OBJECTIVE: To determine reliability of maximal grip strength, muscle coordination and muscle endurance. To compare these parameters in young adults with unilateral cerebral palsy and healthy subjects. To evaluate the correlation of these variables with functional activities.
SUBJECTS: Twenty-six healthy subjects and 26 young adults with unilateral cerebral palsy recruited from a cohort study in young adults with cerebral palsy.
METHODS: Maximal grip strength, muscle coordination and muscle endurance were measured in both hands of all subjects. In the healthy subjects test-retest reliability was established. In the young adults with cerebral palsy, the Melbourne assessment and Abilhand Questionnaire were used to determine functional activities.
RESULTS: For the dominant and non-dominant hand the intraclass correlation coefficients for the maximal grip strength were 0.93 and 0.91, for the muscle coordination 0.81 and 0.86, and for the muscle endurance 0.59 for both sides. Maximal grip strength of the involved hand of patients was reduced compared with the uninvolved hand and compared with healthy subjects. There was no difference in muscle coordination and muscle endurance between the involved and uninvolved hands. These parameters, however, were significantly reduced in both hands compared with healthy subjects. Correlations between grip strength parameters and activity limitations were relatively weak and non-linear.
CONCLUSION: Performance of activity is not directly related to grip strength parameters. The uninvolved hand of young adults with unilateral cerebral palsy also has impaired function.
Key words: grip strength, cerebral palsy, functional activities.
J Rehabil Med 2007; 39: 598–604
Correspondence address: Jetty van Meeteren, Erasmus MC-University Medical Centre Rotterdam, Department of Rehabilitation Medicine, PO Box 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: j.vanmeeteren@erasmusmc.nl
Submitted May 30, 2006; accepted March 8, 2007
INTRODUCTION
Cerebral palsy (CP) is an umbrella term for multiple aetiologies and clinical manifestations and is often defined as ”a persistent disorder of posture and movement caused by a non-progressive pathological lesion of the immature brain” (1–4). Patients with CP can have a wide range of symptoms, including spastic paresis, ataxia, dyskinesia, impaired sensation, cognitive disorders, speech disorders, visual and auditory disturbance, and epilepsy (4, 5).
It has been reported that in almost 50% of patients with CP the arm-hand function is impaired, often resulting in limitations in activities and restrictions in participation (5–7). Many patients have reduced muscle strength due to weakness of agonists or a disturbance of muscle tone, such as in spasticity.
Grip strength measurement is a well-known method to investigate hand function, providing insight into the combined action of a number of extrinsic and intrinsic muscles. In several patient groups, grip strength measurement with a dynamometer is known to have excellent reliability (8, 9). To establish abnormal grip strength in patients, grip strength is often compared with normative data, but a disadvantage of this method is that normative data have a large standard deviation (SD) (10). Studies comparing grip force between patients with CP and control subjects have reported conflicting results. One study reported decreased maximal grip force in patients with CP (11), while others reported no differences in static grip force between patients with CP and controls (12, 13).
An alternative method to determine whether grip strength in patients with unilateral disorders is abnormal is to compare the outcome with the contralateral hand (9). However, while in unilateral CP the involved hand can be compared with the uninvolved hand, this may be problematic, since it has been suggested that the uninvolved hand may also be impaired (14, 15). For example, Gordon et al. (16) have described an impaired coordination of fingertip forces of the uninvolved hand of patients with unilateral CP in comparison with normal subjects. Steenbergen et al. (14) suggested that dexterity of the uninvolved hand is impaired because of a deficit in forward movement planning, especially in left hemispheric lesions. Brown et al. (15) found that one-third of patients with unilateral CP had bilateral lesions on a computerized tomography (CT) scan. In the same study, 50% of the children had unilateral lesions with bilateral impairment. Brown et al. (15) suggested that bilateral impairment might result from unilateral lesions, since 10–30% of the lateral cortico-spinal tract consists of uncrossed fibres (17).
While assessment of maximal grip strength can provide valuable insight into the maximal strength of the muscle groups involved, this is not the only important aspect of muscle function. For example, muscle coordination and muscle endurance may not be reflected in a maximal voluntary contraction, while they may be similarly important in the performance of skilled manual tasks in daily activities. It is known that patients with CP have deficits in motor control, mainly due to involuntary co-activation of the antagonistic muscles (13). Several studies (12, 13) reported an impaired force coordination of fingertip forces, resulting in a prolonged and uncoordinated release of a grasped object. In these studies, a strong correlation was found between the impaired force coordination pattern and the level of dexterity.
