OBJECTIVE: To confirm that electrical myostimulation is a good alternative to conventional aerobic training in patients with chronic heart failure and to compare the effects of both training programmes in patients with different exercise capacities.
Patients and methods: A total of 44 patients with stable chronic heart failure underwent 5 weeks of exercise training, with electrical myostimulation or conventional aerobic training programmes. At baseline and after the training period, patients performed a symptom-limited cardiopulmonary exercise test and a 6-min walk test.
RESULTS: Oxygen uptake at the end of exercise (V.O2 peak) and at ventilatory threshold (V.O2 VT) increased after electrical myostimulation (p< 0.001) and conventional aerobic training (p< 0.001) training programmes. The slope of the relationship between V.O2 and workload was reduced after electrical myostimulation (p< 0.05), but not after conventional aerobic training. Recovery was improved after both training programmes (p< 0.05), and the distance walked in 6 min was increased (p< 0.001). These improvements were not statistically different between electrical myostimulation and conventional aerobic training. Moreover, electrical myostimulation induced greater improvements in patients with low exercise capacity, whereas conventional aerobic training induced improved performance in patients with average exercise capacity.
CONCLUSION: Five weeks of electrical myostimulation and conventional aerobic training exercise training produced similar improvements in exercise capacity in patients with chronic heart failure. However, electrical myostimulation appears to be more effective in patients with low exercise capacity than in those with average exercise capacity.
Key words: chronic heart failure, low-frequency electrical myostimulation, conventional aerobic exercise training, exercise capacity.
J Rehabil Med 2008; 40: 219–224
Correspondence address: Gaelle Deley, Cardiovascular Research Laboratory, Spaulding Rehabilitation Hospital, 125 Nashua Street, Boston, MA 02 114, USA. E- mail: gdeley@partners.org
Submitted May 23, 2007; accepted September 28, 2007
INTRODUCTION
Originally regarded as a contraindication by the Scientific Council on Cardiac Rehabilitation, physical activity has become important in the management of patients with chronic heart failure (CHF) only during the last decade (1). Training programmes usually include aerobic activity alone or in combination with resistance exercise (2, 3) and their benefits are well established (4–7). However, other modes of rehabilitation, such as interval training and electromyostimulation (EMS), have been proposed for patients with CHF, regardless of severity (8–10). Two studies recently demonstrated that low-frequency EMS and conventional aerobic exercise training induce similar benefits in aerobic parameters, field test parameters, and muscle strength in stable patients with CHF (10, 11). However, the number of patients in these studies was small (24 and 30 patients divided into 2 groups). The first aim of the present experiment was therefore to confirm these preliminary results with a comparison of the 2 methods with a larger patient population. Moreover, as suggested by Larsen & Dickstein (12), it is important to identify the CHF population that would benefit most from EMS. Thus, the secondary aim of this study was to compare the effects of EMS and conventional training in CHF patients with different exercise capacities. Therefore, a comparison was made of: (i) cardiorespiratory parameters during moderate to high workloads of exercise (i.e. oxygen uptake (V.O2) at ventilatory threshold (VT) and at the end of exercise, slope of the V.O2/workload relation and V.O2 during recovery); and (ii) submaximal field test parameters.
METHODS
Participants
Table I presents the baseline characteristics of the 44 patients enrolled in this study. They had stable CHF due to dilated or ischaemic cardiomyopathy, an ejection fraction < 40% as measured by echocardiography and were in New York Heart Association (NYHA) classification II–IV. All patients were symptomatically stable and their medical treatment (angiotensin-converting enzyme (ACE) inhibitors, diuretics, beta-blockers) was stable throughout the study. Exclusion criteria were obstructive valvular heart disease and pulmonary disease, acute coronary syndrome or myocardial infarction during the preceding 3 months and evolutive ventricular dysrhythmia. Patients whose activity was limited because of factors other than fatigue and exertional dyspnoea, i.e. angina, arteriopathy, neurological or orthopaedic impairments, which could prevent reliable performance of the exercise tests, were also excluded. The investigation conformed to the principles outlined in the Declaration of Helsinki. All patients gave their written consent after being clearly advised about the protocol, which was approved by the Institutional Ethics Committee.
