OBJECTIVES: The number of people in Western countries on long-term sick-leave and disability pension due to musculoskeletal complaints and psychological health problems is increasing. The main objective of this study was to examine whether fear-avoidance beliefs, illness perceptions, subjective health complaints, and coping are prognostic factors for return to work after multidisciplinary vocational rehabilitation, and to assess the relative importance and inter-relationship of these factors.
METHODS: A prospective cohort study with a 1-year follow-up period was performed. A total of 135 individuals on long-term sick-leave (87 women, mean age 45 years) participated in a 4-week inpatient multidisciplinary vocational rehabilitation programme. The participants had been out of work for an average of 10.5 months.
RESULTS: Fear-avoidance beliefs about work was the most important risk factor for not returning to work, both at 3 months (odds ratio (OR) 3.8; confidence interval (CI) 1.30–11.32) and 1 year (OR 9.5; CI 2.40–37.53) after the intervention. Forty-eight percent of the variance in fear-avoidance beliefs was explained by subjective health complaints, illness perceptions and education. Coping explained only 1% of the variance.
CONCLUSION: These findings indicate that interventions for these patients should target fear of returning to work and illness perceptions about subjective health complaints.
Key words: multidisciplinary vocational rehabilitation, return to work, subjective health complaints, illness perceptions, fear-avoidance, coping, expectancy.
J Rehabil Med 2008; 40: 548–554
Correspondence address: Irene Øyeflaten, Attføringssenteret i Rauland, NO-3864 Rauland, Norway. E-mail: irene.oyeflaten @air.no
Submitted December 12, 2006; accepted February 19, 2008
*This paper was presented as a poster at the 14th European Conference on Public Health, 16–18 November 2006, in Montreaux, Switzerland.
INTRODUCTION
The main objective of this study was to examine whether fear-avoidance beliefs, illness perceptions, subjective health complaints, and coping were prognostic factors for return to work (RTW) after multidisciplinary vocational rehabilitation, and to assess the relative importance and inter-relationship of these factors.
Despite the improvement in objective measures in health, long-term sickness compensation and disability pension in Western countries has increased substantially (1, 2). Diagnoses related to musculoskeletal and psychiatric complaints are among the most common causes of sickness absence and long-term incapacity to work (2, 3). Most of the increased trend is in non-specific conditions, largely subjective complaints, often with little objective pathology or impairment (2). In particular, for the musculoskeletal complaints, up to 85% of cases are non-specific (4). For these conditions there is a high rate of co-morbidity with other subjective health complaints (5), and the degree of co-morbidity influences the prognosis and degree of disability (6). The intensity of complaints forms a continuum from normal complaints to conditions that require medical care and are incompatible with participation in social and working life (7). RTW following long-term sick-leave is influenced by a mixture of medical, psychological and social factors (8). To be able better to target the interventions, knowledge of predictive factors is required.
The impairment from severe cases of subjective health complaints, including RTW, is related to the perception, attribution and expectancies of the individual. Expectations of treatment outcome and RTW, are in part determined by earlier experience and learning. The ability to handle demands and challenges is, according to the Cognitive Activation Theory of Stress (CATS; 9), dependent on acquired expectancies of the situation and on the resources available to the individual. In CATS, coping is defined as positive response outcome expectancies, i.e. the individual expects to be able to handle a difficult and challenging situation. Positive expectancies and good health (9, 10) may be enhanced through multidisciplinary interventions (11), and may influence RTW (12). Expecting to RTW is an important prognostic factor (13, 14) and individuals with no, or negative response outcome expectancies, may not believe in RTW (9).
Illness perceptions may be related to both stimulus expectancy and response outcome expectancy (9), and are the patient’s cognitive and emotional models of health and disease (15). Illness perceptions include the complaints associated with the illness, personal ideas about aetiology, perceived duration of the illness, expected effects of outcome, and expectations of cure control or recovering from the illness (16). Illness perceptions are related to RTW regardless of the severity of the illness, in patients with myocardial infarction (17) as well as in chronic fatigue syndrome (18). Our hypothesis is that illness perception is an important factor for RTW following multidisciplinary vocational rehabilitation.
Patients on long-term sick-leave related to subjective health complaints have often established a belief that pain is a sign of damage or harm to the body, and that activities that might cause pain should be avoided (19), i.e. establish a negative response outcome expectancy regarding work or activities (9). The fear-avoidance model is based on cognitive-behavioural theory explaining why some acute low back pain sufferers develop a chronic pain problem (20). Pain-related fear has been shown to be more disabling than the pain itself (21, 22), and is an important factor in explaining the transition from acute low back pain to chronic conditions (23). An understanding of the development of chronic health problems is crucial for both prevention and better management of pain conditions (24). Fear-avoidance beliefs are associated with prolonged disability and work absence in patients with low back pain (12, 25), and are related to level of disability among people with chronic pain (19). There is, therefore, reason to assume that interventions based on reducing fear-avoidance-based behaviours may be a successful intervention (20, 26).