Thus, in order to evaluate hand muscle function in relation to manual activities, it might be useful to assess not only maximal grip strength, but also other aspects of muscle function, such as muscle coordination and muscle endurance. Both are complex phenomena that may be difficult to assess in a simple task. In the literature, several tasks have been defined to assess aspects of muscle coordination and muscle endurance. For example, a simple task assessing sensorimotor control of the hand muscles was proposed by Kurrilo et al. (18). In this task, subjects had to perform a tracking task in which periodic muscle activation was needed to match a sinus-shaped line on a computer screen by adjusting the grip strength on a dynamometer. A simple task used to assess muscle endurance of the hand muscles is the sustained voluntary contraction. This task has been reported in several patient groups, including patients with multiple sclerosis. Schwid et al. (19) performed a 30-sec sustained maximal grip task in patients with multiple sclerosis and concluded that the fatigue index estimated as the area under the curve (AUC) was reliable and discriminative between patients and healthy subjects.
Grip strength parameters are often used to determine whether hand function is impaired, which may cause limitations in functional activities. However, there is no consensus about the correlation between grip strength and functional activities. In patients with early rheumatoid arthritis, grip strength was an accurate indicator for upper limb ability (20). Other studies, performed in patients with peripheral nerve injuries, reported that besides grip strength, other functions, such as sensory disturbance, also had a correlation with functional activities (21, 22). Within rehabilitation medicine, insight into relationships between the International Classification of Functioning, Disability and Health (ICF) levels body function and functional activities is relevant for a better understanding of the impact of impairments, and measuring on both levels is necessary for a useful evaluation of the effectiveness of rehabilitation treatment (23). The ICF model does not assume a direct causal relation between the severity and nature of impaired functions and limitations in functional activities, since the domains of body function, functional activities and participation are also influenced by personal characteristics of an individual as well as the environmental context that represents a person’s physical and social circumstances.
The overall aim of the study was to establish grip strength parameters, such as maximal grip strength, muscle coordination and muscle endurance of unilateral patients with CP in relation to the performance of functional activities of the upper extremity.
First, we studied the reliability of maximal grip strength, muscle coordination and muscle endurance. In addition, we studied which grip strength parameters (i.e. maximal grip strength, muscle coordination and muscle endurance) were able to differentiate between the involved and the uninvolved hand in young adults with unilateral CP. To establish whether the uninvolved hand of patients with unilateral CP may also have an impaired function, we compared these data with healthy subjects. Finally, we evaluated the relationships between the maximal grip strength, muscle coordination and muscle endurance, and performance of functional activities.
METHODS
Subjects
Twenty-six young adults with unilateral CP and 26 healthy subjects were included in the study. The young adults with CP were recruited from the CP Transition study in south-west Netherlands, a prospective cohort study (24). This cohort was recruited from 8 participating rehabilitation centres and rehabilitation departments in the region. Young adults in this cohort study were diagnosed with CP, and born in the years 1982–86. Exclusion criteria were severe learning disabilities (IQ below 70), additional diagnosis with lasting effects on motor functioning (disorders of the musculoskeletal system), and insufficient knowledge of the Dutch language. Out of 42 young adults with unilateral CP, we randomly selected 26 participants with a mean age 20.6 years (SD 1.2), for the present study (25). Classification according to the Gross Motor Function Classification System (GMFCS) and the Manual Ability Classification System (MACS) showed that this is a population of young adults with CP with high levels (level I) of both the GMFCS and MACS (26, 27). The GMFCS and the MACS are 5-level classification systems for gross motor functioning and manual ability, respectively. Level I represents good, independent functioning. In levels II, III, IV and V the functioning decreases and the subject becomes more dependent on assistance.
The healthy subjects, mean age 21.8 years (SD 4.2), were recruited from students, employees of the rehabilitation department and friends, and matched for age and gender.
The medical ethics committee of Erasmus MC Rotterdam approved the study. All subjects gave their informed consent.
Measurements
For the different tasks, a Mecmesin AFTI (MecMesin limited, Horsham, United Kingdom) force gauge with the Lode handgrip dynamometer (handle position 2) was used, which is similar to the Jamar dynamometer with a distance of 4.6 cm between the handles (Fig. 1). The measurement system was connected to a computer for data acquisition and real-time visual feedback. The force applied to the grip-measuring device was sampled with a frequency of 10 Hz.
Fig. 1. Lode grip dynamometer used for the maximal grip strength, muscle coordination and muscle endurance measurements.