| Table I. Baseline data (mean (SD)) for the studied population |
| | EMS n = 22 | CONV n = 22 | p-value |
| Sex, M/F | 16 / 6 | 19 / 3 | |
| Age, years | 55 (10) | 56 (7) | 0.6 |
| Weight, kg | 75.1 (15) | 78.8 (15.4) | 0.4 |
| Height, cm | 170.0 (6.7) | 170.9 (6.9) | 0.6 |
| BMI, kg/m² | 25.9 (3.8) | 27 (7.1) | 0.4 |
| LVEF, % | 23.7 (7.4) | 23.2 (10.6) | 0.9 |
| NYHA II / III / IV, n | 9 / 12 / 1 | 11 / 11 / 0 | |
| Dilated cardiomyopathy, n | 13 | 14 | |
| Coronary artery disease, n | 9 | 8 | |
| ACE inhibitors, n | 21 | 21 | |
| Diuretics, n | 20 | 20 | |
| Beta-blockers, n | 11 | 11 | |
| EMS: chronic heart failure patients under low-frequency electrical myostimulation rehabilitation programme; CONV: chronic heart failure patients under conventional rehabilitation programme; ACE: angiotensin-converting enzyme; M: male; F: female; BMI: body mass index (weight/height²); LVEF: left ventricular ejection fraction; NYHA, New York Heart Association. p-value, EMS vs CONV (Student’s t-test). |
Measurements and data analysis
At baseline (PRE) and after the training period (POST), patients underwent a symptom-limited cardiopulmonary exercise test and a 6-min walk test (6-MWT). These tests were performed on separate days in order to avoid fatigue-induced limitation in performance (48-h delay). The symptom-limited cardiopulmonary exercise test was performed first in order to exclude patients presenting contra-indications to the study.
Symptom-limited cardiopulmonary exercise test. As previously described (10), the incremental exercise test was performed on an electromagnetically braked cycle ergometer (Lode, Groningen, The Netherlands). Following a 3-min rest and a 1-min warm-up at 20 Watts (W), the work rate was increased by 10 Watts every min. The exercise test was terminated when the patient was unable to maintain the pedalling rhythm of 60 revolutions per min, limited generally by dyspnoea and/or leg fatigue. A 12-lead electrocardiogram (Case, General Electrics Medical Systems, UK) was monitored throughout the test and auscultatory blood pressure measurements were obtained every 2 min with a standard mercury sphygmomanometer. Gas exchange was measured breath-by-breath using a computerized system (CPX, Medical Graphics, St Paul, MN, USA). From this test, peak V.O2 and peak heart rate were determined and VT was estimated using the method of Beaver et al. (13). The V.O2/workload slope was calculated using linear regression of data from VT to the end of exercise (14). V.O2 was monitored during the recovery period and the time required for a 50% fall from peak V.O2 (T1/2 of V.O2) determined (15). When this occurred in the middle of 2 sampling points, T1/2 was set to the second of these points.
6-minute walk test (6-MWT). A therapist blinded to the exercise test results administered this test. It was performed in a 50-m long unobstructed corridor, using the protocol described by Lipkin et al. (16). Patients were asked to walk as far as possible in 6 min. Slow down and stops for rest were authorized. The total walking distance was measured in m at the end of 6 min. Neither encouragement, nor time information were given during the test.
Exercise training
Following baseline assessment, all patients were blind randomized to receive either a conventional (CONV) or low-frequency EMS ambulatory training. Both training programmes consisted of 1-h sessions, 5 days a week over 5 weeks. According to the recommendations of the European Society of Cardiology (17), patients undergoing conventional training had to perform aerobic exercise (treadmill, bicycle) with a global warm-up and cool-down. Exercise intensity was determined on an individual basis, so that the patient’s target heart rate corresponded to the heart rate at VT (obtained during the initial cardiopulmonary exercise test). During training, exercise intensity was also checked individually by the determination of perceived exertion rating using the Borg scale with a target range between 13 and 15 (10, 18).