Expectancies of outcome, coping, illness perceptions and fear-avoidance have been shown to be important predictors for RTW for patient groups with specific diagnoses (12–14). However, it is not established whether these factors predict RTW for individuals who have been sick-listed for a long time for complex non-specific health conditions (24, 27).
The aims of this study were: (i) to identify the prognostic value of subjective health complaints, fear-avoidance beliefs, illness perceptions and coping for RTW after a 4-week vocational rehabilitation programme for individuals on long-term sickness leave; and (ii) to explore which variables could explain significant variance in the main predictor.
METHODS
Design
This study was a prospective cohort study with a 12-month follow-up period, examining possible predictive factors on RTW measured 3 and 12 months after a multidisciplinary vocational rehabilitation programme.
Participants
A total of 135 individuals, 87 women (64%) and 48 men (36%) participated in the study (mean age 45 years; standard deviation (SD) 8.4; age range 24–61 years). They were recruited from a sample of 172 consecutive long-term sick-listed individuals, participating in a 4-week inpatient multidisciplinary vocational rehabilitation programme during the autumn of 2002. Patients were admitted to the rehabilitation centre based on referrals from their general practitioners (GP), National Health Insurance offices or labour marked agencies. They were recruited from the whole country, both urban and rural areas. The patients did not pay any charge to attend the programme. Inclusion criteria at the rehabilitation centre were: being motivated to participate in the programme and having an intentional goal and plan to RTW. In addition, other relevant medical examinations and treatments should have been tried before admittance to the programme. Exclusion criteria were: serious psychiatric disorders or undecided applications for disability pension or insurance claims.
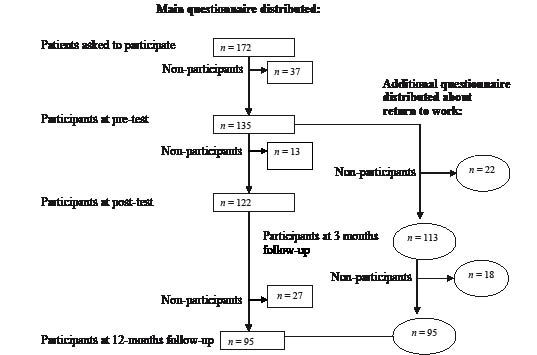
All participants answered a comprehensive set of questionnaires (pre-test) before they entered the rehabilitation programme. The same sets of questionnaires were distributed to the participants 4 weeks (post-test; response rate 90% (n = 122)) and (by post) 12 months (follow-up test; response rate 70% (n = 95)) after completing the rehabilitation programme. Three and 12 months after completing the rehabilitation programme data and sickness leave were collected from questionnaires (by post) (response rate at 3 months; 84% (n = 113) and after 12 months; 70% (n = 95)) (Fig. 1).
Multidisciplinary vocational rehabilitation programme
The study was performed at a national vocational rehabilitation centre offering a 4-week inpatient multidisciplinary rehabilitation programme, with 6 1-hour long sessions 5 days per week. The aim of the multidisciplinary rehabilitation programme was to help individuals on long-term sick-leave with complex, non-specific subjective health complaints, mainly related to musculoskeletal and psychological diagnoses, to improve their level of functioning, improve their work ability, and to increase the likelihood of RTW. The multidisciplinary rehabilitation programme included a combination of individual and group-based interventions with physical activity, education and cognitive behavioural modification. Self-confidence, coping and learning were important objectives for all activities offered. The multidisciplinary rehabilitation team consisted of physicians, nurses, physiotherapists, vocational social workers and sport educators.
Instruments and outcome measures
The comprehensive questionnaire comprised 8 standardized instruments, demographic variables, level of education, self-ratings of health and fitness, physical activity and exercise, sleep, smoking, and alcohol consumption. Medical diagnosis, length of sickness leave, occupation, and work-related conditions at baseline were collected from patient journals. RTW and sickness leave were measured by self-report in a questionnaire administered 3 and 12 months after the intervention.
RTW was defined as return to work-related activity (see Table II). Return to ordinary work, return with adjusted work tasks, new work tasks/same employer, new employer and “work related re-employment” (paid by the public health insurance or labour-agency) were included in work-related activity. Not returned to work was defined as not in work at the moment (due to sickness compensation, unemployment, student or other reasons) and “active sick-leave”/vocational training.