The subject was seated on a chair with both feet placed flat on the floor with the ankles, knees and hips flexed at 90°. The upper arm was adducted, the elbow was flexed at 90° and the forearm was in neutral position without support, as recommended by the American Society of Hand Therapists (28). Both hands were tested and each task was first performed with the dominant or uninvolved hand. Although this could cause a systematic error, the sequence was chosen because the young adults with CP could better understand the task and perform it correctly if they first performed it with the uninvolved hand. The dominant hand was defined as the hand subjects used to write. During all tasks, the same researcher (RvR) instructed the subjects, checked whether they understood the task and verbally encouraged them.
The first task was maximal grip strength, determined as the average of 3 maximal voluntary isometric contractions (MVC) (29). The maximal grip strength measurements were alternated between both hands. No visual feedback was given.
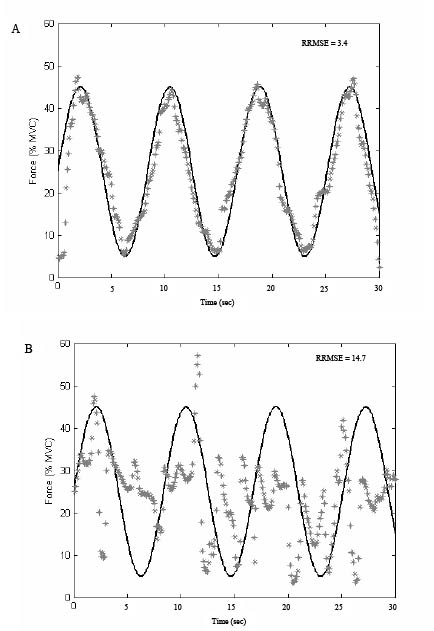
Secondly, a 30-sec dynamic grip-force tracking (muscle coordination) task was performed. In this task, a target signal was presented on the computer screen as a sinus-shaped line ranging between 5% and 45% of the measured MVC. The cycle duration of the sinus was 8.3 sec. The goal of the task was to track the presented target as accurately as possible by applying the appropriate grip strength, presented as dots on the screen (Fig. 2). The tracking task was programmed in Matlab (The Mathworks Inc., Natick, USA). No repetition of the task was performed.
Fig. 2. Example of the muscle coordination task: the sinusoidal line is the target signal presented on the computer screen and the dots represent the performance of the subject. Performance of (A) a healthy subject and (B) a patient with cerebral palsy (CP). RPMSE: relative root mean square error; MVC: maximal voluntary isometric contractions.
Thirdly, the subjects performed the sustained grip strength (muscle endurance) task for both hands. This task contained a maximal isometric contraction over a period of 20 sec. The contraction was started on a sound signal and ended when the researcher gave a sign. Grip strength was continually recorded, but no visual feedback was provided during the task. The task was not repeated.
For the muscle coordination task, no reliability data have been reported. Therefore, test-retest reliability of this task was established in the healthy subjects, as well as for the other grip strength tasks. Between measurements as much rest was given as requested, with at least one min between measurements of the same hand. Data were analysed using the intraclass correlation coefficient (ICC) as estimated from a 2-way mixed effects model.
In the young adults with CP, functional activities were measured using a functional test, the modified Melbourne assessment, and a questionnaire, the Abilhand Questionnaire. The Melbourne assessment is a simple, reliable and easy-to-administer test of a child’s unilateral upper-limb motor function that provides general information about levels of ability and disability (30). The assessment is developed for children aged 5–15 years and consists of 16 items addressing 37 item-scores. The items address, for example, range of movement, target accuracy, fluency of movement, or accuracy of release. Each component is scored on a 3, 4 or 5-point scale. The total score is the sum of all item-scores, converted to a percentage score (0–100). The Melbourne assessment is a reliable tool for measuring the quality of unilateral upper-limb function, but it can be questioned whether the assessment is adequate in children with hemiplegic CP (6). In this study, we selected 4 items of the Melbourne assessment, especially concerning the fine motor hand functions grasping, manipulation and dexterity. These items were performed with both the right and left hand. From the 5 item-scores of both hands we computed an adapted total score, ranging from 0 to 36.
The Abilhand Questionnaire is a questionnaire on bi-manual activities, rating the patient’s perceived difficulty in performing everyday bi-manual activities, such as cutting nails, opening a zip, wrapping up presents and peeling potatoes (31). Rasch analysis in chronic stroke patients led to a hierarchical list of 23 bimanual items, 3-level scaled (31). In the present study we used the Abilhand for chronic stroke patients, because we assumed that young adults with unilateral CP were comparable to this patient group. An explorative Rasch analysis on data collected in the CP Transition study cohort confirmed the unidimensionality of the scale, but not the item hierarchy found in chronic stroke patients (31). Therefore, in the present study we used the raw sum score of the Abilhand Questionnaire, with a maximum score of 46.
