OBJECTIVE: To characterize the mental and physical functioning of subjects admitted to Beitostølen Healthsports Centre, and evaluate whether functioning was improved during rehabilitation.
Material and methods: A total of 228 subjects admitted for rehabilitation completed the Medical Outcome Study Short Form 12 (SF-12) on admission and on discharge after approximately 4 weeks. A total of 174 subjects also completed SF-12 3 months after discharge. The physical and mental sum scores and the scores for the 8 subscales of SF-12 were calculated. In a stepwise backward multiple regression model, demographic and medical factors influencing improvement during rehabilitation were explored.
RESULTS: Physical, as well as mental, functioning was reduced on admission. Bodily pain and emotional factors represented the most dominant components. Both physical and mental functioning improved during the stay, and the improvement in physical functioning remained stable 3 months after discharge. The improvement in physical functioning was greatest for those subjects living in urban areas and having a painful musculoskeletal diagnosis. The improvement in mental functioning was greatest for females.
CONCLUSION: This approach to rehabilitation appears to be effective for improving physical functioning in the relevant group of individuals. However, carefully controlled studies with longer follow-up periods are required.
Key words: physical activity, rehabilitation, participation, SF-12, impairment.
J Rehabil Med 2008; 40: 410–417
Correspondence address: Cecilie Røe, Department of Physical Medicine and Rehabilitation, Ulleval University Hospital, NO-0407 Oslo, Norway. E-mail: eller@medisin.uio.no
Submitted April 22, 2007; accepted January 2, 2008
Introduction
The present study was undertaken in order to characterize the mental and physical functioning of the population admitted to Beitostølen Healthsports Centre (BHC) for rehabilitation, and to evaluate whether functioning improved during rehabilitation.
BHC is a rehabilitation hospital offering secondary rehabilitation to persons with impairments and disabilities. It is located in the mountains in southern Norway. The treatment philosophy has been to help disabled people to achieve a better quality of life by means of physical, but also social and cultural, activities.
Living with impairments is associated with various problems, ranging from reduced physical fitness to mental problems, which eventually influence the quality of life of this population (1, 2). These individuals also struggle with pain, which limits activity and participation (3). Both pain and physical activity seem to interplay with psychological functioning, in particular depression (4). In turn, physical inactivity may gradually add to their initial impairments and increase the functional consequences of the impairments. Another implication of reduced physical capacity is that activities of daily life require most of, or more than, the subject’s functional capacity.
The importance of physical activity is well documented in the general population. Mortality is reduced by its preventive effect on cardiovascular and other lifestyle diseases (5). Physical activity also improves muscular function when force and endurance capacity are included (6). Exercise treatment also improves mental aspects, such as depression (7). These benefits are also shown in a population with impairments and chronic diseases (8, 9). However, there are limited opportunities for many of the individuals with impairments to participate in community physical activities (10). One factor often ignored, is that some of these individuals have been told that engaging in physical activity may actually be harmful (11). Therefore emphasis must also be put on the information and motivation aspect. Special adaptations to exercise and activity programmes, as well as adjustments at the individual level, may also be necessary. Hence, traditional medical treatment and sports clubs often fail to reach this group.
Several adapted physical activity programmes have been developed (12). However, their effects have rarely been evaluated. Given the wide variety of impairments, the measurement of outcomes is difficult. However, it may be possible to overcome the heterogeneity of individual impairments using relatively crude outcome measurements for physical and mental functioning (13).
The rehabilitation programmes at BHC are based on the vision of Adapted Physical Activity (APA) (14, 15). The main philosophy is that physical activity is important for physical and mental health. However, in order to achieve these benefits the physical activity must meet the patients’ preferences and be adapted to their capabilities (16). Removing environmental obstacles as well as providing individually adapted instructions and technical aids may facilitate physical activity. Subjects may benefit from experiencing participation and coping, as well as an improvement in physical capacity, which may contribute to improved mental functioning. Emphasis is also placed on activities that can be maintained after discharge, in order to facilitate continued physical activity. This strategy needs to be evaluated. Knowledge of both the factors influencing the effects of rehabilitation on these subjects, and the duration of the effects are of great importance.
The main aim of the present work was to evaluate the rehabilitation programme at BHC. The specific questions addressed were:
• What is the physical and mental functioning of subjects admitted for rehabilitation at BHC?
• Which factors predict changes in physical and mental functioning during rehabilitation?
• Do changes in physical and mental functioning persist 3 months after discharge?
Material and methods
Subjects
Approximately 500 adults from 4 of the 5 health regions in Norway are referred to BHC each year. Thirty-five percent of subjects are referred directly from hospitals and 65% from local physicians in the community. Forty percent of the referred patients are rejected, because of their primary psychiatric diagnosis, or because it is revealed that they are dependent on help for personal activities of daily living. Some of the rejections are also due to capacity problems at BHC or due to the subject recently having received rehabilitation at BHC.
