OBJECTIVE: To determine variables among glenohumeral elevation and 3-dimensional scapular rotations that are related to shoulder function as assessed by the Disability of the Arm, Shoulder and Hand-Disability/Symptom (DASH-D/S) scale.
DESIGN: Prospective, cross-sectional study.
Patients: Eighty-eight patients with shoulder pain and limited range of motion were included.
METHODS: Each patient performed 2 full active range of motion activities, forward flexion and abduction, and 2 activities of daily living, combing hair and simulating washing the back. Glenohumeral elevation and scapular rotations were measured by the Polhemus Fastrak electromagnetic system.
RESULTS: On multiple regression analysis, glenohumeral elevation in combing hair and scapular lateral rotation in both abduction and simulating washing the back were the best predictors of shoulder function and explained 39.7% of the variance of the DASH-D/S score.
CONCLUSION: These findings support the classical rehabilitation of the shoulder based on glenohumeral elevation and suggest the importance of attention paid to scapular lateral rotation.
Key words: shoulder, kinematics, disability, rehabilitation, range of motion.
J Rehabil Med 2008; 40: 456–460
Correspondence address: Fouad Fayad, Department of Physical Medicine and Rehabilitation, Cochin Hospital, 27 Rue du Faubourg Saint Jacques, 75679 Paris Cedex 14, France. E-mail: fouadfayad@yahoo.fr
Submitted July 31, 2007; accepted February 5, 2008
INTRODUCTION
Shoulder disorders are the third most common musculoskeletal reason for consulting a doctor (1). Their prevalence varies between 21% and 34% in community surveys (2–4). Disability related to the shoulder was found in 30% of healthy subjects over the age of 65 years and was significantly associated with reduced movement (3).
Several disorders of the shoulder with different mechanisms of stiffness could be responsible for limited glenohumeral (GH) motion and consequent disability. Previous studies showed global shoulder range of motion (ROM) significantly correlated with function (5, 6). In particular, forward flexion, abduction, internal rotation and external rotation have moderate to good correlation with various upper extremity activities such as combing hair and washing the back (5, 6).
The global shoulder ROM is the result of multiple joint movements of the shoulder girdle, particularly of the scapulothoracic and GH joints, which must be coordinated to perform full ROM. Rundquist & Ludewig (7) studied the relation between GH motion and function in 21 patients with idiopathic loss of shoulder ROM. Multiple regression analysis revealed that scapular-plane abduction, external rotation at the side, external rotation at 90° of abduction, and patient weight were significantly correlated with shoulder function and explained 69% of the variation in score on the Shoulder Rating Questionnaire (7). Lin et al. (8) evaluated the relation between scapular movement and function in a sample of 25 patients with shoulder pain and limited ROM and found 3-dimensional (3-D) scapular kinematics correlated significantly with function, as measured by the Self-Report Flexivel Scale of Shoulder Function.
Medical and, especially, rehabilitation treatments are used for managing GH stiffness in patients with shoulder disorders (9, 10). Because of the interrelations between scapular and GH joint motions, a more complete understanding of the relation of GH motion and 3-D scapular kinematics with shoulder function could help improve physical and rehabilitation treatment of these patients.
We aimed to analyse the relationship of variables among GH elevation and 3-D scapular rotations with shoulder function as assessed by the Disability of the Arm, Shoulder and Hand-Disability/Symptom (DASH-D/S) questionnaire.
