OBJECTIVE: We tested the hypothesis that physically active people with spinal cord injury do not have increased subclinical atherosclerosis compared with an age-matched able-bodied group.
METHODS: Subjects comprised 28 wheelchair athletes with spinal cord injury (mean age 22 (standard deviation (SD) 3) years) and 24 recreationally active aged-matched able-bodied control participants (mean age 23 (SD 3) years). Intima media thickness, arterial compliance and β stiffness of the common carotid artery were measured using B-mode ultrasound. Aortic augmentation index was derived from applanation tonometry of the radial artery.
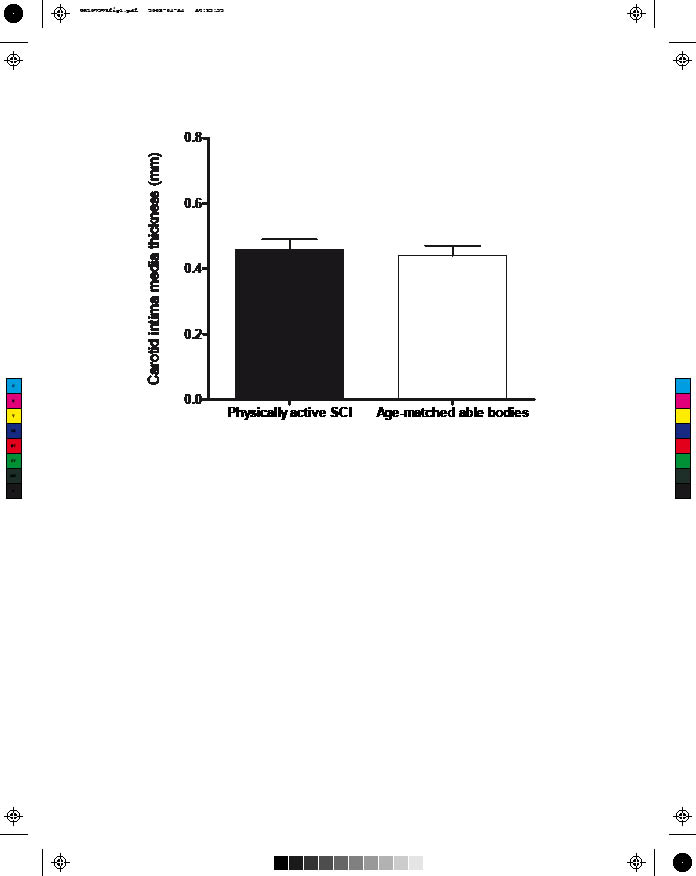
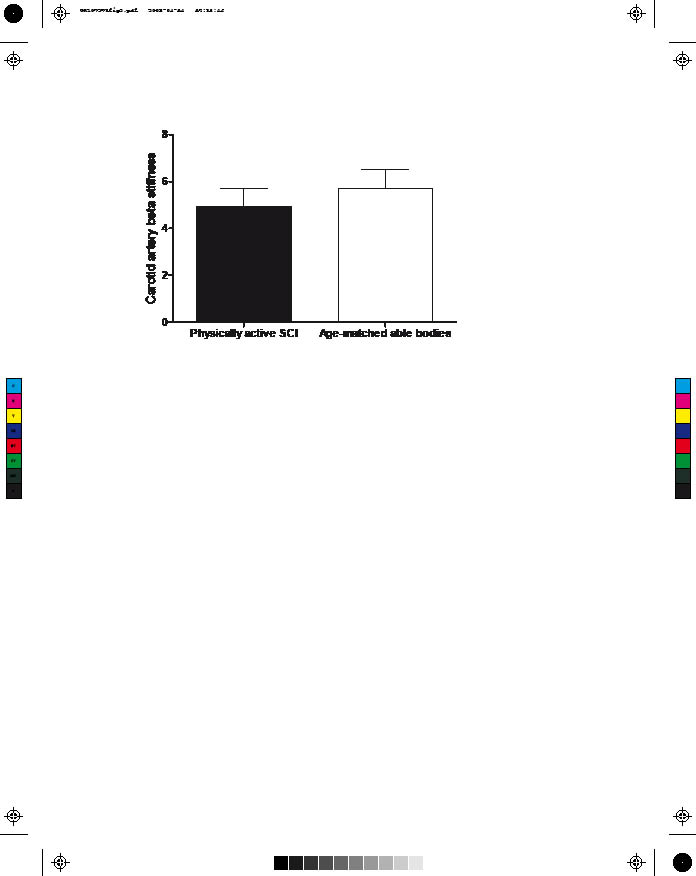
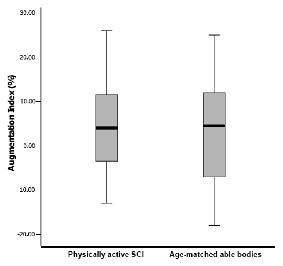
RESULTS: Carotid mean intima media thickness in persons with spinal cord injury did not differ from that of controls (0.46, SD 0.07 vs 0.44, SD 0.06, p = 0.94). Carotid artery β stiffness in persons with spinal cord injury also did not differ from that of controls (4.92, SD 1.6 vs 5.70, SD 1.6, p = 0.08). The augmentation index did not differ between groups (4.0% [–3.8–12.3] vs 4.5 %, [–8.0–12.0] of median and interquartile range, p = 0.78).
CONCLUSION: Participation in regular exercise may preserve arterial function in individuals with spinal cord injury when compared with aged-matched able-bodied participants.
Key words: spinal cord injury, carotid intima media thickness, arterial stiffness, augmentation index.
J Rehabil Med 2008; 40: 535–538
Correspondence address: Sae Young Jae, The Health and Integrative Physiology Laboratory, Department of Sports Informatics, University of Seoul, Seoul, South Korea, Siripdae-gil 13, Dongdaemun-gu, Seoul, 130-743, South Korea. E-mail: syjae@uos.ac.kr
Submitted October 2, 2007; accepted March 4, 2008
INTRODUCTION