In 2 periods, from February to May 2004 and February to September 2005, all subjects (n = 313) receiving rehabilitation at BHC were asked to report their physical and mental functioning using the Medical Outcome Study Short Form 12 (SF-12). Fifty-six subjects did not reply, and 29 completed the form only at admission. Hence, the study group, which comprised subjects completing the form both on admission and departure, numbered 228 subjects (72%). Fifty-five percent (n = 174) also responded at the 3-month follow-up. The characteristics of the different groups are given in Table I. Of the main study group (n = 228), only 12.5% were working full-time or studying, and 24% were on part-time or full-time sick-leave or undergoing rehabilitation. Forty-six percent received full disability pension, 17% combined disability pension and part-time work and 1% were unemployed. The median disease duration was 11 (interquartile range 16) years. The subjects had a wide variety of medical problems. Approximately one-third (29%) had painful musculoskeletal problems including rheumatic diseases, and one-third (31%) had various neurological problems. Fifteen percent were in need of rehabilitation after various traumas. Subjects with cardiovascular diseases including stroke (10%), sequelae after cancer (5%), genetic diseases and blindness (10%) were also represented.
The study was approved by the Regional Medical Committee for Research Ethics in Norway.
| Table I. Characteristics of the subjects invited to participate, those completing SF-36 at admission to Beitostølen Healthsports Centre but not later on, those completing SF-36 at admission and departure, and follow-ups at 3 months. Physical (PCS) and mental (MCS) sum score of SF-12 for the latter 3 groups |
| | Invited n = 313 | Admission n = 257 | Admission and departure n = 228 | Follow-up at 3 months n = 174 |
| Age (years), mean (SD) | 45 (12)* | 47 (12) † | 48 (11) | 49 (11) |
| Gender (% males) | 49 | 48 | 48 | 47 |
| Duration of disease (years), mean (IQR) | 8.5 (2) | 10 (2) | 11 (3) | 9 (2) |
| Musculoskeletal diseases (%) | 22 | 22 | 29 | 30 |
| Rural settlement (%) | 40 | 42 | 40 | 41 |
| Married/cohabiting (%) | 56 | 59 | 60 | 61 |
| Disability pensioned (%) | 41% | 43 | 46 | 47 |
| PCS, mean (SD) | | 31 (11) | 31 (11) | 39 (13) |
| MCS, mean (SD) | | 48 (14) | 47 (14) | 55 (12) |
| *p < 0.05 for with the invited subjects not completing SF-12 (n = 56) compared with the subjects completing SF-12 at admission (n = 257). †p < 0.05 for comparison of 29 subjects completing SF-12 at admission compared with the subjects completing SF-12 at both admission and departure (n = 228) SD: standard deviation; IQR: interquartile range; SF-36: short form health survey; SF-12: medical outcome study short form 12. |
Procedures on admission
All subjects were examined by a medical doctor on arrival, and also by health professionals according to the subject’s special needs. Physiotherapists, nurses, social workers and sports pedagogues comprised the other professions involved. A team was organized for each subject. On the second day, the team and the patient made a detailed goal-oriented plan for their rehabilitation at BHC and during the follow-up period.
Rehabilitation programme at BHC
BHC accommodates 30 adults at a time. Besides accommodation, BHC offers a wide range of training and treatment facilities with a large sports hall, swimming and therapy pools, physiotherapy premises, testing laboratories, horse stables with an indoor riding hall and rooms for various leisure activities. The centre has 200 acres of land with a sports stadium, a lake for water sports and fishing, paved paths, cabins, cross country-tracks and an alpine ski hill.
The usual length of stay for adults is 28 days, ranging from 19 to 37 days in the relevant group, but 80% stayed between 24 and 32 days. The rehabilitation programme is based on physical activities, adapted to the specific needs of each individual with disabilities. “Adapted” means facilitating participation in an activity in spite of, and not because of, a disability. The rehabilitation includes social and cultural activities and extensive use of outdoor natural facilities on a year-round basis. A wide range of services is offered, including adaptation of the environmental factors, technical aids and individual instruction. Such services may be essential in order to participate in the activities, or recommended in order to obtain the optimal effect of the activity programme. Skilled professionals with personal experience in the different activities and with competency regarding health and disability design the programmes and advise each individual. BHC is one of the few places in Norway where people can try out technical equipment meant for activity and sports. Part of the philosophy of the rehabilitation programme at BHC is to ensure a prolonged effect and continued physical activity after discharge. The topic “Continuation of follow-up in the local environment” is taught in groups and addressed during individual interviews towards the end of the stay. Specific agreements and plans for the chosen continuation are made. The doctor responsible for the patient in the community receives a medical summary, and the patient is given an extensive activity report and a plan for further contact in his local community.