Data analysis
Statistical comparison of the grip strength parameters between both hands of patients and healthy subjects was done using the paired t-test. To test differences between the groups, the independent-samples t-test was used.
The performance on the muscle coordination was assessed by calculating the relative root mean square error (RRMSE) between the target (FT) and the measured signal (FM) over the last 10 sec of the task. The error was normalized as a percentage of the mean MVC to permit comparison of the results between patients (18). A lower RRMSE suggests better muscle coordination (32).
RRMSE = 100% *
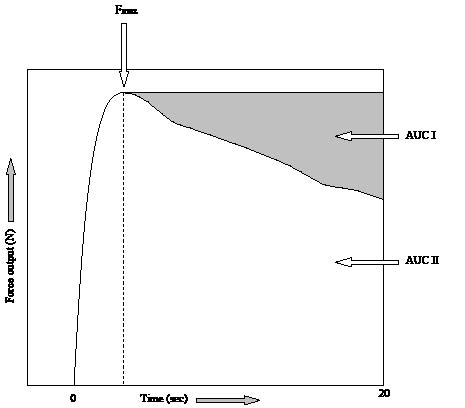
The muscle endurance during the sustained grip strength measurement was quantified using a static fatigue index (SFI) (19). The SFI was calculated from the force-time graph, as the ratio of the AUC of the sustained contraction (AUC II, see Fig. 3) through the hypothetical AUC when no force decline would occur (AUC I + AUC II). Both AUC I and AUC II were calculated from the moment of maximal grip strength until the end of the 20-sec task. A higher SFI corresponds to more force decline, thus less muscle endurance.
Fig. 3. A typical example of the curve of the 20-sec muscle endurance task. Fmax is the maximal grip strength reached, AUC II is the area under the curve of the sustained contraction from the time of reaching Fmax. The sum of AUC I + AUC II is the hypothetical area under the curve when no force decline would occur. Static fatigue index (SFI) = 100% * (1 – (AUC II/(AUC I + II))).
SFI = 100%*
Correlations between the grip strength parameters and measures of functional activities were investigated using Pearson correlation coefficients.
A p-value of 0.05 or less was considered statistically significant.
RESULTS
ICCs of 0.93 and 0.91 were measured for maximal grip strength (dominant and non-dominant hands, respectively), 0.81 and 0.86 for muscle coordination, and 0.59 and 0.59 for muscle endurance.
There were no significant differences between the characteristics of the young adults with CP and healthy subjects (Table I). Ten of the young adults with CP and 11 of the healthy subjects were female. All young adults with unilateral CP were classified as GMFCS level I. For the MACS, 23 young adults were classified as level I, 2 as level II, and one as level III. Data from one young adult with CP could not be used due to technical problems with muscle strength recording.
| Table I. Characteristics of patients with cerebral palsy and healthy subjects |
| | Patients (n = 26) | Healthy subjects (n = 26) | p-value |
| Age (years), mean (SD) | 20.6 (1.2) | 21.8 (4.2) | 0.18 |
| Body mass (kg), mean (SD) | 66.2 (8.3) | 69.1 (11.1) | 0.29 |
| Height (cm), mean (SD) | 174.9 (8.7) | 177.1 (9.5) | 0.40 |
| SD: standard deviation. |
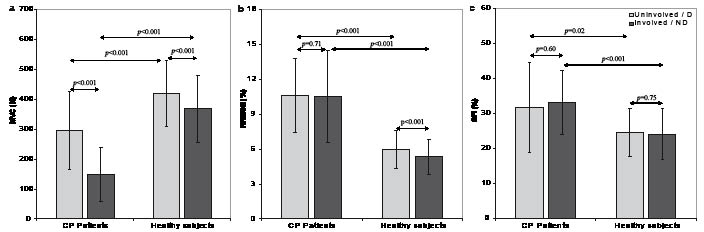
Fig. 4 show the mean values, SD and p-values of the maximal grip strength, muscle coordination and muscle endurance, respectively. In the young adults with CP, maximal grip strength of the involved hand was approximately 50% (p < 0.000) of the uninvolved hand. No significant differences were found for the muscle coordination (p = 0.71) and muscle endurance (p = 0.60) between the involved and uninvolved hand in young adults with CP. In the healthy subjects, the maximal grip strength of the non-dominant hand was 88% (p < 0.000) of the dominant hand. The muscle coordination showed a significant difference between both hands (p < 0.000). No significant difference was found for the muscle endurance between both hands (p = 0.75).