The EMS programme was the same as used in our previous study (10). It consisted of a stimulation of both quadriceps and calf muscles using 2 portative dual-channel stimulators (Elpha 2000, Danmeter, Odense, Denmark). Each delivered a low-frequency 10-Hertz biphasic current, with pulse duration of 200 microsec. The stimulus was alternatively on for 12 sec and off for 8 sec. The stimulation intensity for each muscle was increased throughout the training programme according to the patient’s tolerance, in order to be always at the maximum tolerated value (8). If the patient reached the maximum intensity deliverable by the stimulator, the training remained at this level.
Statistical analysis
All data are expressed as mean (standard deviation (SD)). The anthropometric and clinical values were compared between the 2 groups using a Student’s t-test. A two-way analysis of variance (ANOVA) with repeated-measures (group × time) was used to assess each parameter. After this primary analysis, each group was divided into 2 subgroups in order to distinguish the effects of the 2 training modalities according to exercise capacity. The cut-off value of 11 ml/min/kg for V.O2 at VT (19, 20) was used to determine subgroups, termed “average” and “low”. A three-way analysis of variance was then used to assess each parameter.
When the p-value from ANOVA was significant, a post hoc Newmann-Keuls test was used. Significance was set at p < 0.05.
RESULTS
Participants
Prior to rehabilitation, there were no significant differences between the 2 groups for any parameter. A total of 70 patients were screened, 46 were randomly assigned to the 2 groups, and 44 completed the training programme with no significant injury or muscle pain reported in either group (2 patients were excluded from the study due to their lack of compliance during the first 2 weeks of exercise training). Fourteen patients in the “EMS group” reached the maximum intensity deliverable by the stimulator (11 in the “average exercise capacity group” and 3 in the “low exercise capacity group”).
Changes after rehabilitation
Electromyostimulation vs conventional exercise training. Table II presents the values measured during the symptom-limited exercise test and the 6-MWT, before and after both training modalities.
| Table II. Baseline (PRE) and post-training (POST) data (mean (SD)) registered during the tests |
| | EMS | CONV |
| PRE | POST | p-value | PRE | POST | p-value |
| Peak heart rate, beat/min | 136.7 (26.2) | 137.7 (26.3) | – | 133.9 (21.8) | 141.6 (20.3) | – |
| Peak V.O2, ml/kg/min | 16.4 (3.1) | 18.4 (3.6) | † | 16.1 (4.7) | 18.8 (5.7) | † |
| V.O2 at VT, ml/kg/min | 11.0 (2.1) | 12.7 (2.7) | † | 10.9 (1.9) | 12.8 (2.4) | † |
| V.O2/WL, ml O2/W/min | 9.7 (4.0) | 7.9 (2.3) | * | 8.9 (1.9) | 8.6 (2.0) | – |
| T1/2, sec | 114.0 (38.0) | 97.9 (29.9) | * | 116.0 (28.9) | 93.1 (17.9) | * |
| Distance 6-MWT, m | 428.0 (60.4) | 487.1 (57.7) | † | 440.0 (52.1) | 512.7 (46.5) | † |
| p-value, PRE vs POST (Newman-Keuls post hoc): *p < 0.05, †p < 0.001. EMS: patients under low-frequency electrical myostimulation rehabilitation programme; CONV: patients under conventional rehabilitation programme; peak V.O2: oxygen uptake at the end of the symptom-limited cardiopulmonary exercise test; V.O2 at VT: oxygen uptake at ventilatory threshold; V.O2/WL: slope of the oxygen uptake/workload relation above the ventilatory threshold; T1/2: time to recover half of peak V.O2; distance 6-MWT, distance in the 6-minute walk test; SD: standard deviation. |
Peak oxygen uptake was increased by 12.2% after EMS (p < 0.001) and by 16.8% after CONV (p < 0.001). V.O2 at VT was increased by 15.4% after EMS (p < 0.001) and by 17.4% after CONV (p < 0.001). These increases were not significantly different between EMS and CONV protocols.
The slope of the V.O2/WL relationship was decreased after EMS (–18.5%, p < 0.05). This parameter was not significantly modified by CONV (–3.4%, p = 0.9).
T1/2 of V.O2 was decreased after both training protocols (– 14.1% after EMS and – 19.7% after CONV, p < 0.05). The training modality had no influence on this parameter.
Both training protocols induced significant improvements in the distance walked in 6 min (+ 13.8% in EMS and + 16.5% in CONV, p < 0.001). These increases were not significantly different between EMS and CONV protocols.