The programme is intensive, with 4–5 h of physical activity a day, 6 days a week. Variation in activities is emphasized. The structure of the programme over the 4 weeks is shown in Table II. To some extent the programme reflects the Norwegian activity culture, with great focus on outdoor activities. Most of the activities are arranged in groups. The group setting is considered important, with peer work and exchange of activity experiences between the patients. During the stay individual plans are constantly supervised and adjusted when necessary. Removing environmental obstructions and facilitating the performance of activities according to individual’s preferences is considered to have both mental and physical effects. Physical activity levels may be increased, but the consequences for the role function both physical and mental may be even more important. The range of activities and, compared with other rehabilitation programmes, often less traditional activities offered by BHC provide the opportunity to determine activities suited for the individual, and facilitate the experience of coping. Hippotherapy is an example of the implementation of such a strategy. Specially trained horses, different types of specially adapted saddles, equipment for mounting the horse and so forth are all prerequisites for this activity. On the physical level hippotherapy can influence muscle tone or inappropriate movement patterns or increase range of motion in joints. Perhaps more important is the experience of contact with an animal, the warmth and rhythmic movements from the horse. Hippotherapy may lead to a shift of focus from the patients’ body and pain to the wellbeing of, and the co-operation with, the animal and the opportunity to experience the natural world.
| Table II. The Beitostølen Healthsports Centre programme with examples of the activities |
| Arrival week | Second week | Third week | Departure week |
| Interviews | Basic activities | Basic activities | Basic activities |
| Information | Goal-oriented activities | Goal-oriented activities | Goal-oriented activities Individual activities |
| Testing |
| Goal-setting | Individual activities | Individual activities | Conversation group |
| Basic activities | Conversation group | Conversation group | Re-test |
| Introduction activities | Goal evaluation | Goal evaluation | Departure interview |
| Conversation group | Group education | Group education | Evaluation |
| Basic activities: group activities in pool and gymnastics. Individual activities: horse-riding, canoeing, kayaking rowing, cross-country skiing, alpine skiing, cycling, walking, archery, wall-climbing, physiotherapy. |
An example of adaptation of the programme according to medical condition and functioning is that of a 45-year-old man diagnosed with ankylosing spondylitis 20 years previously. He had been exercising regularly, but he experienced times when he found it difficult to remain motivated to stay both active and employed. After admission he was assigned a programme where his days began in the swimming pool alone or in a group. The swimming pool was heated to 32°C, which reduced his pain and stiffness. In order to increase aerobic capacity he was introduced to hiking with ski poles (Nordic walking), as running and cycling proved uncomfortable. One of his difficulties was the rotation and lateral flexion of his spine, so his work-outs focused on maintaining and improving his range of motion in that area in the individual physiotherapy sessions. This movement was also facilitated by horse-riding and kayak paddling. In both activities he was part of a group as well as experiencing the natural world. Focusing on his daily activities made him forget his pain and stiffness for periods of time. In addition to the physical training, he spent a lot of time enjoying social interaction with fellow clients in his free time and during meals. He participated in various leisure activities with others, had plenty of time to rest and reflect, and an opportunity to pay greater attention to himself for a few weeks without other responsibilities. He improved physically according to the tests, but most important to him was that he was returning home with more motivation, many new experiences, and had acquired 2 new outdoor activities, paddling and Nordic walking, which he could also do with his family. He felt very satisfied because he had re-gained his enthusiasm for physical activity.
Measurements
The SF-12 was completed by the subjects within the first 2 days of the start of the stay, and again on the last day. Three months after discharge, the SF-12 form was sent to the subjects by post.
SF-12 has been shown to contain almost 90% of the variance in SF-36, and to reflect the same 8 dimensions (17, 18). SF-12 is far less time-consuming than SF-36. It was regarded by the subjects as easier to complete and was chosen in order to increase the response rate after discharge. Only the first version (SF-12 Norwegian Standard version 1.1, SF-12 Health surveys), which was used for the 1996 Health Status Survey, is translated into Norwegian. There are minor differences in terms of wording and scoring between the first and second versions; however they are summed and weighted so as to be comparable with each other. The answers were given on a Likert scale with scoring levels from 2 to 6 according to the various questions. The Physical and Mental Component (PCS and MCS) norm-based scores for SF-12 were calculated using the reversed scores of questions 1, 8, 9 and 10 (18). SF-12 contains 8 subscales: physical function, role physical, bodily pain, general health, vitality, social function, role emotional and mental health. The norm-based factor scores for these 8 subscales were aggregated using the reversed scores of questions 1, 8, 9 and 10 for calculation of each subscale.
Due to differences in medical diagnosis and functioning, meaningful measurements of physical function were difficult to obtain. The Bath Ankylosing Spondylitis Metrology Index (BASMI) (19) consists of 5 tests measuring active range of motion in the different parts of the spine and hips. BASMI was applied at arrival and departure for the patients with ankylosing spondylitis (n = 22). It is scored as a sum score of the 5 functions, ranging from 0 (mildly affected) to 10 (severely affected). Several of the other subjects with musculoskeletal disorders were evaluated using walking tests (n = 15). The subjects were asked to walk as fast as possible back and forth on a 20-m long track for 3 min, and the distance covered in metres was measured (20). The subjects were categorized as married/cohabiting or other civilian status, living in rural or urban areas, and employed (including students and part-time work) and on sick-leave/pensioned.
