each of these 2 tests was performed with and without the word prediction function, in random order. For all dictation tests, the time needed for typing was measured in seconds.
| Table III. The 8 items of the device sub-score in the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) and the 5-point scale used to rate each item: 1 = Not satisfied at all, 2 = Not very satisfied, 3 = More or less satisfied, 4 = Quite satisfied and 5 = Very satisfied. |
| QUEST | 1 | 2 | 3 | 4 | 5 |
| Dimensions | | | | | |
| Weight | | | | | |
| Adjustments | | | | | |
| Safety | | | | | |
| Durability | | | | | |
| Simplicity of use | | | | | |
| Comfort | | | | | |
| Effectiveness | | | | | |
Statistical analysis
The level of use of the device was analysed descriptively, as was the level of word prediction function use, the QUEST score at the end of the training period and at the end of the 2-month trial period. The QUEST was compared between high-level users and the other patients using a Mann-Whitney test. The durations of the standard-dictionary dictation and personal-dictionary dictation taken at the end of the 2-month study period with and without the word prediction function were compared using the Wilcoxon test. Data were expressed as means +/– SD. Statistical tests were run on Statview 5.
RESULTS
Level of use of the speech synthesizer
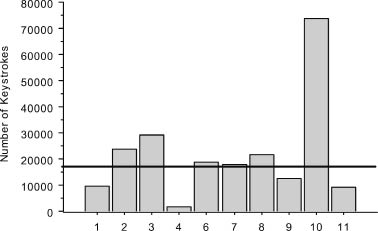
The level of use of the device varied considerably across patients (Fig. 1). Six patients made more than 15,000 keystrokes during the 2-month trial period and were categorized as “high-level users”. This group included all 3 patients with amyotrophic lateral sclerosis, the patient with incomplete locked-in syndrome, and 2 patients with cerebral palsy. Only 2 of these 6 patients (patients 3 and 10) used a speech synthesizer before study inclusion.
Fig. 1. Number of keystrokes (y-axis) performed by each of the 10 patients (x-axis) during the 2-month trial of the Dialo® device at home. The horizontal line separates “high-level user patients” who had more than 15,000 keystrokes during the 2-month trial period and other patients.
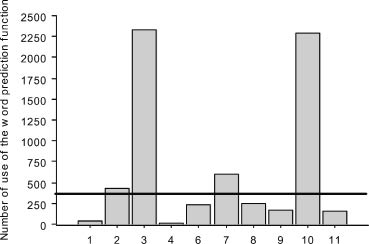
Use of the word prediction function also varied widely across patients (Fig. 2). Only 4 patients used this function more than 300 times during the 2-month period. These 4 patients were among the 6 high-level users.
Fig. 2. Number of uses of the word prediction function (y-axis) by each of the 10 patients (x-axis) during the 2-month trial of the Dialo® device at home. The horizontal line separates patients who used this function more than 300 times during the 2-month period.
Satisfaction
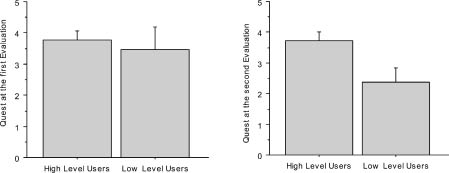
Overall satisfaction with the device was very good. The mean QUEST device sub-score after the 2-month period at home was 3.4 (SD 1) (the maximum being 5). Scores at the end of the training sessions were similar in the 6 “high-level users” and in the other patients (3.77 (SD 0.7) vs 3.47 (SD 1.4); Mann-Whitney, z = −0.426 and p = 0.66). At the end of the 2-month trial period, scores were similar to the baseline values in the 6 high-level users (3.72 (SD 0.66)) but were lower in the other patients (2.36 (SD 0.92); Mann-Whitney, z = −2.025 and p = 0.042) (Fig. 3). For all patients, the least satisfactory feature of the device was its weight.
Fig. 3. Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) scores (y-axis) in high-level (n = 6) and low-level (n = 4) users before (left panel) and after (right panel) the 2-month trial of Dialo® at home.
Dictation speed
The standard-dictionary dictation test given at the end of the 2-month trial period showed no difference between the time with the word prediction function (519 seconds (SD 238); range 196–989 seconds) and the time without the function (499 seconds (SD 221); range 185–913 seconds) (Wilcoxon test, p = 0.269). Because dictation times varied considerably across patients, as shown by the wide SD, we computed the individual percentage of time reduction with the word prediction function on. This showed no improvement related to use of the word prediction function. At the end of the 2-month trial, 6 of the 10 patients had longer times with than without the word prediction function when tested on words from the Dialo® standard dictionary.