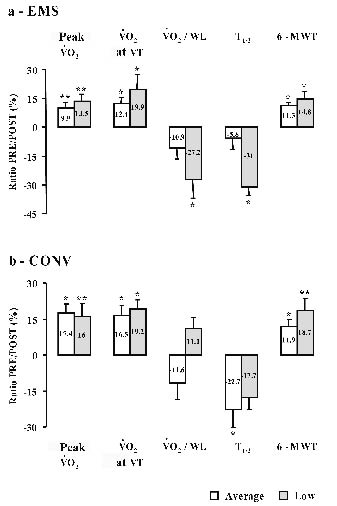
Effects of exercise training in the subgroups. As mentioned above, patients from each group were subdivided according to V.O2 at VT. Patients with V.O2 at VT < 11 ml/min/kg were allocated to the low exercise capacity group and those with V.O2 at VT > 11 ml/min/kg to the average exercise capacity group. Table III presents the number of patients in each subgroup and their baseline values measured for the symptom-limited exercise test and the 6-MWT. Fig. 1 presents the values of the PRE to POST ratios calculated for the different parameters measured during the symptom-limited exercise test (V.O2 peak, V.O2 at VT, slope V.O2/WL and T1/2) and for the distance in the 6-MWT.
| Table III. Baseline data (mean (SD)) registered in the 4 subgroups |
| | EMS | CONV |
| | Average n = 10 | Low n = 12 | p-value | Average n = 11 | Low n = 11 | p-value |
| Peak V.O2, ml/kg/min | 18.2 (2.3) | 15.4 (3.1) | † | 18.1 (2.6) | 15.1 (2.8) | † |
| V.O2 at VT, ml/kg/min | 12.6 (1.9) | 9.5 (0.9) | † | 12.4 (1.4) | 9.8 (1.2) | * |
| V.O2/WL, ml O2/W/min | 10.7 (2.6) | 9.1 (3.0) | – | 9.5 (1.8) | 8.8 (1.8) | – |
| T1/2, sec | 92.4 (23.2) | 128.8 (36.8) | † | 112.1 (35.4) | 120.4 (22.9) | – |
| Distance 6-MWT, m | 441.1 (38.8) | 421.7 (45.0) | – | 460.0 (47.1) | 425.8 (49.7) | – |
| p-value, Average exercise capacity vs Low exercise capacity (Newman-Keuls post hoc): *p < 0.05, †p < 0.01. EMS: chronic heart failure patients under low-frequency electrical myostimulation rehabilitation programme; CONV: chronic heart failure patients under conventional rehabilitation programme; peak : V.O2 oxygen uptake at the end of the symptom-limited cardiopulmonary exercise test; V.O2 at VT: oxygen uptake at the ventilatory threshold; V.O2/WL: slope of the oxygen uptake/workload relation above the ventilatory threshold; T1/2: time to recover half of peak V.O2; distance 6-MWT: distance in the 6-minute walk test. |
After EMS (Fig. 1a), these ratios demonstrate that peak V.O2 (p < 0.01), V.O2 at VT and 6-MWT distance were significantly increased both in average and low exercise capacity patients (p < 0.05). However, V.O2/WL and T1/2 decreased significantly only in the low exercise capacity patients (p < 0.05).
Fig. 1. Pre to post ratio for oxygen uptake at the end of the symptom-limited cardiopulmonary exercise test (V.O2 peak) and at ventilatory threshold (V.O2 VT), slope of the V.O2/workload relation (V.O2/WL), half -recuperation time of V.Oz (T1/2) and distance in the 6-minute walk test (6-MWT) in “average exercise capacity” () and "low exercise capacity" () patients. (a) After electromyostimulation (EMS). (b) After conventional training. Values are expressed as mean (standard deviation (SD)). *p ≤ 0.05, **p < 0.01, differences of the PRE to POST ratio (Newman-Keuls post hoc).
After conventional training (Fig. 1b), all patients demonstrated significant increases in peak V.O2, V.O2 at VT and 6-MWT distance (p < 0.05), whereas only average exercise capacity patients demonstrated a significant improvement in T1/2. The slope V.O2/WL was not significantly modified by conventional training in either subgroup.