Statistics
Normal distributed data are presented as mean and standard deviation (SD), skewed data are presented with median and interquartile range (IQR). Differences between the demographic and diagnostic factors between subjects invited and not completing SF-12 (n = 56), and the subjects completing at admission were investigated by χ2 test and independent sample t-tests and Mann-Whitney U tests. These differences were also investigated between subjects completing SF-12 at admission compared with subjects completing both at admission and departure, and subjects not completing compared with those completing 3 months follow-up.
The SF-12 PCS and MCS were compared with a Swedish reference population (n = 7734) (18) using the mean and SD of the populations. Paired samples t-tests were used to compare the same subjects on admission, departure and at 3 months follow-up. Independent sample t-tests were used to compare the subjects only completing SF-12 at admission, with the subjects completing both at admission and departure, as well as the subjects not completing compared with those completing SF-12 at 3 months follow-up.
Effect sizes or Z-scores were calculated as the variables mean change divided by the SD for the reference population. Subjects with musculoskeletal diseases (n = 70) were compared with subjects with other diagnoses (n = 158) for the different measurements by independent samples t-tests and Mann-Whitney U tests. The factors influencing improvement during rehabilitation were explored in a stepwise backward multiple regression model, with the sum score of the PCS, the subscale of Role Physical Function and the sum score of the MCS as the dependent variables. Age, gender, length of disease, employment status, cohabitant status, urban/rural settlement and painful musculoskeletal diagnosis were included as predictor variables. Associations between PCS and MCS at admission and changes during the rehabilitation were analysed by Pearson (r) correlation analysis. Subjects not showing any improvement in PCS or MCS, respectively, from admission to discharge were compared with subjects improving with respect to demographic factors and PCS and MCS level at admission by χ2 analysis, independent sample t-tests and Mann-Whitney U tests. Paired t-test comparisons of admission and departure results of BASMI and walking test distance were performed.
The comparison of SF-12 with the Swedish reference population was made using the NCSS 2004 (Kaysville, Utah, USA). All other statistical analyses were performed by SPSS version 14.0. A significance level of 0.05 was chosen.
Results
Physical and mental functioning on admission
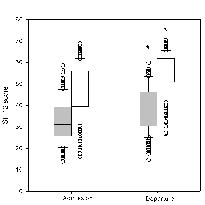
The subjects in this analysis had significantly reduced physical (32.7) and mental (47.5) functioning on admission to BHC compared with the Swedish reference population (mean score 50.2 and 52.8 PCS and MCS, respectively, in the reference population) (p < 0.001). More problems were observed for physical, compared with mental, functioning as evaluated by the sum scores on admission (p < 0.001) (Fig. 1). Subjects with musculoskeletal disorders reported significantly lower physical functioning compared with subjects with other diagnoses (p = 0.04). There were no statistical differences between the diagnostic groups with respect to mental functioning (p = 0.11). No statistically significant differences in physical or mental functioning were observed between subjects being married/cohabitant and other civilian status (p > 0.08); however, the physical functioning scores were slightly lower in the married group. Living in urban areas was related to higher physical functioning compared with subjects living in rural areas (p = 0.013). Employed subjects also reported higher physical functioning compared with the non-working group (p = 0.007), whereas the difference in mental level did not reach statistical significance (p = 0.09). The duration of the disease did not influence physical or mental functioning in the present population (p < 0.18). Furthermore, there were no associations between employment status and urban/rural living (r = 0.04, p = 0.60).
Fig. 1. Physical (grey) and mental (white) scores of SF-12 on admission to and departure from Beitostølen Healthsports Centre ((n = 228). Median, 25th and 75th percentiles (box), 10th and 90th percentiles (error bars) and outliers (circles) are shown. *Changes from admission to departure (p < 0.001).
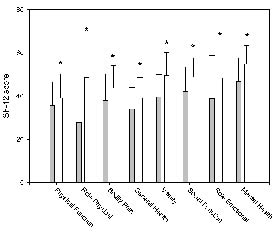
When SF-12 was broken down into its 8 subscales, role physical function and general health appeared to be the domains with the largest limitations, and mental health the domain with least limitations (Fig. 2). As expected, subjects with musculoskeletal disorders reported significantly more problems with bodily pain than subjects with other diagnoses (p < 0.001). However, lower general health, vitality, social function and mental health were also reported by subjects with musculoskeletal disorders (p <0.03).
Fig. 2. Mean values for the subscales of SF-12 on admission to (grey bars) and departure from (white bars) Beitostølen Healthsports Centre for all participating subjects (n = 228). *Changes from admission to departure (p < 0.001).