Subjective Health Complaints (SHC) Inventory (28) consists of 29 questions regarding common somatic and psychological complaints over the last 30 days, rated on a 4-point scale. The items are scored on 5 sub-scales: SHC musculoskeletal complaints (8 items), SHC pseudoneurological complaints (7 items: fatigue, anxiety, sleep-problems, sadness/depression, dizziness, hot flushes, extra heart-beats), gastrointestinal complaints (7 items), SHC allergy (5 items) and SHC influenza (2 items).
Revised Illness Perceptions Questionnaire (IPQ-R) (16, 29) is based on the 5 components of illness representations in Leventhal’s self-regulatory model. The questionnaire is a method for assessing cognitive representations of illness and contains 9 scales or components (identity, timeline acute/chronic, timeline cyclical, consequences, personal control, cure control, illness coherence, emotional representations and cause).
Fear-Avoidance Beliefs Questionnaire (FABQ) (21) was created to measure pain-related fear and fear-avoidance behaviour. The questionnaire consists of 11 statements rated on a 7-point scale. The test comprises 2 sub-scales: fear-avoidance beliefs for physical activity and fear-avoidance beliefs for work.
Coping was measured with 5 different standardized instruments, as follows:
Perceived Self-Efficacy Scale (GPSES) (30) consists of 10 questions rated on a 4-point scale. The questionnaire was created to assess a general sense of perceived self-efficacy (coping expectancy) with the aim of predicting coping with daily hassles as well as adaptation after all kinds of stressful life events.
Utrecht Coping List (UCL) (10, 31) consists of 47 statements about how one would cope with problems. Each statement is rated on a 4-point scale. The test yields 2 major factors based on 7 subscales: instrumental mastery-oriented coping and emotion-focused coping.
Coping (32) was created to assess coping expectancy and how the individual considers their own abilities and beliefs in the future. The schema consists of 7 statements rated on a 4-point scale.
Hopelessness (33) measures negative expectancies about oneself and the future and consists of 2 items rated on a 5-point scale.
The Ladder of Life (34) consists of 10 “steps” indicating the best and worst possible quality of life. The individual rates on which of the 10 steps he/she consider him/herself to have been one year ago, where he/she is just now and where he/she expects to be one year from now.
Statistics
SPSS 11.0 and 12.1 for Windows was used for the statistical analyses. Descriptive data was determined for baseline characteristics and RTW. The χ2 test was used to explore gender differences. Logistic regression was used to evaluate prognostic factors for RTW. Continuous data used in the regression model were dichotomized by the median into high and low score. Hierarchical multiple regression was performed to determine which set of variables explained the main predictor for RTW (fear-avoidance beliefs).
RESULTS
Out of 172 invited participants, 135 (78.5%) individuals returned the questionnaires at baseline. The 37 non-participants (Fig. 1) did not differ from the participants regarding gender (p = 0.64; χ2), medical diagnosis (p = 0.24; χ2), age (p = 0.498; t-test), or sick-leave period (p = 0.405; t-test).
Fig. 1. Study flow-chart.
Work status and diagnosis at baseline
All the participants were on sickness leave, with a mean duration of sick-leave of 10.5 months, (SD = 2.8) and a range of 0–48 months, before inclusion in the study. About one-third (34%) (n = 46) of the participants had been sick-listed more than one year. Sick-leave length distribution was skewed to the left. All participants were diagnosed by their GP according to the International Classification of Primary Care (ICPC) diagnostic system when they were granted their initial sickness certificate. According to the ICPC diagnoses 59 participants (43.7%) were sick-listed for a diagnosis related to musculoskeletal complaints, 44 (31.9%) for psychiatric diagnoses, and 31 (23%) had no specific diagnosis. In Norway the ICPC is the only diagnostic system used within general practice and primary care. More than 50% of the participants were registered with more than one medical diagnosis (ICPC) at baseline, and about half of these participants had more than one diagnosis in 2 different diagnostic groups, i.e. one musculoskeletal diagnosis and one psychiatric diagnosis.
Occupational and education status at baseline
Occupational status was distributed equally between the participants: 18% were blue-collar workers (n = 24), 22% were white-collar workers (n = 29), 16% worked in school or kindergarten (n = 22), 26% worked in the healthcare sector (n = 35) and 16% worked in the service field (n = 21). Sixty-five percent were full-time workers (n = 88), 25% worked part-time (n = 34) and 8% were unemployed (n = 11). The educational level was, on average, 13.5 years (SD 3.3) with a range of 8–22 years.