Fig. 4. Mean values and standard deviation of the maximal grip strength (a), muscle coordination (b), and muscle endurance (c) of patients with cerebral palsy (CP) and healthy subjects for the uninvolved or dominant hand (D) and for the involved or non-dominant hand (ND). The p-values of the paired t-test (between both hands) and the independent sample t-test (between both groups) are presented.
MCV: maximal voluntary contractions; RRMSE: relative root mean square error; SFI: static fatigue index.
Comparison of the uninvolved hand of the young adults with CP and the dominant hand of healthy subjects showed significant differences for the maximal grip strength (p < 0.001), the muscle coordination (p < 0.000) and the muscle endurance (p = 0.02). Similarly, all 3 parameters showed a significant difference between the involved side of the young adults with CP and the non-dominant hand of the healthy subjects.
Table II shows the correlation coefficients of the maximal grip strength, muscle coordination and muscle endurance, and assessments of functional activities (modified Melbourne assessment and Abilhand Questionnaire). No significant correlations were found between the 3 grip strength parameters. A significant correlation was found between the Melbourne assessment and the Abilhand Questionnaire. Significant correlations were found between the grip strength parameters and the measures of functional activities. The strongest correlations were found between the maximal grip strength and the Melbourne assessment (0.63, p < 0.01) and between the muscle coordination and the Abilhand Questionnaire (0.45, p < 0.05).
| Table II. Pearson correlation coefficients between the grip strength parameters and measures of functional activities in young adults with cerebral palsy. The grip strength parameters are maximal grip strength (MVC), muscle coordination (RRMSE) and muscle endurance (SFI) |
| | MVC | RRMSE | SFI | Melbourne assessment | Abilhand Questionnaire |
| MVC | – | – 0.36 | 0.06 | 0.63 | 0.35 |
| RRMSE | | – | 0.02 | – 0.20 | – 0.45 |
| SFI | | | – | 0.25 | 0.23 |
| Melbourne assessment | | | | – | 0.49 |
| Abilhand Questionnaire | | | | | – |
| Bold type: statistically significant. MVC: maximal voluntary isometric contraction; RRMSE: relative root mean square error; SFI: static fatigue index. |
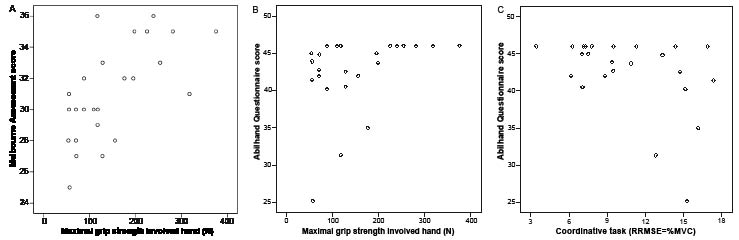
The scatter plots (Fig. 5A–C) show a non-linear relation between the maximal grip strength and the scores of the Melbourne assessment and Abilhand Questionnaire, and between the muscle coordination and the score of the Abilhand Questionnaire. Young adults with CP with a high maximal grip strength or good outcome on the muscle coordination performed well on functional activities. However, while some young adults with CP with low maximal grip strength or a lower coordinative function also had low scores on functional activities, other young adults with CP performed functional activities equally well as young adults with CP with high maximal grip strength and a good result for muscle coordination.
Fig. 5. Scatter plots of the maximal grip strength and the scores of (A) the Melbourne assessment, (B) the Abilhand Questionnaire, and (C) the muscle coordination and the score of the Abilhand Questionnaire of the patients with cerebral palsy (CP).
RRMSE: relative root mean square error; MVC: maximal voluntary isometric contraction.
DISCUSSION
This study compared 3 grip strength parameters (maximal grip strength, muscle coordination and muscle endurance) in young adults with unilateral CP and healthy subjects. In young adults with unilateral CP, the maximal grip strength of the involved hand was reduced compared with the uninvolved hand and compared with healthy subjects. For the muscle coordination and muscle endurance, there was no difference between the involved and uninvolved hand. However, for both these tasks, significant reductions in both hands were found compared with healthy subjects. Correlations between the 3 grip strength parameters and limitations in functional activities were relatively weak and were not linear.