Factors influencing changes in physical and mental functioning during rehabilitation
Both physical and mental functioning improved significantly (p < 0.001) (mean score improvement 5.26 (SD 7.45) and 8.17 (SD 9.63), respectively) (Fig. 1). However, physical function remained more than 20% below the level of the reference population (p < 0.001).
All the subscales also improved significantly (p < 0.001), but the most marked improvement was observed for role physical function (Fig. 2). The effect sizes ranged from 0.32 for physical function to 1.6 for role physical function.
No relationship between improvement in physical and mental functioning was found (r = –0.11, p = 0.12). Only 9% of the subjects did not improve at all during the rehabilitation. Improvement in physical function was associated with lower levels of physical functioning on admission (r = 0.33, p < 0.001). The 45 subjects not improving in physical function also had lower mental function at admission compared with the subjects improving (p = 0.03). Twenty percent of subjects did not improve their mental functioning during the rehabilitation period, and this was associated with higher level of mental functioning on admission (r = 0.64, p < 0.001). Painful musculoskeletal conditions were also more infrequent in this group (p = 0.04) (Table IV).
| Table IV. Non-responders with respect to physical and mental improvement during the Beitostølen Healthsports Centre rehabilitation programme. Number of subjects with SF-12 physical and mental component (PCS and MCS) changes from admission to departure ≤0 |
| | Non-responders PCS n = 45 | Non-responders MCS n = 56 |
| Age (years), mena (SD) | 49 (13) | 47 (12) |
| Gender (% males) | 48 | 55 |
| Duration of disease (years), mean (IQR) | 10 (2) | 8 (1) |
| Musculoskeletal diseases (%) | 30 | 21 |
| Rural settlement (%) | 45 | 36 |
| Married/cohabiting (%) | 57 | 66 |
| Disability pensioned (%) | 67 | 68 |
| PCS, mean (SD) | 34 (12) | 32 (11) |
| MCS, mean (SD) | 43 (13) | 57 (11) |
| SD: standard deviation; IQR: interquartile range. |
The multiple backward regressions indicated that the improvement in the sum score of physical functioning and subscale of role physical function was explained by living in urban areas and having a painful musculoskeletal diagnosis. The improvement in mental functioning was explained by female gender (Table III) , whereas age did not influence improvement in mental or physical function (regression coefficient (B) < 0.02, p > 0.61).
| Table III. Regression coefficient (B) with 95% confidence interval (CI), given for the final predictors in the multiple regression models with the sum score of the Physical Component (PCS), the subscale of Role Physical Function (RP) and the sum score of the Mental Component (MCS) as the dependent variables. Age, gender, length of disease, employment status, cohabitant status, urban/rural settlement and painful musculoskeletal diagnosis were included as predictor variables. Final prediction models presented |
| | B unadjusted | CI for B lower, upper | p-values |
| PCS Urban settlement Musculoskeletal diagnosis | –1.07 –2.95 | –2.32, 0.18 –5.59, –0.30 | 0.092 0.029 |
| RP Urban settlement Musculoskeletal diagnosis | –2.41 –4.69 | –4.69, –0.13 –9.55, 0.17 | 0.039 0.058 |
| MCS Gender | 3.29 | 0.06, 6.52 | 0.046 |
The BASMI score declined from 3.09 to 1.64 (p < 0.001) for the 22 patients with ankylosing spondylitis. A significant improvement in the walking test, from a mean of 226 (SD 63) to 251 (SD 65) m, for 15 other musculoskeletal patients was also observed (p = 0.02).
Physical and mental functioning 3 months after discharge
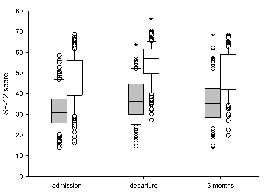
No deterioration was found for physical functioning in subjects with musculoskeletal disorders from departure to 3 months (p = 0.46). Otherwise, physical and mental functioning declined from departure to 3 months follow-up (n = 174, p = 0.04 and p < 0.001, respectively) (Fig. 3), but remained above the level at admission (p < 0.001).
Fig. 3. Physical (grey) and mental (white) scores of SF-12 on admission to, departure from, and 3 months after departure from Beitostølen Healthsports Centre (n = 174). Median, 25th and 75th percentiles (box), 10th and 90th percentiles (error bars) and outliers (circles) given. Physical and mental score on departure and physical score at 3 months are significantly higher compared with admission (*p < 0.001).