MethodS
Patients
Eighty-eight patients with shoulder pain and limited ROM consecutively referred to a tertiary care rehabilitation centre participated in the study. Limited ROM is defined as forward flexion and/or abduction less than 160°. Patients included had the following 4 common shoulder disorders: primary or secondary frozen shoulder (n = 25), proximal humeral fractures (n = 24), rotator cuff tendinopathies (n = 20), and GH osteoarthritis (n = 19). The diagnosis was confirmed by an experienced senior physician at our institution. Frozen shoulder was defined as a pattern of limited joint mobility in external rotation, abduction, and forward flexion (passive and active range of motion < 50% of the unaffected side) with normal plain X-ray results (11). Patients with proximal humeral fracture were seen after bone healing confirmed on plain X-ray. Rotator cuff tendinopathies were confirmed by ultrasound and/or magnetic resonance imagining (MRI) of the shoulder, and GH osteoarthritis was diagnosed on the basis of plain X-ray results, showing at least a narrowing of the GH space with or without osteophytes on the humeral head. Patients with cervical radiculopathy, a history of cervico-thoracic outlet compression syndrome and rheumatic disease were excluded.
Parameters recorded for each patient were age, sex, disease duration, body mass index, pain scores at rest and during activities on a visual analogue scale (VAS, 0–100 mm), and patient-perceived handicap on a VAS. The French version of the DASH-D/S (F-DASH-D/S) was used to assess shoulder disability (12). This 30-item scale was validated for patients with shoulder disorders and has good reliability and construct validity (13). The items ask about the degree of difficulty in performing various physical activities because of an arm, shoulder or hand problem; the severity of each of the symptoms of pain, activity-related pain, tingling, weakness and stiffness; and the problem’s effect on social activities, work, and sleep and its psychological impact. Each item in the scale has 5 response options, ranging from 1, “no difficulty or no symptom,” to 5, “unable to perform activity or very severe symptoms.” All patients provided informed consent, and the study protocol was approved by the local Institutional Review Board.
Instrumentation
We used an electromagnetic tracking device, the Polhemus Fastrak (SPACE FASTRAK, Colchester, VT, USA), for recording kinematic data. Real-time 3-D position and orientation of the thorax, scapula and humerus were tracked at 30 Hz. The Polhemus Fastrak consists of a transmitter and 4 receivers/sensors, all hardwired to the system’s electronic unit. The transmitter generates a low-frequency electromagnetic field that is detected by the sensors. The system’s electronic unit determines the relative orientation and position of the sensors, and data were stored on a computer. The reported root mean square (RMS) accuracy of this system is 0.3–0.8 mm for position and 0.15° for orientation when used within a 76-cm source to sensor separation (SPACE FASTRAK User’s Manuel, Revision F. Colchester, VT, USA; Polhemus Inc.; 1993).
Experimental procedure
Kinematics. The transmitter was fitted on a rigid plastic frame 30 cm in front of the subject and established the global coordinate system (GCS). The thorax sensor was adhered to the subject’s skin overlying the sternum, and the scapula sensor was fixed on the flat surface of the superior acromion process with double-sided adhesive tape secured with 2 strips of Transpore. The humeral sensor was attached to a thermoplastic cuff Velcro strapped to the lateral arm just below the insertion of the deltoid. Validation studies of 3-D scapular kinematics comparing skin sensors to acromion-fixed sensors demonstrated that the average motion pattern of surface method was similar to that measured by the invasive technique, especially below 120 degrees of elevation (14). Only the study of Karduna et al. (14) assessed the validity of the skin sensor method by comparison with data collected simultaneously by an invasive approach in which pins were drilled directly into the scapula. For humeral motion, previous validity data compared with that from an external bone fixator found less than 4° RMS error for all motions except for long-axis rotation (15).
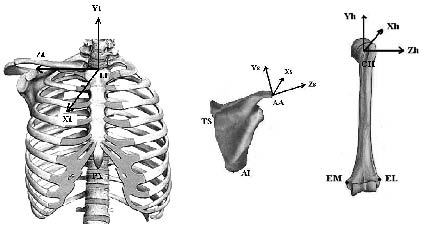
The fourth sensor mounted on a pointer manually digitized anatomic landmarks. Nine bony landmarks on the thorax, humerus and scapula were palpated and digitized to allow transformation of the sensor data from the GCS to anatomically based local coordinate systems (LCSs) (Fig. 1). From the combination of LCSs constructed from these anatomical landmarks and the sensor motions, both segment and, subsequently, joint rotations could be calculated (18). LCSs and segment and joint rotations were defined according to the International Society of Biomechanics standardization proposal for the upper extremity (19).