A number of limitations of the present study should be noted. First, the sample frequency of the grip-measuring device was limited to 10 Hz. As a result, high-frequency fluctuations in muscle strength may not have been recorded using this device. While the sample frequency might be relatively low to detect small differences in the muscle coordination task, the differences between patients and healthy subjects in the muscle coordination task were so large that this cannot be explained by the relatively low sample frequency.
Another limitation is that although the muscle coordination task used in this study has been described in patients with neuromuscular diseases (18), the test-retest reliability of this task had not yet been studied. Therefore, we evaluated the test-retest reliability of the muscle coordination and of the other grip strength parameters in the healthy subjects. We found excellent ICC values for the maximal grip strength and muscle coordination, while the ICC of the muscle endurance was moderate (34). The ICC for the maximal grip strength is comparable to studies on other patient groups (9, 35, 36). In addition, the moderate ICC for the muscle endurance is in line with other studies (19, 37). We assumed that the test-retest reliability in young adults with CP would be comparable to healthy subjects. We chose not to perform the reliability study in the young adults with CP because the measurements of this study were performed in addition to more measurements of a prospective cohort study that would also involve many other assessments in the near future. Future studies should indicate the reliability of the muscle coordination in different patient groups. For interpretation of the outcomes, it is important to note the lower reliability of the muscle coordination and especially the muscle endurance as compared with the maximal grip strength. For example, the finding that maximal grip strength is more strongly correlated with functional activities may partly be related to the lower reliability of the muscle coordination and muscle endurance. Future studies developing more reliable outcome measures of muscle coordination and muscle endurance would therefore be valuable.
It should also be noted that the study population consisted of young adults with unilateral CP, with rather good gross motor function and manual ability. Therefore, we can not generalize the present results to a broader population of young adults with unilateral CP, including patients with more severe functional and cognitive consequences of the lesion. In addition, the groups were not matched for the amount of regular physical activity undertaken. As a result, differences in activity level between both groups should be recognized as a potential confounding variable.
While in clinical practice maximal grip strength is used to assess hand function in patients, in the present study we also evaluated 2 other grip strength parameters that we referred to as ”muscle coordination” and ”muscle endurance”. It should be noted, however, that both muscle coordination and fatigue are complex phenomena that may not be optimally evaluated in a simple and easy to administer task. The goal of this study was to evaluate whether the outcome on these tasks differed between the involved and uninvolved hand in young adults with unilateral CP, and between young adults with unilateral CP and healthy subjects. In addition, we evaluated how these tasks relate to limitations in functional activities. We found that both tasks were easy to administer and were able to discriminate between young adults with unilateral CP and healthy subjects. Scores on the muscle coordination and muscle endurance did not correlate more strongly with functional activities than maximal grip strength.
Comparing the maximal grip strength, the muscle coordination and muscle endurance between both hands in young adults with unilateral CP and healthy subjects, we found that both the involved and uninvolved hand scored significantly lower compared with the healthy subjects. This was consistently found in the maximal grip strength, the muscle coordination and the muscle endurance. Overall, these data suggest that the uninvolved hand of young adults with unilateral CP may not have a normal muscle function compared with healthy subjects.
A reduced function of the uninvolved hand is in line with other studies reporting an impaired function of the uninvolved hand of young adults with unilateral CP with respect to control of force (13–16). The underlying mechanism of a bilateral impaired function has not yet been established. A possible explanation might be that muscle coordination of both sides is impaired due to bilateral instead of unilateral lesions. In the present study, young adults with CP were clinically assessed as unilateral CP without scans of the cerebrum. Therefore, it is not certain whether these patients have only a unilateral lesion. On the other hand, it is known that even in patients who have unilateral lesions on a scan, bilateral impairment can be found (15).
The finding that the uninvolved hand of young adults with unilateral CP might also have an impaired function compared with healthy subjects can have important implications for the limitations in functional activities. Although the young adults with CP in the present study have a high MACS level, indicating that they handle objects relatively easily and successfully, the young adults with CP do have limitations in activities based on the Melbourne assessment and the Abilhand Questionnaire scores. While in the MACS, being a classification system, the handling of objects is important, the Melbourne assessment and the Abilhand Questionnaire assess especially capacity and performance of manual activities. While it is generally assumed that patients with unilateral CP are able to perform normally with the uninvolved hand, the present study indicates that this hand may also be involved. As a result, limitations in bimanual activity may not only result from impaired function of the involved hand, but also from impairment of the uninvolved hand.