Co-morbidity
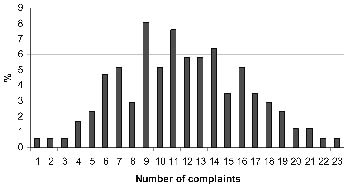
The participants reported, on average, 12 subjective health complaints (SD 4.6) during the last 30 days, with a range of 1–23 complaints (29 possible complaints) (Fig. 2). Fatigue was the most frequently reported complaint, and was reported by 84% of participants, followed by neck pain, headache, sleep problems, and sadness/depression (Table I). Seventy-six percent of participants reported complaints from 2 or several organ systems, i.e. musculoskeletal, pseudoneurological and gastrointestinal complaints.
| Table I. Ranked distribution of the 14 most-reported subjective health complaints. Number and percentage. Separate scores for men and women. χ2 is calculated for gender differences |
| Complaint | All | Men | Women |
| n = 135 n (%) | n = 48 n (%) | n = 87 n (%) | p-value* |
| Fatigue | 113 (83.7) | 37 (77.1) | 76 (87.4) | 0.192 |
| Neck pain | 110 (81.5) | 35 (75.0) | 74 (85.1) | 0.326 |
| Headache | 102 (75.6) | 35 (72.9) | 67 (77.0) | 0.815 |
| Sleep problems | 97 (71.9) | 31 (64.6) | 66 (75.9) | 0.232 |
| Sadness/depression | 95 (70.4) | 26 (54.2) | 69 (79.3) | 0.007 |
| Low back pain | 93 (68.9) | 31 (64.6) | 62 (71.3) | 0.358 |
| Shoulder pain | 91 (67.4) | 28 (58.3) | 63 (72.4) | 0.185 |
| Arm pain | 77 (57.0) | 22 (45.8) | 55 (63.2) | 0.070 |
| Upper back pain | 70 (51.9) | 17 (35.4) | 53 (60.9) | 0.016 |
| Dizziness | 58 (43.0) | 17 (35.4) | 41 (47.1) | 0.257 |
| Diarrhoea | 58 (43.0) | 19 (39.6) | 39 (44.8) | 0.643 |
| Leg pain during physical activity | 54 (40.0) | 13 (27.1) | 41 (47.1) | 0.055 |
| Anxiety | 52 (38.5) | 13 (27.1) | 39 (44.8) | 0.051 |
| Gas discomfort | 51 (37.8) | 15 (31.3) | 36 (41.1) | 0.034 |
| *Level of significance based on χ2 test. p < 0.05 shown in bold. |
Fig. 2. Percentage distribution of the number of complaints within subjective health complaints.
Return to work
After 3 months 60% of the participants had returned to work, and at 12-months follow-up 70% had returned to work (Table II). Type of diagnosis at baseline (musculoskeletal, psychiatric or unspecified diagnosis) did not influence RTW after 3 months (p = 0.24; χ2) or after 12 months (p = 0.25; χ2).The length of sick-leave at baseline did not affect RTW at 3 months (p = 0.25; χ2), but those with more than 12 months sick-leave at baseline were less likely to RTW 12 months after the intervention (p = 0.007; χ2).
| Table II. Return to work and sickness absence after 3 months (n = 113) and at 12 months (n = 95) follow-up |
| | 3 months follow-up n (%) | 12 months follow-up n (%) |
| Total return to work-related activity | 68 (60.2) | 66 (69.5) |
| Return to ordinary work | 44 (38.9) | 43 (45.3) |
| Return with adjusted work tasks | 4 (3.5) | 4 (4.2) |
| New work tasks/same employer | 5 (4.4) | 4 (4.2) |
| New employer | 2 (1.8) | 5 (5.3) |
| “Work-related re-employment” | 13 (11.5) | 10 (10.5) |
| Total not return to work-related activity | 45 (39.8) | 29 (30.5) |
| “Active sick-leave” / vocational-training | 19 (16.8) | 8 (8.4) |
| Not in work at the moment (sickness compensation or without work) | 26 (23.0) | 21 (22.1) |
Prognostic factors for RTW at 3 months follow-up
There was an increased risk for not RTW with high score on SHC pseudoneurology, SHC allergy and fear-avoidance beliefs (Table III). Instrumental mastery-oriented coping had a protective effect; the chances of RTW were 5 times higher with high scores on instrumental mastery-oriented coping than with low coping. After adjusting for all factors significant in the first part of the logistic regression analysis, high scores on SHC pseudoneurology, fear-avoidance beliefs for work, and low score on instrumental mastery-oriented coping showed 3 times higher risk for not returning to work.