Comparison of the percentage increase in average vs low exercise capacity patients suggests greater improvements in all parameters in low exercise capacity patients compared with average exercise capacity patients after EMS; whereas after CONV V.O2 peak, slope V.O2/WL and T1/2 showed a greater improvement in average exercise capacity patients. However, there was no significant difference.
DISCUSSION
Programmes of physical activity, either aerobic and/or strength exercises, are used as supplemental treatment for patients with CHF (5). However, these interventions are usually only proposed for patients with moderate symptoms. Patients with severe CHF are often excluded due to excessive symptoms and dyspnoea. Interval training has therefore been proposed for patients with severe CHF, since it allows intense exercise stimuli to be delivered to peripheral muscles with minimal cardiac strain (21). In fact, EMS, in particular low-frequency EMS training, has been proposed as an interesting alternative to interval training, since it is simple, well-tolerated by patients with CHF, and produces an intense exercise stimulus to the peripheral muscles with low cardiac demand (8–11).
Our results demonstrate increases of peak V.O2 by 12.2% and 16.8% after EMS and CONV, respectively (Table II). These results, in accordance with those of previous studies (8, 9, 22), are of great interest, as peak V.O2 is considered a main predictor of death (23). However, peak V.O2 needs to be considered with other indices. VT is an interesting and objective parameter that can be derived from submaximal exercise. Although controversy exists concerning the mechanisms determining VT, adaptations at the peripheral level must be involved (24, 25). Thus, the 15.4% and 17.4% increases of V.O2 at the VT after EMS and conventional training are very interesting since both enhance the subjects’ capacity to perform sustained submaximal activities (25).
In the present experiment, we were particularly interested in the effects of both training protocols on the slope of the V.O2/WL relationship and its relation to the T1/2 value. Indeed, it has been suggested that the lower the V.O2/workload slope value and the longer the T1/2 value, the more severe is the CHF (26–30). The inverse correlation between exercise V.O2/workload and T1/2 value implies that CHF patients with a low V.O2/workload during exercise were not efficient, but rather were accumulating a large oxygen debt that was repaid after the completion of exercise. Our results reveal a significant decrease in the V.O2/workload slope after EMS and of T1/2 after both protocols (Table II). These results are similar to those found in our previous study (10) and suggest that after only 5 weeks, EMS induces intramuscular changes improving V.O2 kinetics (22). Indeed, if a decreased V.O2/workload slope, per se, could be considered as an aggravation of the pathology (29), when accompanied by a faster recovery, it suggests that muscles are able to work harder with less oxygen and without accumulating debt that results in a longer recovery from exercise. This more efficient kinetics of oxygen uptake during exercise could be explained by EMS training-induced modification of the myotypology (i.e. an increase in the relative distribution of type I myosin heavy chain isoforms and a decrease in type IIx myosin heavy chain isoforms (22)) since the motor recruitment pattern and percentage distribution of type IIx fibres are thought to be the main determinants of V.O2 kinetics above the VT (14). For a given workload, type I fibres are more efficient than type IIx fibres in terms of oxygen requirement (14, 31).
Walk tests have recently been demonstrated to directly evaluate physical performance related to activities of daily living (32, 33). The present study found increased performance in the 6-MWT comparable to previous studies (8, 10), suggesting improved functional capacity. This result is very interesting, since it may relate to better autonomy, physical independence and increased quality of life for trained patients (34).
As suggested by Larsen & Dickstein (12), low-frequency EMS is a very attractive intervention, but it is necessary to identify the population most likely to benefit from it. The second aim of the present experiment was therefore to investigate the effects of both training modalities in patients differently deconditioned. The value of V.O2 at VT, and more precisely, the critical value of 11 ml/min/kg (19, 20), has been identified previously as able accurately to separate patients by fitness. Indeed, we thought that it was the most objective and accurate parameter to evaluate the patients’ exercise capacities and to separate patients with average and low exercise capacities.