To what extent impaired hand function is correlated with functional activities had not yet been investigated in these patients. In this study, moderate correlations between the maximal grip strength and muscle coordination on the one hand and functional activities on the other hand were found. Functional activities were most strongly correlated with maximal grip strength and muscle coordination. Inspection of the scatter plots (Fig. 5A–B) indicated that the correlation between the maximal grip strength and functional activities was not linear. More specifically, it was found that young adults with unilateral CP with high maximal grip strength also had high scores on functional activities, while young adults with unilateral CP with relative low maximal grip strength showed a large variation on functional activity scores. This non-linear correlation indicates that limitations in functional activities cannot be estimated directly from maximal grip strength. From the results of this study, we can not explain the nature of this correlation.
The finding that young adults, clinically assessed as unilateral CP, may also have impaired function of the uninvolved hand suggests that more research is needed to understand the underlying reasons for the impaired function of the hand that is considered to be uninvolved. For example, improved brain imaging techniques might increase the sensitivity of detecting cerebral pathology and determine more accurately whether lesions in patients with CP are unilateral or bilateral.
Bilateral involvement in patients diagnosed as having unilateral CP may have important implications for treatment. Currently, treatment such as physical therapy focuses mainly on the involved side, with the intention to improve function, especially in childhood. It is unclear whether this leads to improved functional activities of the upper extremity. It would be interesting to investigate in a randomized controlled trial if the efficacy of a hand function training protocol, focusing on both sides rather then primarily on the involved side, would result in improved function of both hands and, perhaps, fewer limitations in activities. Other treatment modalities focusing on functional activities might be even better because both hands are trained, possibly leading to fewer limitations in activities and participation.
REFERENCES
1. Krägeloh-Mann I, Hagberg G, Meisner C, Schelp B, Haas G, Eeg-Olofson KE, et al. Bilateral spastic cerebral palsy – a comparative study between south-west Germany and western Sweden. I: clinical patterns and disabilities. Dev Med Child Neurol 1993; 35: 1037–1047.
2. Krägeloh-Mann I, Hagberg G, Meisner C, Schelp B, Haas G, Eeg-Olofson KE, et al. Bilateral spastic cerebral palsy – a comparative study between south-west Germany and western Sweden. II: epidemiology. Dev Med Child Neurol 1994; 36: 473–483.
3. Mutch L, Alberman E, Hagberg B, Kodama K, Perat M. Cerebral palsy epidemiology: where are we now and where are we going? Dev Med Child Neurol 1992; 34: 547–555.
4. Bax M, Goldstein M, Rosenbaum P, Leviton A, Paneth N. Proposed definition and classification of cerebral palsy. Dev Med Child Neurol 2005; 47: 571–576.
5. Odding E, Roebroeck ME, Stam HJ. The epidemiology of cerebral palsy: incidence, impairments and risk factors. Disabil Rehabil 2006; 28: 183–191.
6. Fedrizzi E, Pagliano E, Andreucci E, Oleari G. Hand function in children with hemiplegic cerebral palsy: prospective follow-up and functional outcome in adolescence. Dev Med Child Neurol 2003; 45: 85–91.
7. Beckung E, Hagberg G. Neuroimpairments, activity limitations, and participation restrictions in children with cerebral palsy. Dev Med Child Neurol 2002; 44: 309–316.
8. Clerke A, Clerke J. A literature review of the effect of handedness on isometric grip strength differences of the left and right hands. Am J Occup Ther 2001; 55: 206–211.
9. Schreuders TAR, Roebroeck ME, Goumans J, van Nieuwenhijzen JF, Stijnen TH, Stam HJ. Measurement error in grip and pinch force measurements in patient with hand injuries. Phys Ther 2003; 83: 806–815.
10. Crosby CA, Wehbé MA, Mawr B. Hand strength: normative values. J Hand Surg 1994; 19A: 665–670.
11. Valvano J, Newell KM. Practice of a precision isometric grip-force task by children with spastic cerebral palsy. Dev Med Child Neurol 1998; 40: 464–473.
12. Gordon AM, Lewis SR, Eliasson AC, Duff SV. Object release under varying task constraints in children with hemiplegic cerebral palsy. Dev Med Child Neurol 2003; 45: 240–248.
13. Eliasson AC, Gordon AM. Impaired force coordination during object release in children with hemiplegic cerebral palsy. Dev Med Child Neurol 2000; 42: 228–234.
14. Steenbergen B, Meulenbroek RGJ, Rosenbaum DA. Constraints on grip selection in hemiparetic cerebral palsy: effects of lesional side, end-point accuracy, and context. Cognitive Brain Res 2004; 19: 145–159.