| Table III. Odds ratios (OR) (95% confidence interval) for no return to work after 3 months |
| | OR adjusted for gender and age | OR adjusted for gender, age and significant factors† |
| n = 113 | p-value | n = 98 | p-value* |
| Education | 0.9 (0.42–1.99) | 0.83 | | |
| SHC musculoskeletal | 1.2 (0.54–2.71) | 0.70 | | |
| SHC pseudoneurology | 3.5 (1.51–8.02) | 0.004 | 3.3 (1.14–9.60) | 0.03 |
| SHC gastrointestinal | 1.9 (0.83–4.18) | 0.14 | | |
| SHC allergy | 2.6 (1.12–5.93) | 0.03 | 2.8 (0.98–8.22) | 0.053 |
| SHC influenza | 1.3 (0.57–2.82) | 0.61 | | |
| Fear-avoidance beliefs for activity | 1.8 (0.80–4.17) | 0.16 | | |
| Fear-avoidance beliefs for work | 2.3 (1.00–5.49) | 0.05 | 3.8 (1.30–11.32) | 0.02 |
| “Coping” | 1.4 (0.63–3.25) | 0.41 | | |
| Hopelessness | 1.8 (0.79–4.18) | 0.21 | | |
| Instrumental coping | 0.2 (0.08–0.51) | 0.001 | 0.3 (0.10–0.74) | 0.01 |
| Emotion-focused coping | 1.2 (0.54–2.71) | 0.64 | | |
| Self-efficacy | 0.8 (0.33–1.73) | 0.51 | | |
| *Level of significance based on logistic regression analysis. p < 0.05 in bold. †Adjustment was made for all factors in the model significant in the first part of the analysis. SHC: subjective health complaints. |
Prognostic factors for RTW at 12 months follow-up
After one year there was an increased risk for not RTW with short education (≤ 12 years) and high score in fear-avoidance beliefs for work (Table IV). Instrumental mastery-oriented coping no longer had any protective effect, but had changed to be a risk factor for not RTW. After adjusting for all factors significant in the first part of the logistic regression analysis, there was still a high risk of not RTW with high scores on fear-avoidance beliefs for work and instrumental mastery-oriented coping. Short education was no longer a risk factor. The large confidence intervals indicate uncertainty concerning the relative risks on fear-avoidance beliefs and instrumental mastery-oriented coping.
| Table V. Hierarchical multiple regression analysis of subjective health complaints and illness perception with fear-avoidance beliefs for work as dependent variable (n = 135) |
| | Step 1 | Step 2 | Step 3 |
| β Beta | Significant p-value | β Beta | Significant p-value | β Beta | Significant p-value |
| 1. Gender | –0.078 | 0.354 | –0.111 | 0.166 | –0.029 | 0.703 |
| 2. Age | –0.198 | 0.019 | –0.154 | 0.043 | –0.139 | 0.051 |
| 3. Education | –0.365 | 0.000 | –0.286 | 0.000 | –0.183 | 0.015 |
| 4. SHC musculoskeletal* | | | 0.482 | 0.000 | 0.397 | 0.000 |
| 5. SHC pseudoneurology* | | | –0.198 | 0.033 | –0.258 | 0.008 |
| 6. SHC gastrointestinal* | | | –0.061 | 0.455 | 0.014 | 0.859 |
| 7. SHC allergy* | | | –0.035 | 0.707 | –0.055 | 0.507 |
| 8. SHC influenza* | | | –0.034 | 0.667 | –0.038 | 0.593 |
| 9. Identity† | | | | | –0.122 | 0.232 |
| 10. Timeline acute/chronic† | | | | | 0.200 | 0.031 |
| 11. Timeline cyclical† | | | | | –0.033 | 0.643 |
| 12. Consequences† | | | | | 0.284 | 0.001 |
| 13. Personal control† | | | | | –0.226 | 0.006 |
| 14. Cure control† | | | | | 0.109 | 0.262 |
| 15. Illness coherence† | | | | | 0.134 | 0.082 |
| 16. Emotional representations† | | | | | 0.077 | 0.350 |
| R2 | 0.177 | | 0.369 | | 0.545 | |
| Adjusted R2 | 0.156 | | 0.325 | | 0.477 | |
| R2 change | 0.177 | | 0.192 | | 0.176 | |
| Significant change (F) | p < 0.001 | | p < 0.001 | | p < 0.001 | |
| *High score is many reported subjective health complaints. †High score is many symptoms associated with the complaint, perceptions of long duration, perceptions of cyclical/episodic duration, beliefs of illness severity and consequences, beliefs of personal control, beliefs of treatment control, good illness coherence and many emotional representations. SHC: subjective health complaints. |
| Table IV. Odds ratios (OR) (95% confidence interval (95% CI)) for no return to work after 12 months |
| | OR adjusted for gender and age | OR adjusted for gender, age and significant factors† |
| n = 113 | p-value | n = 98 | p-value* |
| Education | 0.2 (0.09–0.64) | 0.005 | 0.4 (0.12–1.12) | 0.07 |
| SHC musculoskeletal | 1.8 (0.71–4.54) | 0.21 | | |
| SHC pseudoneurology | 0.7 (0.31–1.91) | 0.53 | | |
| SHC gastrointestinal | 1.5 (0.61–3.61) | 0.40 | | |
| SHC allergy | 0.9 (0.40–2.20) | 0.80 | | |
| SHC influenza | 1.2 (0.51–2.98) | 0.67 | | |
| Fear-avoidance beliefs for activity | 1.6 (0.65–4.21) | 0.31 | | |
| Fear-avoidance beliefs for work | 6.9 (2.30–20.91) | 0.001 | 9.5 (2.40–37.53) | 0.001 |
| “Coping” | 0.9 (0.35–2.30) | 0.83 | | |
| Hopelessness | 1.2 (0.51–3.04) | 0.71 | | |
| Instrumental coping | 3.1 (1.20–8.24) | 0.02 | 5.9 (1.63–21.41) | 0.007 |