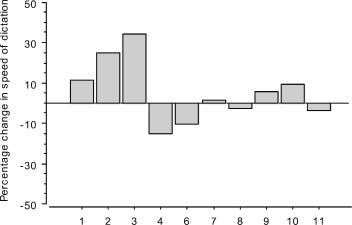
When tested on words from the personal dictionary compiled in each patient by Dialo® during the 2-month trial, a trend toward a shorter dictation time was found with the word prediction function on at the end of the 2-month trial period (453 seconds (SD 158), range 170–655 seconds vs 418 seconds (SD 140); range 188–595 seconds; Wilcoxon test, p = 0.241). When we computed the individual percentage of improvement with the word prediction function on, we found that dictation speed changes ranged from −15% to +34%, compared with the same test without the word prediction function. Of the 10 patients, 6 took the dictation faster with the word prediction function on (Fig. 4).
Fig. 4. Percentage change (y-axis) in speed of dictation-taking when using the word prediction function, compared with speed without the word prediction function. The results for each of the 10 patients are shown. For each patient, the dictation consisted of words stored in the Dialo® personal dictionary during the 2-month trial.
DISCUSSION
The most important conclusion of this study is that a high degree of satisfaction with the Dialo® device was found at the end of the 2-month trial at home, as assessed by the QUEST score, especially in “high-level users”. The extensive training and long trial period at home probably contributed to this result. A strong point of our study is this long period of use of the device at home. To our knowledge, no previous studies evaluated the benefit and real level of use of AAC systems used at home for such a long period.
In the same way, all the patients were satisfied with the device after the 10 training sessions. Satisfaction after the training period could not predict the level of use at home, since the mean QUEST scores were similar in the 6 “high-level users” and in the other patients. After the 2 months at home, “low-level users” were less satisfied with the aid than “high-level users”. This result suggests that satisfaction as measured after the home trial period did relate to some amount of use at home. In any case, the level of use may not fully reflect the magnitude of the communication improvement related to the device. Thus, 5 of our 10 patients continued to use Dialo® after the study and finally purchased it, but only 3 of these 5 were “high-level users”.
This emphasizes the complex problems related to evaluations of AAC systems and the need to measure both level of use and subjective satisfaction. The relationship between real use and personal satisfaction remains complex. For example, in the field of ethnographic research, McCuaig & Frank (22) showed that technology choices by an adult with cerebral palsy were dependent not only on functional usefulness, but also on the patient’s desire to be perceived as able, especially as mentally competent.
The real use of word prediction varied strongly across patients when referring to the number of times this function was used during the 2-month trial at home. It is difficult to relate this fact to some kind of usefulness: even if this function was globally rarely used, it may have been very useful to the patients at those moments. In the same way, increase in dictation speed did not reach significance, even considering the results with the personal dictionary. We just found a trend toward a beneficial effect on speed in “high-level users”. This measurement contrasts with individual results showing that 6 of the 10 patients took dictation faster with word prediction than without it. Consistent with these findings, we cannot conclude that the word prediction function is not useful for some people.
The fact that speed dictations were not statistically improved by word prediction was unexpected and may be explained by several factors. All our patients had severe motor impairments that made use of the device difficult. Thus, the word prediction function may have resulted in a cognitive overload that adversely affected performance. Furthermore, the patients may have had linguistic difficulties that were not detected by the BEC 96. Finally, proper use of the word prediction function may require a very long training period, most notably in patients who are not familiar with assistive technologies and who may have linguistic problems.
Speech synthesizers appear to be of limited usefulness in patients with severe and multiple impairments, compared with multimodal control of several devices via a computer. Computers can now allow communication through specific communication programs (23) using letters, phonemes or icons. These programs could be easy to use and inexpensive, and they could accommodate all switching devices. This may have contributed to the difficulties encountered in recruiting patients for our study. Some integrated devices allow patients to use a single input system for multiple assistive devices, such as a wheelchair, telephone, computer and AAC system. In a study of 24 patients, Angelo & Trefler (24) showed that integrated devices were associated with a high level of satisfaction regarding independence gains and ability to control several appliances, such as television sets and computers. Simplicity, touch sensitivity and visual/auditory feedback appeared to play major roles in satisfaction. However, these integrated devices are at present not easily available and speech synthesizers are the most common AAC systems proposed to patients for 2 main reasons: solidity and portability.
The present study has several limitations. The small sample size, of 10 patients, limited the applicability of regression analysis and Bayesian models, which assume a normal distribution of data. Most patients with severe dysarthria have major motor or visual impairments that limit their ability to use AAC devices and/or to travel to a study site. Moreover, many patients may prefer computer-based AAC systems over speech synthesizers. Further studies of larger numbers of patients are needed. Another limitation of the study is the variability within the subject population. There were 4 different diagnoses, as well as wide variations in age and computer experience. Furthermore, of the 24 patients recruited initially, 14 were excluded, usually because they were unable to type on a keyboard or had severe visual impairment precluding the use of Dialo®. Our findings do not necessarily apply to other AAC systems, some of which are easier to use than Dialo®, even by patients with severe motor impairment.