The results of this study show that the greatest improvements in all parameters after EMS occurred in patients with low exercise capacity. These results are not surprising regarding the development of heart failure: the disease and the subsequent inactivity lead to deconditioning characterized by alterations at the peripheral level, such as skeletal muscle atrophy, changes of fibre-composition, reduced capillary density and reduced cytochrome oxidase activity (35, 36). Thus, a method mainly improving peripheral factors, such as EMS, seems to be of great interest and particularly effective to improve exercise capacities in low exercise capacity patients. Regarding patients with average exercise capacity, the results may be explained by an insufficient intensity of stimulation. Indeed, some patients reached the maximum intensity deliverable by the stimulator after only a few weeks and therefore trained during several weeks at a submaximal intensity. It is well known that EMS-induced benefits are related to the stimulation intensity and that at least 4 weeks at the maximal tolerable intensity are necessary to induce significant modifications of the myotypology (increased transcription of myosin heavy chain-I and decreased transcription of myosin heavy chain-IIx) and the enzyme activity (increased oxidative potential) (37).
Our results also show that after conventional training, improvements in most parameters (V.O2 peak, slope V.O2/workload and T1/2) were greater in patients with average exercise capacity. These results may also be due to the training intensity: in most patients from the low group, the exercise capacity at baseline did not allow training work rates in excess of approximately 40 W. As the patients were already accustomed to these intensities from activities of daily living, training at this level would probably have had only slight effects (e.g. 21).
This could also explain the increased value of the slope V.O2/workload obtained after conventional training in patients with low exercise capacity (whereas this parameter was decreased in patients with average exercise capacity). Indeed, as suggested above, the motor recruitment pattern and percentage distribution of type IIx fibres are thought to be the main determinants of V.O2 kinetics above the VT (14). For a given workload, type I fibres are more efficient compared with type IIx fibres in terms of oxygen requirement (14, 31). While aerobic training performed at or above the VT induces an increase in skeletal muscles oxidative capacity (a shift from type II to type I fibres and an increase in total volume density of mitochondria, a lower training intensity is not sufficient to induce these modifications (38, 39).
Study limitations
One could argue that the results of this study are not new, since several groups have already reported similar findings (9–11). However, as mentioned above, there is a need for repetition of studies investigating the effects of this method in order to assemble a body of evidence regarding its effectiveness. The parameter chosen to separate average and low exercise capacity patients, i.e. V.O2 at VT, may also be questionable. However, in regards of the literature, authors were of the opinion that this parameter is more accurate than peak V.O2 (40), NYHA class or left ventricular ejection fraction (41, 42).
Conclusions about the effects of EMS and conventional training in the subgroups are based on comparisons of percentage increases for each parameter. A greater number of patients are needed to highlight statistical differences.
In conclusion, 5 weeks of low-frequency EMS or conventional aerobic exercise training induce similar beneficial effects on aerobic variables (assessed across the moderate to high workloads and during recovery), and on field test parameters in stable patients with CHF. These results therefore confirm that EMS is not only a good alternative to conventional rehabilitation, eliciting improvements of peripheral factors, but also an interesting new method, opening the door of rehabilitation to the most severely affected patients. However, due to the small number of patients in each subgroup (and thus the low statistical power of this study), caution should be applied when considering the results. An extension of this work would be to assess the effects of EMS in a larger population of patients with severe heart failure.
REFERENCES
1. Dickstein K, Aarsland T. Which patients with heart failure are likely to benefit from participation in an exercise training program? Heart Failure Rev 1999; 3: 283–286.
2. Remme WJ, Swedberg K. Comprehensive guidelines for the diagnosis and treatment of chronic heart failure. Task force for the diagnosis and treatment of chronic heart failure of the European Society of Cardiology. Eur J Heart Fail 2002; 4: 11–22.
3. Giannuzzi P, Mezzani A, Saner H, Bjornstad H, Fioretti P, Mendes M, et al. Physical activity for primary and secondary prevention. Position paper of the Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology. Eur J Cardiovasc Prev Rehabil 2003; 10: 319–327.
4. Belardinelli R, Georgiou D, Cianci G, Purcaro A. Randomized, controlled trial of long-term moderate exercise training in chronic heart failure: effects on functional capacity, quality of life, and clinical outcome. Circulation 1999; 99: 1173–1182.
5. Belardinelli R, Georgiou D, Scocco V, Barstow TJ, Purcaro A. Low intensity exercise training in patients with chronic heart failure. J Am Coll Cardiol 1995; 26: 975–982.