| Emotion-focused coping | 0.6 (0.31–1.60) | 0.33 | | |
| Self-efficacy | 2.1 (0.85–5.24) | 0.11 | | |
| *Level of significance based on logistic regression analysis. p < 0.05 in bold. †Adjustment was made for all factors in the model significant in the first part of the analysis. SHC: subjective health complaints. |
What explains fear-avoidance beliefs for work?
Together with education, both subjective health complaints and illness perceptions contributed to explaining fear-avoidance beliefs for work (Table V). In a fully adjusted model, a total of 48% of the variance for fear-avoidance for work was explained by these variables. Gender, age, and education explained 18% of the variance. Subjective health complaints explained 19% of the variance, while illness perceptions explained 18%. The coping variables self-efficacy, emotion-focused coping, instrumental mastery-oriented coping, and hopelessness explained only 1% of the variance in fear-avoidance beliefs for work (adjusted R2 0.556, significant change 0.781).
DISCUSSION
Fear-avoidance beliefs for work were the main prognostic factor for RTW, both 3 and 12 months after the intervention. Subjective health complaints and low coping were significant risk factors for sick-leave at 3-months follow-up.
At 3-months follow-up, an adjusted model showed 3 times higher risk for not RTW for high scores on subjective health complaints (SHC pseudoneurology), fear-avoidance beliefs for work, and low coping. At 12-months follow-up, the adjusted model showed 9 times higher risk for not RTW with high scores on fear-avoidance beliefs for work. Subjective health complaints did not predict RTW after 12 months. Coping shifted from being a protective factor 3 months after the intervention, to a strong risk factor for not RTW after 12 months. Instrumental mastery-oriented coping may be used as a measure of a general positive response outcome expectancy (9, 10), i.e. a belief that “my strategies will yield a good result”. The goal of the rehabilitation programme was RTW.
The participants may therefore have believed that RTW was a good solution to their health and work situation at 3-months follow-up. At 12-months follow-up some participants may have experienced that the daily hassles and demands at home and work were an obstacle to RTW. When RTW is the goal, but is not reached, a coping individual has, according to the cognitive activation theory of stress (9, 10), 2 options; one is to try harder to reach the goal the other is to change the goal. The coping participant who has not returned to work 12 months after the intervention may now consider further sick-leave to be a positive solution to health problems and difficult work situations. The patient is coping, but at a high cost. We know that patients have strong influence on whether their physician grants them a sick-leave certificate and that the decision hinges on factors such as the patients needs, expectations and demands (35). This shift in coping as a predictor may have consequences for the way we treat and follow-up patients after rehabilitation.
Fear-avoidance beliefs for work explained RTW in this study. The result is in accordance with previous findings on the development of chronic conditions and the level of functional ability among patients with low back pain (21). Fear-avoidance itself was explained by a combination of subjective health complaints, illness perceptions and education (48% of the variance). This agrees with findings that pain, illness perceptions, expectancy, and pain-related fear are strongly inter-related in patients with back pain and have a predictive value for future pain and disability (13). Other studies have also identified low education as an independent predictor of long-term absence (36) and disability (37). High levels of education may be associated with the resources and motivation to do something with one’s own health and work situation, and may be related to the general socioeconomic gradients for health (38). This group may also be characterized by mobility and good employment opportunities. Coping, the expectancy to be able to handle challenging situations, explained only 1% of the variance in fear-avoidance beliefs. This is surprising, since expectations of outcome are essential within coping and stress theory (9), and in psychosocial theories where expectations are significant (13, 14). It appears that, in our data where all the patients have participated in a rehabilitation programme, illness perceptions, education, and the level of subjective health complaints are the main links between fear-avoidance beliefs and RTW.