AAC systems allow patients with severe dysarthria to recover a voice and therefore to participate in vocational and avocational activities that otherwise would be out of their reach. Future challenges for the field of assistive technologies include selection of features associated with optimal performance, development of training methods for patients, and exploration of environmental factors that limit full participation in community-based activities. Further studies of functional outcomes in everyday settings are urgently needed to define better the effectiveness of AAC systems. When designing these studies, one should bear in mind that the number of keystrokes does not fully reflect the efficiency of such devices, and that satisfaction must be taken into account.
ACKNOWLEDGEMENTS
No commercial party having a direct financial interest in the results of the research supporting this article has conferred or will confer a benefit upon the authors or upon any organization with which the authors are associated.
The study was supported by the French Ministry of Research.
REFERENCES
1. Yorkston KM, Strand EA, Kennedy MRT. Comprehensibility of dysarthric speech: implications for assessment and treatment planning. Am J Speech-Lang Pathol 1996: 5; 55–66.
2. Ball LJ, Beukelman DR, Pattee GL. Communication effectiveness of individuals with amyotrophic lateral sclerosis. J Commun Disord 2004; 37: 197–215.
3. Murphy J. Communication strategies of people with ALS and their partners. Amyotroph Lateral Scler Other Motor Neuron Disord 2004; 5: 121–126.
4. LoPresti EF, Brienza DM, Angelo J, Gilbertson L. Neck range of motion and use of computer head controls. J Rehabil Res Dev 2003; 40: 199–211.
5. Blenkhorn P. A picture communicator for symbol users and/or speech-impaired people. J Med Eng Technol 1992; 16: 243–249.
6. Angelo J. Comparison of three computer scanning modes as an interface method for persons with cerebral palsy. Am J Occup Ther 1992; 46: 217–222.
7. Hoover J, Reichle J, Van Tasell D, Cole D. The intelligibility of synthesized speech: ECHO II versus VOTRAX. J Speech Hear Res 1987; 30: 425–431.
8. Keating DL, Evans AL, Wyper DJ, Cunningham E. A comparison of the intelligibility of some low cost speech synthesis devices. Br J Disord Commun 1986; 21: 167–172.
9. Light J, Lindsay P. Message-encoding techniques for augmentative communication systems: the recall performance of adults with severe speech impairments. J Speech Hear Res 1992; 35: 853–864.
10. Yorkston KM, Smith K, Beukelman D. Extended communication samples of augmented communicators. I: a comparison of individualized versus standard single-word vocabularies. J Speech Hear Disord 1990; 55: 217–224.
11. Dattilo J, Camarata S. Facilitating conversation through self- initiated augmentative communication treatment. J Appl Behav Anal 1991; 24: 369–378.
12. Glennen SL, Calculator SN. Training functional communication board use: a pragmatic approach. Augmentative and Alternative Communication 1985; 1: 134–142.
13. Spiegel BB, Benjamin BJ, Siegel SA. One method to increase spontaneous use of an assistive communication device: case study. Augmentative and Alternative Communication 1993; 9: 111–118.
14. Culp DM, Ambrosi DM, Berniger TM. Augmentative communication aid use: a follow up study. Augmentative and Alternative Communication 1986; 2: 19–24.
15. Yorkston KM. Treatment efficacy: dysarthria. J Speech Hear Res 1996; 39: S46–S57.
16. Handley-More D, Deitz J, Billingsley F, Coggins T. Facilitating written word using computer word processing and word prediction. Am J Occup Ther 2003; 57: 139–151.
17. Tam C, Reid DT, Naumann S, O’Keefe B. Perceived benefits of word prediction intervention on written productivity in children with spina bifida and hydrocephalus. Occup Ther Int 2002; 9: 237–255.
18. Yorkston KM, Beukelman DR, Smith K, Tice R. Extended communication samples of augmented communicators. II: Analysis of multiword sequences. J Speech Hear Disord 1990; 55: 225–230.
19. Montani C, Bouati N, Pelissier C, Couturier P, Jasso-Mosqueda G, Hugonot R, Franco A. Scoring and validation of the Clock Face Test in psychometric assessment of elderly subjects. Encephale 1997; 23: 194–199.
20. Demers L, Weiss-Lambrou R, Ska B. Development of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST). Assistive Technology 1996; 8: 3–13.
21. Demers L, Ska B, Giroux F, Weiss-Lambrou R. Stability and reproducibility of the Quebec User Evaluation of Satisfaction with Assistive Technology: J Rehabil Outcomes Meas 1999; 3: 42–52.
22. McCuaig M, Frank G. The able self: adaptive patterns and choices in independent living for a person with cerebral palsy. Am J Occup Ther 1991; 45: 224–234.
23. Newman GC, Sparrow AR, Hospod FE. Two augmentative communication systems for speechless disabled patients. Am J Occup Ther 1989; 43: 529–534.
24. Angelo J, Trefler E. A survey of persons who use integrated control devices. Assist Technol 1998; 10: 77–83.