Fig. 1. Local coordinate systems (LCSs) of the thorax, scapula and humerus defined with bony landmarks. The LCS of the thorax was defined with the processus xiphoideus (PX), incisura jugularis (IJ), and processus spinosis of the 7th cervical vertebra and the 8th dorsal vertebra; the LCS of the scapula with the angulus acromialis (AA), trigonum spinae (TS), and angulus inferior (AI); and the LCS of the humerus with the medial epicondylus (EM), lateral epicondylus (EL) and the glenohumeral rotation (GH) centre. The GH rotation centre was estimated with a least squares algorithm and defined as the point that moved the least during several passive circumduction movements (16, 17).
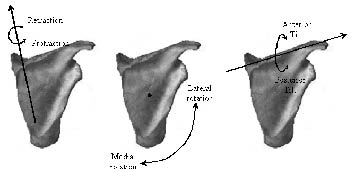
Definition of segment orientation. The LCSs developed for the thorax, scapula and humerus were used to describe clinically relevant shoulder motions (20). The standardized sequence of Euler angles proposed by Wu et al. (19) was chosen. Scapular orientation with respect to the thorax was described by the YX’Z’’ Euler sequence. Protraction/retraction (or internal/external rotation) was around the thoracic Y axis, followed by lateral/medial (upward/downward) rotation around the scapula X’ axis (perpendicular to the scapular plane, pointing forward), followed by anterior/posterior tilt around the scapular Z’’ axis through the scapular spine (Fig. 2). Humeral orientation relative to the scapula was described with the YX’Y’’ sequence, including the plane of elevation with respect to the scapula Y axis, humeral elevation/depression around the local X’ axis, and axial rotation around the local Y’’ axis (Fig. 1). For simplicity, the rotations of the left side were transformed by appropriate geometrical calculation for projection on the right side.
Fig. 2. The scapular rotations.
Movement analysis. Following the digitization process, kinematic data were collected at 30 Hz during trials of 2 full active ROM activities, forward flexion and abduction, and 2 activities of daily living, combing hair and simulating washing the back. For these trials, subjects were standing upright with both arms hanging beside the body (in a resting position). Each subject performed 2 repetitions of each movement. Subjects were asked to reach the resting position after each trial and to avoid moving the trunk during data recording. Visual landmarks and oral instructions were used during the experimental procedure, but no mechanical constraints were established so as to preserve spontaneous physiological organization of motion.
Statistics
Data analysis involved use of SYSTAT 9 Delta Soft for Windows (Systat Software, Inc., Point Richmond, CA, USA). Demographic and clinical characteristics were described with means and standard deviation (SD). The variables of interest were the values of GH elevation and scapular protraction/retraction, lateral/medial rotation, and anterior/posterior tilt obtained for each subject at the peak ROM of each task. The reliability in values between the 2 repetitions of each movement performed by each subject was assessed by use of intraclass correlation coefficients (ICCs).
Pearson product moment correlations (r) were used to assess the correlation between 2 quantitative variables. Several multiple regressions analysis were used to explain the variation in the total F-DASH-D/S score (explained variable) with the following quantitative explanatory variables: GH elevation in the 2 active ROM and the 2 activities of daily living, scapular lateral rotation in the 2 active ROM activities, scapular protraction and posterior tilt in abduction, and scapular lateral rotation in simulating washing the back. These variables were chosen because their correlations with the F-DASH-D/S score on bivariate analysis were > 0.20. A p < 0.05 was considered significant.