After 3 months, 60% of participants had returned to work, and at 12-months follow-up 70% had returned. This appears to be a very good result, but the lack of any control group in this study does not allow any conclusions to be drawn about the effect of the intervention.
There are several possible shortcomings to this study. Self-rating of both the dependent and independent variables may inflate the risk estimates. Rather large confidence intervals for significant predictive variables may be explained by a large range between the lowest and highest score and may limit the strength of the conclusion. Possible inter-correlations between the standardized instruments may also bias the results. On the other hand, inter-correlations between the instruments may be a strength, since it is obvious that no single item alone predicts or explains RTW in sick-listed individuals with complex conditions. The response rate tends to decrease in long-term follow-up studies, as is the case here.
This study confirms that long-term sick-listed individuals are a complex patient group reporting a broad spectrum of different health complaints, and a high level of co-morbidity. High levels of co-morbidity are also found in long-term patients with low back pain (5) and patients with “functional” gastrointestinal problems (39, 40). There is, therefore, reason to question whether a single medical diagnosis reflects the complex situation for these long-term sick-listed individuals. In our study the diagnosis did not influence RTW. The important factors appear to be complex and non-specific subjective health complaints, and this terminology may therefore be better than “unspecific medical diagnosis”.
In conclusion, it is likely that, to be successful, interventions for long-term sick-listed individuals with complex health conditions should be directed at fear-avoidance beliefs, since this was the main prognostic factor for not RTW. Our findings also indicate that interventions should target illness perceptions about subjective health complaints. Directing rehabilitation programmes to overcome biopsychosocial obstacles to RTW may be fundamental to better clinical and occupational management and minimizing incapacity (3). There is a need for studies that further examine these complex issues in rehabilitation and clinical practice.
REFERENCES
1. Schultz IZ, Gatchel RJ, editors. Handbook of complex occupational disability claims. Early risk identification, intervention and prevention. New York: Springer; 2005, p. ix–xi.
2. Waddell G. Preventing incapacity in people with musculoskeletal disorders. Br Med Bull 2006; 77/78: 55–69.
3. Eriksen HR, Ursin H. Subjective health complaints, sensitization, and sustained cognitive activation (stress). J Psychosom Res 2004; 56: 445–448.
4. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, et al. European guidelines for the management of chronic non-specific low back pain. Eur Spine J 2006; 15 Suppl 2: s192–s300
5. Hagen EM, Svensen E, Eriksen HR, Ihlebæk CM, Ursin H. Comorbid subjective health complaints in low back pain. Spine 2006; 31: 1491–1495.
6. Natvig B, Bruusgaard D, Eriksen W. Localized low back pain and low back pain as part of widespread musculoskeletal pain: two different disorders? A cross-sectional population study. J Rehabil Med 2001; 33: 21–25.
7. Ihlebaek C, Eriksen HR, Ursin H. Prevalence of subjective health complaints (SHC) in Norway. Scand J Public Health 2002; 30: 20–29.
8. Staal JB, Hlobil H, van Tulder MW, Koke AJ, Smid T, van Mechelen W. Return-to-work interventions for low back pain: a descriptive review of contents and concepts of working mechanisms. Sports Med 2002; 32: 251–267.
9. Ursin H, Eriksen HR. The cognitive activation theory of stress. Psychoneuroendocrinology 2004; 29: 567–592.
10. Eriksen HR, Olff M, Ursin H. The CODE: a revised battery for coping and defense and its relations to subjective health. Scand J Psychol 1997; 38: 175–182.
11. Storrø S, Moen J, Svebak S. Effects on sick-leave of a multidisciplinary rehabilitation programme for chronic low back, neck or shoulder pain: comparison with usual treatment. J Rehabil Med 2004; 36: 12–16.
12. Turner JA, Franklin G, Fulton-Kehoe D, Sheppard L, Wickizer TM, Wu R, et al. Worker recovery expectations and fear-avoidance predict work disability in a population-based workers’ compensation back pain sample. Spine 2006; 31: 682–689.
13. Boersma K, Linton SJ. Expectancy, fear and pain in the prediction of chronic pain and disability: a prospective analysis. Eur J Pain 2006; 10: 551–557.
14. Schultz IZ, Crook J, Meloche GR, Berkowitz J, Milner R, Zuberbier OA, Meloche W. Psychosocial factors predictive of occupational low back disability: towards development of a return-to-work model. Pain 2004; 107: 77–85.
15. Leventahl H, Nerenz D, Steele DJ. Illness representations and coping with health threats. In: Baum A, Taylor SE, Singer JE, editors. Handbook of psychology and health. Hillsdale, New Jersey: Erlbaum; 1994, p. 219–252.