6. Piepoli MF, Davos C, Francis DP, Coats AJ. ExTraMATCH Collaborative. Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ 2004; 328: 189.
7. Smart N, Marwick TH. Exercise training for patients with heart failure: a systematic review of factors that improve mortality and morbidity. Am J Med 2004; 116: 714–716.
8. Maillefert JF, Eicher JC, Walker P, Dulieu V, Rouhier-Marcer I, Branly F, et al. Effects of low-frequency electrical stimulation of quadriceps and calf muscles in patients with chronic heart failure. J Cardiopulm Rehabil 1998; 18: 277–282.
9. Harris S, LeMaitre JP, Mackenzie G, Fox KA, Denvir MA. A randomised study of home-based electrical stimulation of the legs and conventional bicycle exercise training for patients with chronic heart failure. Eur Heart J 2003; 24: 871–878.
10. Deley G, Kervio G, Verges B, Hannequin A, Petitdant MF, Salmi-Belmihoub S, et al. Comparison of low-frequency electrical myostimulation and conventional aerobic exercise training in patients with chronic heart failure. Eur J Cardiovasc Prev Rehabil 2005; 12: 226–233.
11. Dobsak P, Novakova M, Fiser B, Siegelova J, Balcarkova P, Spinarova L, et al. Electrical stimulation of skeletal muscles. An alternative to aerobic exercise training in patients with chronic heart failure? Int Heart J 2006; 47: 441–453.
12. Larsen AI, Dickstein K. Can sedentary patients with heart failure achieve the beneficial effect of exercise training without moving? Eur Heart J 2004; 25: 104–106.
13. Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 1986; 60: 2020–2027.
14. Lucia A, Rivero JL, Perez M, Serrano AL, Calbet JA, Santalla A, et al. Determinants of VO(2) kinetics at high power outputs during a ramp exercise protocol. Med Sci Sports Exerc 2002; 34: 326–331.
15. Nanas S, Nanas J, Kassiotis C, Nikolaou C, Tsagalou E, Sakellariou D, et al. Early recovery of oxygen kinetics after submaximal exercise test predicts functional capacity in patients with chronic heart failure. Eur J Heart Fail 2001; 3: 685–692.
16. Lipkin DP, Scriven AJ, Crake T, Poole-Wilson PA. Six minute walking test for assessing exercise capacity in chronic heart failure. Br Med J (Clin Res Ed) 1986; 292: 653–655.
17. Working Group on Cardiac Rehabilitation & Exercise Physiology and Working Group on Heart Failure of the European Society of Cardiology. Recommendations for exercise training in chronic heart failure patients. Eur Heart J 2001; 22: 125–135.
18. Verges B, Patois-Verges B, Cohen M, Lucas B, Galland-Jos C, Casillas JM. Effects of cardiac rehabilitation on exercise capacity in type 2 diabetic patients with coronary artery disease. Diabet Med 2004; 21: 889–895.
19. Weber KT, Janicki JS. Cardiopulmonary exercise testing for evaluation of chronic cardiac failure. Am J Cardiol 1985; 55: 22A–31A.
20. Gitt AK, Wasserman K, Kilkowski C, Kleemann T, Kilkowski A, Bangert M, et al. Exercise anaerobic threshold and ventilatory efficiency identify heart failure patients for high risk of early death. Circulation 2002; 106: 3079–3084.
21. Meyer K, Samek L, Schwaibold M, Westbrook S, Hajric R, Beneke R, et al. Interval training in patients with severe chronic heart failure: analysis and recommendations for exercise procedures. Med Sci Sports Exerc 1997; 29: 306–312.
22. Nuhr MJ, Pette D, Berger R, Quittan M, Crevenna R, Huelsman M, et al. Beneficial effects of chronic low-frequency stimulation of thigh muscles in patients with advanced chronic heart failure. Eur Heart J 2004; 25: 136–143.
23. Myers J, Gullestad L, Vagelos R, Do D, Bellin D, Ross H, et al. Clinical, hemodynamic, and cardiopulmonary exercise test determinants of survival in patients referred for evaluation of heart failure. Ann Intern Med 1998; 129: 286–293.