RESULTS
Demographic and clinical characteristics of patients
In total, 88 patients (64 women), mean age 58.0 years (SD 14.4), participated in the study. The mean body mass index was 24.8 (SD 4.8) and mean disease duration 24.1 months (SD 32.6). Eighty-six patients were right-dominant and only 2 patients were left-dominant. Eleven patients (12.5%) had bilateral shoulder disease (9 predominant on the right dominant shoulder). The affected shoulder distribution in patients with unilateral involvement was 46 right dominant (52.3%), one right non-dominant (1.1%), 29 left non-dominant (33.0%), and one left dominant (1.1%). Data for one patient were excluded because of more than 3 unanswered items on the F-DASH-D/S questionnaire. The mean pain score at rest and during activities was 16.5 (SD 20.7) (range 0–82) and 53.7 (SD 28.2) (range 0–100), respectively. The mean F-DASH-D/S score was 43.2 (SD 20.7) (range 5–87.5) and the mean patient-perceived handicap score was 43.9 (SD 23.8).
Movement reliability and descriptive kinematics statistics
The reliability of the 2 repetitions of each movement was excellent. ICCs for the humeral elevation and scapular rotation variables for the 4 performed tasks (2 active ROM; 2 activities of daily living) ranged from 0.95 to 0.99.
Table I gives the mean (SD) values of GH elevation and scapular protraction, lateral rotation, and posterior tilt at maximal arm elevation angles for the 4 performed tasks.
| Table I. Descriptive kinematics for glenohumeral (GH) elevation and scapular rotations at maximal arm elevation for tasks performed by patients with shoulder disabilities |
| | GH elevation (º) Mean (SD) | Scapular rotations |
| Protraction (º) Mean (SD) | Lateral rotation (º) Mean (SD) | Posterior tilt (º) Mean (SD) |
| Forward flexion | 65.7 (21.7) | 40.9 (10.9) | 41.5 (11.0) | 0.6 (11.5) |
| Abduction | 57.6 (25.4) | 34.6 (13.2) | 38.3 (12.9) | –3.8 (11.3) |
| Combing hair | 61.9 (15.6) | 31.8 (11.5) | 40.1 (9.3) | 0.8 (11.2) |
| Washing the back | 44.5 (14.3) | 34.9 (7.3) | –2.5 (7.5) | –20.4 (6.7) |
| SD: standard deviation. |
Correlations of GH elevation and scapular kinematics with F-DASH-D/S score
For forward flexion, GH elevation (r = –0.45) and scapular lateral rotation (r = –0.26) correlated best with F-DASH-D/S score (Table II). For abduction, the best correlations were with GH elevation (r = –0.55) and scapular protraction (r = –0.34), lateral rotation (r = –0.39) and posterior tilt (r = –0.23).
| Table II. Correlation of glenohumeral elevation and 3-D scapular kinematics with F–DASH-D/S score in patients with shoulder disabilities |
| | Pearson r |
| Forward flexion Glenohumeral elevation Scapular protraction Scapular lateral rotation Scapular posterior tilt | –0.45 –0.09 –0.26 –0.19 |
| Abduction Glenohumeral elevation Scapular protraction Scapular lateral rotation Scapular posterior tilt | –0.55 –0.34 –0.39 –0.23 |
| Combing hair Glenohumeral elevation Scapular protraction Scapular lateral rotation Scapular posterior tilt | –0.46 –0.01 –0.09 –0.18 |
| Washing the back Glenohumeral elevation Scapular protraction Scapular lateral rotation Scapular posterior tilt | –0.40 0.04 0.42 –0.09 |
| F-DASH-D/S: French version of the Disability of the Arm, Shoulder, and Hand-Disability/Symptom scale. Correlations higher than 0.20 in bold. |
For combing hair, the best correlations were with GH elevation (r = –0.46) and for simulating washing the back, with GH elevation (r = –0.40) and scapular lateral rotation (r = 0.42).