16. Weinman J, Petrie KJ, Moss-Morris R, Horne R. The Illness Perception Questionnaire: a new method for assessing the cognitive representation of illness. Psychol Health 1996; 11: 431.
17. Petrie KJ, Weinman J, Sharpe N, Buckley J. Role of patients’ view of their illness in predicting return to work and functioning after myocardial infarction: longitudinal study. BMJ 1996; 312: 1191–1194.
18. Petrie K, Moss-Morris R, Weinman J. The impact of catastrophic beliefs on functioning in chronic fatigue syndrome. J Psychosom Res 1995; 39: 31–37.
19. Geisser ME, Robinson ME, Miller QL, Bade SM. Psychosocial factors and functional capacity evaluation among persons with chronic pain. J Occup Rehabil 2003; 13: 259–276.
20. Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med 2007; 30: 77–94.
21. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain 1993; 52: 157–168.
22. Crombez G, Vlaeyen JW, Heuts PH, Lysens R. Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain 1999; 80: 329–339.
23. Buer N, Linton SJ. Fear-avoidance beliefs and catastrophizing: occurrence and risk factor in back pain and ADL in the general population. Pain 2002; 99: 485–491.
24. Linton SJ, Buer N, Vlaeyen J, Hellsing AL. Are fear avoidance beliefs related to the inception of an episode of back pain? A prospective study. Psychol Health 2000; 14: 1051–1059.
25. Fritz JM, George SZ, Delitto A. The role of fear-avoidance beliefs in acute low back pain: relationships with current and future disability and work status. Pain 2001; 94: 7–15.
26. Hagen EM, Svensen E, Eriksen HR. Predictors and modifiers of treatment effect influencing sick leave in subacute low back pain patients. Spine 2005; 30: 2717–2723.
27. Pransky G, Gatchel R, Linton SJ, Loisel P. Improving return to work research. J Occup Rehabil 2005; 15: 453–457.
28. Eriksen HR, Ihlebaek C, Ursin H. A scoring system for subjective health complaints (SHC). Scand J Public Health 1999; 27: 63–72.
29. Moss-Morris R, Weinman J, Petrie KJ, Horne R, Cameron LD, Buick D. The Revised Illness Perception Questionnaire (IPQ-R). Psychol Health 2002; 17: 1–16.
30. Schwarzer R, Jerusalem M. Generalized Self-Efficacy scale. In: Weinman J, Wright S, editors. Measures in health psychology: a user’s portfolio. Causal and control beliefs. Windsor, UK: NFER-Nelson; 1995, p. 35–37.
31. Schreurs PJG, Van De Willige G, Brosschot JF, Grau G, editors. De Utrechtse Copinglijst: UCL. Handleiding. Lisse: Swets en Zeitlinger; 1993.
32. Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. J Health Soc Behav 1981; 22: 337–356.
33. Everson SA, Goldberg DE, Kaplan GA, Cohen RD, Pukkala E, Tuomilehto J, Salonen JT. Hopelessness and risk of mortality and incidence of myocardial infarction and cancer. Psychosom Med 1996; 58: 113–121.
34. Andrews FM, Whitney SB. Developing measures of perceived life quality: results from several national surveys. Social Indicators Res 1974; 1: 1.
35. Haldorsen EM, Brage S, Johannesen TS, Tellnes G, Ursin H. Musculoskeletal pain: concepts of disease, illness, and sickness certification in health professionals in Norway. Scand J Rheumatol 1996; 25: 224–232.
36. Tveito TH, Halvorsen A, Lauvålien JV, Eriksen HR. Room for everyone in working life? 10% of the employees – 82% of the sickness leave. Norwegian J Epidemiol 2002; 12: 63–68.
37. Gjesdal S, Bratberg E. The role of gender in long-term sickness absence and transition to permanent disability benefits. Results from a multiregister based, prospective study in Norway 1990–1995. Eur J Public Health 2002; 12: 180–186.
38. Kristenson M, Eriksen HR, Sluiter JK, Starke D, Ursin H. Psychobiological mechanisms of socioeconomic differences in health. Soc Sci Med 2004; 58: 1511–1522.
39. Vandvik PO, Wilhelmsen I, Ihlebæk C, Farup PG. Comorbidity of irritable bowel syndrome in general practice: a striking feature with clinical implications. Aliment Pharmacol Ther 2004; 20: 1195–203.
40. Lind R, Arslan G, Eriksen HR, Kahrs G, Haug TT, Florvaag E, Berstad A. Subjective health complaints and modern health worries in patients with subjective food hypersensitivity. Digestive Dis Sci 2005; 50: 1245–1251.