24. Santa-Clara H, Fernhall B, Mendes M, Sardinha LB. Effect of a 1 year combined aerobic- and weight-training exercise programme on aerobic capacity and ventilatory threshold in patients suffering from coronary artery disease. Eur J Appl Physiol 2002; 87: 568–575.
25. Piepoli MF, Corra U, Agostoni PG, Belardinelli R, Cohen-Solal A, Hambrecht R, et al. Statement on cardiopulmonary exercise testing in chronic heart failure due to left ventricular dysfunction: recommendations for performance and interpretation. Part I: definition of cardiopulmonary exercise testing parameters for appropriate use in chronic heart failure. Eur J Cardiovasc Prev Rehabil 2006; 13: 150–164.
26. Itoh H, Taniguchi K, Koike A, Doi M. Evaluation of severity of heart failure using ventilatory gas analysis. Circulation 1990; 81 Suppl: II31–II37.
27. Solal AC, Chabernaud JM, Gourgon R. Comparison of oxygen uptake during bicycle exercise in patients with chronic heart failure and in normal subjects. J Am Coll Cardiol 1990; 16: 80–85.
28. Cohen-Solal A, Laperche T, Morvan D, Geneves M, Caviezel B, Gourgon R. Prolonged kinetics of recovery of oxygen consumption after maximal graded exercise in patients with chronic heart failure. Analysis with gas exchange measurements and NMR spectroscopy. Circulation 1995; 91: 2924–2932.
29. Koike A, Itoh H, Kato M, Sawada H, Aizawa T, Fu LT, Watanabe H. Prognostic power of ventilatory responses during submaximal exercise in patients with chronic heart disease. Chest 2002; 121: 1581–1588.
30. Mitchell SH, Steele NP, Leclerc KM, Sullivan M, Levy WC. Oxygen cost of exercise is increased in heart failure after accounting for recovery costs. Chest 2003; 124: 572–579.
31. Barstow TJ, Jones AM, Nguyen PH, Casaburi R. Influence of muscle fiber type and pedal frequency on oxygen uptake kinetics of heavy exercise. J Appl Physiol 1996; 81: 1642–1650.
32. Larsen AI, Aarsland T, Kristiansen M, Haugland A, Dickstein K. Assessing the effect of exercise training in men with heart failure; comparison of maximal, submaximal and endurance exercise protocols. Eur Heart J 2001; 22: 684–692.
33. Kervio G, Carre F, Ville NS. Reliability and intensity of the six-minute walk test in healthy elderly subjects. Med Sci Sports Exerc 2003; 35: 169–174.
34. Poole-Wilson PA. The 6-minute walk. A simple test with clinical application. Eur Heart J 2000; 21: 507–508.
35. Lipkin DP, Jones DA, Round JM, Poole-Wilson PA. Abnormalities in patients with chronic heart failure. Int J Cardiol 1988; 18: 187–195.
36. Piepoli MF, Scott AC, Capucci A, Coats AJ. Skeletal muscle training in chronic heat failure. Acta Physiol Scand 2001; 171: 295–303.
37. Pette D, Vrbova G. What does chronic electrical stimulation teach us about muscle plasticity? Muscle Nerve 1999; 22: 666–677.
38. Hambrecht R, Niebauer J, Fiehn E, Kalberer B, Offner B, Hauer K, et al. Physical training in patients with stable chronic heart failure: effects on cardiorespiratory fitness and ultrastructural abnormalities of leg muscles. J Am Coll Cardiol 1995; 25: 1239–1249.
39. Hambrecht R, Fiehn E, Yu J, Niebauer J, Weigl C, Hilbrich L, et al. Effects of endurance training on mitochondrial ultrastructure and fiber type distribution in skeletal muscle of patients with stable chronic heart failure. J Am Coll Cardiol 1997; 29: 1067–1073.
40. Noonan V, Dean E. Submaximal exercise testing: clinical application and interpretation. Phys Ther 2000; 80: 782–807.
41. Franciosa JA, Park M, Levine TB. Lack of correlation between exercise capacity and indexes of resting left ventricular performance in heart failure. Am J Cardiol. 1981; 47: 33–39.
42. Cohen Solal A, Gourgon R. Assessment of exercise tolerance in chronic congestive cardiac failure. Am J Cardiol 1991; 67: 36–40.