Multiple regression analysis
To avoid multicollinearity, a high degree of linear correlation among 2 (or more) explanatory variables, because the correlations between GH elevation in combing hair and GH elevation in both forward flexion (r = 0.86) and abduction (r = 0.86) were high, only GH elevation in combing hair was used as explanatory variable in the final multiple regression model.
In the final regression model, GH elevation in combing hair, and scapular lateral rotation in abduction and in simulating washing the back were the best predictors of shoulder function and explained 39.7% of the variance of the F-DASH-D/S score (Table III).
| Table III. Multiple regression analysis of variables explaining the variation in F-DASH-D/S score |
| Variable | Coefficient | T | p |
| Constant | 86.954 | 9.737 | < 0.001 |
| Scapular lateral rotation in abduction | –0.519 | –3.426 | 0.001 |
| Scapular lateral rotation in washing the back | 0.922 | 3.446 | 0.001 |
| Glenohumeral elevation in combing hair | –0.363 | –2.808 | 0.006 |
| Only the variables significantly related to the F-DASH-D/S score on the multiple regression analysis are represented. F-DASH-D/S: French version of the Disability of the Arm, Shoulder, and Hand-Disability/Symptom scale. |
DISCUSSION
Our results confirm the correlation of GH elevation and 3-D scapular movements with shoulder disability in patients with limited global arm elevation due to common shoulder disorders; however the correlations were relatively weak to moderate. Three kinematic variables – GH elevation in combing hair, and scapular lateral rotation in abduction and in simulating washing the back – explained 39.7% of the variance in the F-DASH-D/S score.
As far as we know, the current study is the first to evaluate simultaneously the association of both GH elevation and 3-D scapular kinematics with shoulder function. Indeed, previous studies investigated primarily the role of global or GH elevation in shoulder function (6, 7). Recently, Lin et al. (8) studied the relation between impaired scapular movements and shoulder function in a sample of 25 men with shoulder disorders and showed 3-D scapular kinematics significantly correlated with function.
Although shoulder disorders mainly affect the GH range of motion, abnormal scapulothoracic kinematics may occur (8, 21–23). Thus, we wondered whether the correlation between scapular movements and shoulder disability would be retained after the addition of GH elevation in multiple regression analysis. We found GH elevation as well as scapular lateral rotation as important kinematics parameters explaining the functional capacities of patients with shoulder disorders.
The correlation coefficients between scapular rotations and shoulder function are low, but higher correlations found between glenohumeral elevation and function was not surprising and was consistent with previous studies (7). Although the participation of the scapula in shoulder function seems to be less important than that of the glenohumeral joint, the role of the scapula appears to be interesting, probably by compensating for glenohumeral limitation in stiff shoulders (21) and optimizing the orientation of the glenoid fossa for adaptation to the required task (20, 24).
We did not find scapular protraction and tilt significantly correlated with shoulder function during forward flexion, whereas Lin et al. (8) found a weak to moderate correlation between scapular tilt and function in subjects with shoulder disorders. However, these authors analysed 4 different tasks while the subjects were sitting on a wooden chair (such as lifting and placing a bottle filled with 0.45 litres of water on the near edge of a height-adjustable desk at a constant distance from the wooden chair and at the height of the top of the subject’s head). In addition, trunk kinematics might be more restricted in a sitting than standing position, may allow less compensation for limited GH motion and, consequently, induce greater scapular compensation. During abduction, we found a weak correlation for both scapular protraction and tilt with shoulder function on bivariate analysis, but these variables were not predictive of shoulder function on multiple regression analysis.