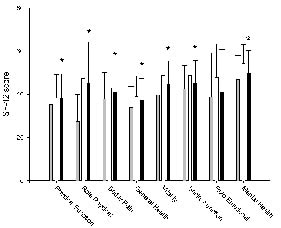
The subscale of physical function indicated that the improvement during the rehabilitation was maintained at the 3 months follow-up (p = 0.94 for comparison of departure and 3 months follow-up) (Fig. 4). Only a slight decline in the role physical dimension was found (p = 0.07). The other 6 subscales indicated deteriorating function from departure to 3 months follow-up (p < 0.04). In summary, except for role emotional function (p = 0.14), all other subscales remained improved at 3 months follow-up compared with the admission scores (p < 0.002) (Fig. 4).
Fig. 4. Mean values for the subscales of SF-12 on admission to (grey bars), departure from (white bars) Beitostølen Healthsports Centre and at 3 months follow-up (black bars) (n = 174). *Significant improvement at 3 months follow-up compared with admission (p < 0.05).
The influence of drop-out
The subjects invited but not completing any SF-12 (n = 56) were significantly younger (p < 0.001) than the 257 subjects completing SF-12 at admission. The subjects completing SF-12 only at admission (n = 29) were also younger than the subjects completing SF-12 at both admission and departure (p < 0.001). Otherwise there were no differences in demographic factors between the drop-outs after invitation, between admission and departure and between departure and 3 months and the attendants (p > 0.45). No differences in physical or mental functioning were found between the subjects completing SF-12 at admission compared with both at admission and at departure (p > 0.49) and the groups completing and not completing the forms at 3 months (p > 0.45) (Table I).
Discussion
SF-12 is an instrument used worldwide to assess health-related quality of life. SF-12 reflects 90% of the variance in the far more extensive form, SF-36 (17). A Norwegian reference population for SF-12 has not been established. In most aspects, the health status is similar in the neighbouring countries of Norway and Sweden; hence a Swedish reference population was chosen (18). In addition, the differences across countries in physical and mental health in the general population are relatively small (18). Hence, it is suggested that the differences found between the present subjects and the reference population reflects a real reduction in physical and mental health in the subjects admitted to BHC. The changes in physical and mental health during rehabilitation, as well as the changes in the 8 subscales, would remain significant if we applied a significance level of 0.005 according to a Bonferroni correction corresponding to 10 tests (21).
No pressure was put on the subjects to complete the SF-12 forms, which may explain the drop-out rate. With respect to demographic variables, medical diagnosis and length of the disease, the drop-out rates were comparable with the study population. Physical and mental functioning was also similar in the subjects completing SF-12 only at admission and the subjects completing SF-12 also at departure and at 3 months follow-up.
Mental functioning, as evaluated by SF-12, was less reduced than physical functioning in the present population. First, subjects with mental illnesses as their main diagnosis were excluded. However, one would expect the disabilities to influence mental functioning (10). BHC and its rehabilitation concept are well-known in Norway among disabled persons and health workers. The BHC’s surroundings and opportunities for participating in physical activities may bias the referral practice, with mainly subjects with physical disabilities being admitted. However, more representative patient populations, for example with arthritis and various neurological conditions, also report greater problems with physical than with mental functioning (22). In some studies, normal mental functioning is reported in subjects with chronic physical impairments (23).
For the present subjects, the role physical function was particularly low. This is important as physical functioning itself is determined mainly by the disorder. However, role physical function is also influenced by expectations, support and environmental factors. Hence, improvement in this dimension may be possible even in the presence of considerable physical disability. The rehabilitation perspective at BHC focuses on participation in activities, in order to increase muscular function and improve endurance as well as facilitate coping. This resulted in overall improvement in both physical and mental functioning comprising all 8 dimensions of SF-12. However, the improvement in role physical function was particularly large. People with disabilities are liable to encounter problems with identity, especially in the western world with its increased focus on body appearance and movement (24). Thus, it can be valuable to experience a new role as an active participant in society. Small changes in physical functioning accompanied by large improvements in role physical function are also documented in other rehabilitation approaches (25). For the subgroups tested, the programme also improved physical functioning as measured by more standardized observation methods.
The improvement in physical and mental functioning was not influenced by the same factors. Women improved more than men with respect to mental functioning. Women often spontaneously reported respite from the traditional housewife role during their stay at the centre. They also seem to have somewhat different expectations regarding the level of physical functioning they might be able to achieve. Similar conclusions were also reached in a previous study at BHC (26).
Long duration of disease and functional problems are generally negative prognostic factors in rehabilitation (27, 28). However, the duration of the problems did not influence the improvement in the present study. We believe this may be related to the selection of subjects as well as the setting in which the rehabilitation takes place. Persons with long-standing, severe disabilities are met with a main focus on what they can do, in order to enhance self-efficacy and self-respect. Age, employment or civilian status, were not predictors of rehabilitation outcome. Hence, the pattern of success in this rehabilitation is different from multidisciplinary rehabilitation in a hospital setting (29). In general, the effect in the present study was also attained across different diagnostic groups. Thus, the benefits of focusing on motivation, self-esteem and reducing distress may be of general importance to the effect of rehabilitation (30).