Cardiovascular disease is one of the leading causes of death in people with spinal cord injury (SCI). This fact is related to potentially treatable risk factors, such as physical inactivity, smoking and overweight (1). Physical inactivity is a major risk factor for cardiovascular morbidity and mortality in people with SCI (2).
Non-invasive testing for identification of early sub-clinical atherosclerosis (3) is becoming more common. Carotid intima media thickness (IMT), a surrogate marker of atherosclerosis, is associated with increased risk of myocardial infarction and stroke in able-bodied populations (4). Individuals with SCI have greater atherosclerotic burden according to coronary artery calcification scores than do able-bodied controls (5), indicating the efficacy of early detection in this population. Although epidemiological studies report that higher levels of physical activity and fitness are associated with a lower prevalence of carotid atherosclerosis in middle-aged able-bodied men (6), these relationships have not been studied in persons with SCI.
Arterial stiffness is also associated with increased risk of cardiovascular diseases (7, 8) and several studies note a strong relationship between increased physical activity and reduced arterial stiffness in able-bodied populations (9, 10). It has been reported recently that physically inactive persons with SCI have significantly increased arterial stiffness compared with their age-matched able-bodied peers (11). However, it is unknown if active persons with SCI also have reduced arterial stiffness.
Because regular exercise reduces cardiovascular risk in persons with SCI (7), we hypothesized that physically active people with SCI would have similar carotid IMT and arterial stiffness compared with an age-matched able-bodied group. The aim of this study was therefore to compare carotid IMT and stiffness and aortic wave reflection in active persons with SCI vs age-matched able-bodied controls.