The population of the current study is heterogeneous and includes patients with various shoulder disorders and different underlying mechanisms of stiffness. Analysing the correlation of variables among GH elevation and 3-D scapular rotations with shoulder function for each subgroup of patients would be interesting, but is beyond the scope of the current study. Indeed, we did not use a disease-specific questionnaire to evaluate the shoulder function, but we assessed the function by the DASH-D/S questionnaire independent of the underlying shoulder disease. The DASH-D/S questionnaire was developed as a region-specific instrument for measuring upper-extremity disability and symptoms, and has the best clinimetric properties among the self-administered questionnaires for shoulder disability (25). Nevertheless, additional analysis in each subgroup of patients according to pathology was performed (data not shown), and predictive kinematic variables for shoulder function in the subgroups of patients were similar to those observed in the whole population. However, the small sample size of each subgroup does not allow for generalization of these results, which need to be confirmed in future studies with a larger sample of patients for each pathology.
The results of the current study suggest that the rehabilitation of shoulder disorders with limited ROM should focus on exercises aiming to improve GH elevation in activities such as combing hair (corresponding to arm elevation in approximately a scapular plane) and scapular lateral rotation in abduction. Because the 3 kinematic variables explained only 39.7% of the variance of the F-DASH-D/S score, a full prediction of shoulder functional status requires the addition of other factors. These factors probably include muscular strength of the shoulder girdle as well as axial rotations of the humerus.
The present study has 2 limitations. First, the 4 chosen tasks did not cover the overall range of functional tasks for the shoulder. Although we analysed maximal abduction and forward flexion, as well as 2 activities included in the F-DASH-D/S questionnaire, testing other functional tasks would be interesting in future studies. Secondly, axial rotations of the humerus were not part of the explanatory variables of the self-reported shoulder function. We did not include these variables in multiple regression analysis because skin artefacts are not negligible and may reach a mean error of 7.5 degrees (15).
In conclusion, our study found 39.7% of the variance in overall shoulder function as measured by the F-DASH-D/S explained by the combination of the variables GH elevation in combing hair and scapular lateral rotation in both abduction and simulated washing the back. These findings support the classical rehabilitation of the shoulder based on GH elevation and suggest the importance of attention paid to scapular lateral rotation.
Acknowledgement
This study was supported by the Société Française de Rhumatologie (SFR), Paris, and the Association pour la Recherche en Médecine de Rééducation (ARMR), Hôpital Cochin, Paris.
We thank Y Macé, A Mayoux-Benhamou, A Roren, F Rannou, Assistance Publique-Hôpitaux de Paris, Cochin Hospital; O Gagey, Assistance Publique-Hôpitaux de Paris, Bicêtre Hospital; and the technical staff of the Department of Rehabilitation Medicine, Cochin Hospital, Paris, for their substantial contributions.
References
1. Rekola KE, Keinanen-Kiukaanniemi S, Takala J. Use of primary health services in sparsely populated country districts by patients with musculoskeletal symptoms: consultations with a physician. J Epidemiol Community Health 1993; 47: 153–157.
2. Chard MD, Hazleman R, Hazleman BL, King RH, Reiss BB. Shoulder disorders in the elderly: a community survey. Arthritis Rheum 1991; 34: 766–769.
3. Chakravarty K, Webley M. Shoulder joint movement and its relationship to disability in the elderly. J Rheumatol 1993; 20: 1359–1361.
4. Van Schaardenburg D, Van den Brande KJ, Ligthart GJ, Breedveld FC, Hazes JM. Musculoskeletal disorders and disability in persons aged 85 and over: a community survey. Ann Rheum Dis 1994; 53: 807–811.
5. Triffitt PD. The relationship between motion of the shoulder and the stated ability to perform activities of daily living. J Bone Joint Surg Am 1998; 80: 41–46.
6. Bostrom C, Harms-Ringdahl K, Nordemar R. Shoulder, elbow and wrist movement impairment – predictors of disability in female patients with rheumatoid arthritis. Scand J Rehabil Med 1997; 29: 223–232.
7. Rundquist PJ, Ludewig PM. Correlation of 3-dimensional shoulder kinematics to function in subjects with idiopathic loss of shoulder range of motion. Phys Ther 2005; 85: 636–647.