The subjects with musculoskeletal conditions, including rheumatic diseases, reported considerably higher pain levels than subjects with other diagnostic entities. In addition, subjects with musculoskeletal conditions reported lower physical functioning. The pain may influence all aspects of health and well-being (31). However, a marked problem with physical functioning is the hallmark of musculoskeletal pain (32). On the other hand, subjects with painful musculoskeletal disorders living in urban areas seemed to gain most from the rehabilitation strategies at BHC with respect to physical functioning and role physical function. The experience of coping and participation in activities as well as the social setting may lead to a shift of focus from the patients’ pain to pleasure in taking part in life. We can only speculate in the reasons for subjects from urban areas benefiting more than subjects from rural areas. Different selection of subjects may be involved, and educational level, which was not recorded in the present study, may influence this result.
Interestingly, significantly lower mental functioning at admission was related to lack of improvement in physical functioning. This was also found in a study by Lillefjell et al. (33), where emotional distress was a negative predictor for improvement in a multidisciplinary rehabilitation programme. Hence, across settings, one may focus on the mental resources. As mastery and self-esteem are important protective factors in mental health (34), improving coping through the rehabilitation at BHC may be of great importance. None responders had generally no possibility to improve mental functioning because of high function at admission. Except for slightly lower age the non-attendants were similar to the participants with respect to other demographic factors and mental and physical functioning.
One important goal of the rehabilitation was to facilitate increased participation in society when the subjects returned to their home environment, assuming that this would imply sustained mental and physical improvement. However, mental functioning declined from departure until follow-up at 3 months, which could indicate a “holiday effect” of the stay at BHC on this dimension. In contrast, the improvement in physical functioning and role physical function was to a large extent maintained at 3 months. To acquire skills in sports activities during the stay at BHC may facilitate participation in activities of daily life as well as sports activities in the community, thus contributing to maintaining physical functioning and physical role function.
The APA is more of a philosophy than a strictly defined rehabilitation strategy (35). It was developed in the education system in contrast to most multidisciplinary rehabilitation programmes evolving from a hospital setting. Skilled professionals supervise subjects in the activities, whereas the instructors are often health professionals in multidisciplinary rehabilitation programmes. A hospital setting represents a restricted environment, whereas the concept of BHC is to facilitate the use of the natural environment indoors, outdoors and across seasons. To investigate the effect of this approach in comparison with traditional rehabilitation in a randomized fashion, without bias due to patient selection is a challenge.
In conclusion, the population admitted to BHC has reduced physical and mental functioning, with problems in the area of role physical function in particular. A significant improvement in both physical and mental functioning was obtained during rehabilitation. The largest improvement was for role physical function. The improvement was best maintained in the physical function domains at the 3 months follow-up. Controlled studies with longer follow-up periods are required.
ACKNOWLEDGEMENTS
We thank Astrid Nyquist, Ine Wigernes and Martin Sebu for valuable discussion, Susan Schanke for proficient language help and BHC for financing the present study.
REFERENCES
1. Bautz-Holter E, editor. Bevegelseshemmet i Sogn og Fjordane [Individuals with disabilities in the country of Sogn og Fjorne] Oslo: Faculty of Medicine, University of Oslo; 1986 (in Norwegian).
2. de Ridder D, Schreurs K. Developing interventions for chronically ill patients: is coping a helpful concept? Clin Psychol Rev 2001; 21: 205–240.
3. Ehde DM, Jensen MP, Engel JM, Turner JA, Hoffman AJ, Cardenas DD. Chronic pain secondary to disability: a review. Clin J Pain 2003; 19: 3–17.
4. Stewart AL, Hays RD, Wells KB, Rogers WH, Spritzer KL, Greenfield S. Long-term functioning and well-being outcomes associated with physical activity and exercise in patients with chronic conditions in the Medical Outcomes Study. J Clin Epidemiol 1994; 47: 719–730.
5. LaMonte MJ, Durstine JL, Addy CL, Irwin ML, Ainsworth BE. Physical activity, physical fitness, and Framingham 10-year risk score: the cross-cultural activity participation study. J Cardiopulm Rehabil 2001; 21: 63–70.
6. Gabriel DA, Kamen G, Frost G. Neural adaptations to resistive exercise: mechanisms and recommendations for training practices. Sports Med 2006; 36: 133–149.
7. Berlin AA, Kop WJ, Deuster PA. Depressive mood symptoms and fatigue after exercise withdrawal: the potential role of decreased fitness. Psychosom Med 2006; 68: 224–230.
8. Kujala UM. Evidence for exercise therapy in the treatment of chronic disease based on at least three randomized controlled trials – summary of published systematic reviews. Scand J Med Sci Sports 2004; 14: 339–345.
9. Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 2006; 16 Suppl 1: 3–63.