15. Brown JV, Schumacher U, Rohlmann A, Ettlinger G, Schmidt RC, Skreczek W. Aimed movements to visual targets in hemiplegic and normal children: is the ”good” hand of children with infantile hemiplegia also normal? Neuropsych 1989; 22: 283–302.
16. Gordon AM, Charles J, Duff SV. Fingertip forces during object manipulation in children with hemiplegic cerebral palsy. II: Bilateral coordination. Dev Med Child Neurol 1999; 41: 176–185.
17. Glees P, Cole J. Ipsilateral representation in the cerebral cortex. Lancet 1952; 1: 1191–1192.
18. Kurillo G, Zupan A, Bajd T. Force tracking system for the assessment of grip force control in patients with neuromuscular diseases. Clin Biomech 2004; 19: 1014–1021.
19. Schwid SR, Thornton CA, Pandya S, Manzur KL, Sanjak M, Petrie MD, et al. Quantitative assessment of motor fatigue and strength in MS. Neurology 1999; 53: 743–750.
20. Adams J, Burridge J, Mullee M, Hammond A, Cooper C. Correlation between upper limb functional ability and structural hand impairment in an early rheumatoid population. Clin Rehabil 2004; 18: 405–431.
21. Jaquet JB, Luijsterburg AJM, Kalmijn S, Kuypers PDL, Hofman A, Hovius SER. Median, ulnar, and combined median-ulnar nerve injuries: functional outcome and return to productivity. J Trauma 2001; 51: 687–692.
22. Bruyns CNP, Jaquet JB, Schreuders TAR, Kalmijn S, Kuypers PDL, Hovius SER. Predictors for return to work in patients with median and ulnar nerve injuries. J Hand Surg [Am] 2003; 28A: 28–34.
23. World Health Organization. International classification of functioning, disability and health. Geneva: WHO; 2001.
24. Donkervoort M, Roebroeck M, Wiegerink D van der Heijden H, Stam H and the Transition Research Group South West Netherlands. Determinants of functioning of adolescents and young adults with cerebral palsy. Disabil Rehabil 2007; 29: 453–463.
25. SCPE: Surveillance of cerebral palsy in Europe. a collaboration of cerebral palsy surveys and registers. Dev Med Child Neurol 2000; 42: 816–824.
26. Wood E, Rosenbaum P. The gross motor function classification system for cerebral palsy: a study of reliability and stability over time. Dev Med Child Neurol 2000; 42: 292–296.
27. Eliasson AC, Krumlinde-Sundholm L, Rösblad B, Beckung E, Arner M, Öhrvall, Rosenbaum P. The Manual Ability Classification System (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol 2006; 48: 549–554.
28. Clinical Assessment Recommendations. 2nd edn. Garner, NC: American Society of Hand Therapists; 1981.
29. Desrosiers J, Bravo G, Hébert R, Dutil E. Normative data for grip strength of elderly men and women. Am J Occup Ther 1995; 49: 637–644.
30. Johnson LM, Randall MJ, Reddihough DS, Oke LE, Byrt TA, Bach TM. Development of a clinical assessment of quality of movement for unilateral upper-limb function. Dev Med Child Neurol 1994; 36: 965–973.
31. Penta M, Tesio L, Arnould C, Zancan A, Thonnard J. The ABILHAND questionnaire as a measure of manual ability in chronic stroke patients. Stroke 2001; 32: 1627–1634.
32. Kriz G, Hermsdorfer J, Marquardt C, Mai N. Feedback-Based training of grip force control in patients with brain damage. Arch Phys Med Rehabil 1995; 76: 653–659.
33. Shrout P, Fleiss JL. Intraclass correlation: uses in assessing rater reliability. Psychol Bull 1979; 86: 420–428.
34. Hanten WP, Chen WY, Austin AA, Brooks RE, Carter HC, Law CA, et al. Maximum grip strength in normal subjects from 20 to 64 years of age. J Hand Ther 1999; 12: 193–200.
35. Peolsson A, Hedlund R, Öberg B. Intra- and inter-tester reliability and reference values for hand strength. J Rehabil Med 2001; 33: 36–41.
36. Kamimura T, Ikuta Y. Evaluation of grip strength with a sustained maximal isometric contraction for 6 and 10 seconds. J Rehabil Med 2001; 33: 225–229.
37. Videler AJ, Beelen A, Aufdemkampe G, Groot IJ de, Leemputte M van. Hand strength and fatigue in patients with hereditary motor and sensory neuropathy (types I and II). Arch Phys Med Rehabil 2002; 83: 1274–1278.