8. Lin JJ, Hanten WP, Olson SL, Roddey TS, Soto-quijano DA, Lim HK, et al. Shoulder dysfunction assessment: self-report and impaired scapular movements. Phys Ther 2006; 86: 1065–1074.
9. Kelley MJ, Ramsey ML. Osteoarthritis and traumatic arthritis of the shoulder. J Hand Ther 2000; 13: 148–162.
10. Moskowitz RW, Blaine TA. An overview of treatment options for persistent shoulder pain. Am J Orthop 2005; 34: S10–S15.
11. Dias R, Cutts S, Massoud S. Frozen shoulder. BMJ 2005; 331: 1453–1456.
12. Dubert T, Voche P, Dumontier C, Dinh A. The DASH questionnaire. French translation of a trans-cultural adaptation. Chir Main 2001; 20: 294–302.
13. Fayad F, Lefevre-Colau MM, Macé Y, Fermanian J, Mayoux-Benhamou A, Roren A, et al. Validation of the French version of the Disability of the Arm, Shoulder and Hand questionnaire (F-DASH). Joint Bone Spine 2007; Aug 30 [Epub ahead of print].
14. Karduna AR, McClure PW, Michener LA, Sennett B. Dynamic measurements of three-dimensional scapular kinematics: a validation study. J Biomech Eng 2001; 123: 184–190.
15. Ludewig PM, Cook TM, Shields RK. Technical note: comparison of surface sensor and bone-fixed measurement of humeral motion. J Appl Biomech 2002; 18: 163–170.
16. Harryman DT 2nd, Sidles JA, Clark JM, McQuade KJ, Gibb TD, Matsen FA 3rd. Translation of the humeral head on the glenoid with passive glenohumeral motion. J Bone Joint Surg Am 1990; 72: 1334–1343.
17. Biryukova EV, Roby-Brami A, Frolov AA, Mokhtari M. Kinematics of human arm reconstructed from spatial tracking system recordings. J Biomech 2000; 33: 985–995.
18. Meskers CG, Vermeulen HM, de Groot JH, van Der Helm FC, Rozing PM. 3D shoulder position measurements using a six-degree-of-freedom electromagnetic tracking device. Clin Biomech 1998; 13: 280–292.
19. Wu G, van der Helm FC, Veeger HE, Makhsous M, Van Roy P, Anglin C, et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion – part II: shoulder, elbow, wrist and hand. J Biomech 2005; 38: 981–992.
20. Fayad F, Hoffmann G, Hanneton S, Yazbeck C, Lefevre-Colau MM, Poiraudeau S, et al. 3-D scapular kinematics during arm elevation: effect of motion velocity. Clin Biomech 2006; 21: 932–941.
21. Vermeulen HM, Stokdijk M, Eilers PH, Meskers CG, Rozing PM, Vliet Vlieland TP. Measurement of three dimensional shoulder movement patterns with an electromagnetic tracking device in patients with a frozen shoulder. Ann Rheum Dis 2002; 61: 115–120.
22. Yamaguchi K, Sher JS, Andersen WK, Garretson R, Uribe JW, Hechtman K, et al. Glenohumeral motion in patients with rotator cuff tears: a comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000; 9: 6–11.
23. Mell AG, LaScalza S, Guffey P, Ray J, Maciejewski M, Carpenter JE, et al. Effect of rotator cuff pathology on shoulder rhythm. J Shoulder Elbow Surg 2005; 14: S58–S64.
24. Matias R, Pascoal AG. The unstable shoulder in arm elevation: a three-dimensional and electromyographic study in subjects with glenohumeral instability. Clin Biomech 2006; 21: S52–S58.
25. Bot SD, Terwee CB, van der Windt DA, Bouter LM, Dekker J, de Vet HC. Clinimetric evaluation of shoulder disability questionnaires: a systematic review of the literature. Ann Rheum Dis 2004; 63: 335–341.