10. Verbrugge LM, Jette AM. The disablement process. Soc Sci Med 1994; 38: 1–14.
11. Giske L, Stanghelle J, Rand-Hendrikssen, Strøm V, Wilhelmsen J-E, Røe C. Pulmonary function, working capacity and strength in young adults with Marfan syndrome. J Rehabil Med 2003; 35: 221–228.
12. Simon C, Wagner A, Platat C, Arveiler D, Schweitzer B, Schlienger JL, et al. ICAPS: a multilevel program to improve physical activity in adolescents. Diabetes Metab 2006; 32: 41–49.
13. Keysor JJ. Does late-life physical activity or exercise prevent or minimize disablement? A critical review of the scientific evidence. Am J Prev Med 2003; 25 Suppl 2: 129–136.
14. Sherill C, editor. Adapted physical activity. Recreation and sport: crossdisciplinary and lifespan. Boston: MA: WCB McGraw-Hill; 2004.
15. Sherill C. What is adapted physical activity? In: Sherril C, editor. Adapted physical education and recreation: a multidisciplinary approach. Dubuque: Wm. C. Brown; 1976, p. 3–11.
16. Sherill C, editor. Quality of life through adapted physical activity and sport-a lifespan concept. Proceedings of the 10th ISAPA. Oslo & Beitostølen: ISAPA Organizers; 1995, p. 32–44.
17. Ware J, Jr., Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34: 220–233.
18. Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: results from the IQOLA Project. International Quality of Life Assessment. J Clin Epidemiol 1998; 51: 1171–1178.
19. Jenkinson TR, Mallorie PA, Whitelock HC, Kennedy LG, Garrett SL, Calin A. Defining spinal mobility in ankylosing spondylitis (AS). The Bath AS Metrology Index. J Rheumatol 1994; 21: 1694–1698.
20. Harding VR, Williams AC, Richardson PH, Nicholas MK, Jackson JL, Richardson IH, et al. The development of a battery of measures for assessing physical functioning of chronic pain patients. Pain 1994; 58: 367–375.
21. Bland JM, Altman DG. Multiple significance tests: the Bonferroni method. Br Med J 1995; 310: 170.
22. Turan Y, Duruoz MT, Cerrahoglu L. Quality of life in patients with ankylosing spondylitis: a pilot study. Rheumatol Int 2007; 10: 895–899.
23. Kelly MH, Brillante B, Kushner H, Gehron RP, Collins MT. Physical function is impaired but quality of life preserved in patients with fibrous dysplasia of bone. Bone 2005; 37: 388–394.
24. Brown JD, Siegel JM. Exercise as a buffer of life stress: a prospective study of adolescent health. Health Psychol 1988; 7: 341–353.
25. Fletcher A. Quality-of-life measurements in the evaluation of treatment: proposed guidelines. Br J Clin Pharmacol 1995; 39: 217–222.
26. Blaasvaer S, Stanghelle JK. Rehabiliteringsopphold med tilpasset fysisk aktivitet - hva skjer med pasientenes livskvalitet? [Rehabilitation with proper physical activities – what happens with patients’ quality of life?]. Tidsskr Nor Laegeforen 1999 10; 119: 1281–1286.
27. Kennedy CA, Manno M, Hogg-Johnson S, Haines T, Hurley L, McKenzie D, et al. Prognosis in soft tissue disorders of the shoulder: predicting both change in disability and level of disability after treatment. Phys Ther 2006; 86: 1013–1032.
28. Heikkila H, Heikkila E, Eisemann M. Predictive factors for the outcome of a multidisciplinary pain rehabilitation programme on sick-leave and life satisfaction in patients with whiplash trauma and other myofascial pain: a follow-up study. Clin Rehabil 1998; 12: 487–496.
29. Gross DP, Battie MC. Predicting timely recovery and recurrence following multidisciplinary rehabilitation in patients with compensated low back pain. Spine 2005; 30: 235–240.
30. Hays RD, Eastwood JA, Kotlerman J, Spritzer KL, Ettner SL, Cowan M. Health-related quality of life and patient reports about care outcomes in a multidisciplinary hospital intervention. Ann Behav Med 2006; 31: 173–178.
31. Penny KI, Purves AM, Smith BH, Chambers WA, Smith WC. Relationship between the chronic pain grade and measures of physical, social and psychological well-being. Pain 1999; 79: 275–279.
32. Gross DP. Are functional capacity evaluations affected by the patient’s pain? Curr Pain Headache Rep 2006; 10: 107–113.
33. Lillefjell M, Krokstad S, Espnes GA. Prediction of function in daily life following multidisciplinary rehabilitation for individuals with chronic musculoskeletal pain; a prospective study. BMC Musculoskelet Disord 2007; 8: 65.
34. Bovier PA, Chamot E, Perneger TV. Perceived stress, internal resources, and social support as determinants of mental health among young adults. Qual Life Res 2004; 13: 161–170.
35. Hutzler Y, Sherrill C. Defining adapted physical activity: international perspectives. Adapt Phys Activ Q 2007; 24: 1–20.