METHODS
We used a cross-sectional study design to compare carotid and arterial stiffness of 28 physically active competitive wheelchair athletes with low-level (below T6) SCI (caused by trauma, transverse myelitis, spina bifida and neuroblastoma) and 24 recreationally active aged-matched able-bodied control participants. According to the American Spinal Injury Association (ASIA) impairment scale, 10 participants with SCI were grade A, 4 were grade B, 7 were grade C, 5 were grade D, and 2 were grade E. Written informed consent was obtained from all participants, and the study protocol was approved by the University of Illinois at Urbana and Champaign institutional review board. None of the participants smoked or had an abnormal electrocardiogram, cardiovascular disease or diabetes. All subjects abstained from caffeine and exercise on the testing day and were at least 3-hours postprandial upon arrival at the laboratory for testing. Resting blood pressure was measured during seated rest following a 5–10 min period of quiet rest, using an automated blood pressure monitor (Omron, HEM-712C, Vernon Hills, IL, USA).
Carotid artery ultrasound imaging was performed using a high-resolution B-mode ultrasound system (Aloka, SSD 5500, Japan). IMT was defined as the distance between the leading edge of the lumen-intima interface and the leading edge of the media-adventitia interface of the far wall of the carotid artery. All measurements were made at end diastole. The IMT of the common carotid artery was determined from an average of 5 measurements of a 10-mm segment (separated by 2-mm intervals) obtained 2 cm proximal to the carotid bifurcation. The overall maximal IMT was defined as the mean of the maximal IMT of both the common carotid arteries. Carotid artery compliance and β-stiffness was measured by ultrasonography (Aloka, SSD 5500, Japan). The intra-class correlation coefficient (ICC) for carotid artery IMT in our laboratory is 0.95.
The cephalic portion of the right common carotid artery with the subject lying in a supine position was imaged in longitudinal section, 1–2 cm proximal to the bifurcation, using a high-resolution (7.5 MHz) linear array probe. Image analysis and calculation of arterial compliance (AC) was carried out using an automated wall detection echo-tracking software system. AC was calculated as:
| AC = | � (D1 * D1 – D0 * D0) |
| 4 (P1 – P0) |
where D1 and D0 are the maximum and minimum diameters, and P1 and P0 are the highest and lowest blood pressures. The β-stiffness index (β) was calculated as a means of adjusting arterial compliance for changes in distending pressure as follows:
In our laboratory, the ICC for carotid artery compliance and β-stiffness are ≥ 0.9.
Radial artery pressure waveforms were obtained in the sitting position from a 10-sec epoch using applanation tonometry and a high-fidelity strain gauge transducer (Millar Instruments, Houston, TX, USA). Using a generalized validated transfer function, a central aortic pressure waveform was reconstructed from the radial artery pressure waveform (SphygmoCor, AtCor Medical, Australia). Augmentation Index (AIx) was calculated as the ratio of amplitude of the pressure wave above its systolic shoulder to the total pulse pressure and expressed as a percentage, and used as an index of wave reflection. Because AIx is influenced by heart rate (12), AIx values were normalized to a heart rate of 75 bpm (AIx@75). Only high-quality recordings, defined as an in-device quality index ≥ 80% were included in the analysis. In our laboratory, the ICC obtained on 2 separate days was > 0.9 (13).
All values are presented as mean (standard deviation (SD)) and non-parametric results are presented as median and interquartile range. Comparison between groups was performed using independent t-test for the normally distributed data and Mann-Whitney U test for the non-normally distributed data. Statistical significance was set at p < 0.05 for all data. Statistical analyses were performed using the SPSS 12.0 (SPSS, Chicago, IL, USA).
RESULTS
Table I presents the characteristics of the subjects. There were no significant differences in age, body mass index, systolic or diastolic blood pressure. Resting heart rate was significantly higher in SCI athletes vs able-bodied controls (p < 0.05). Carotid mean IMT in persons with SCI did not differ from in the controls group (0.46, SD 0.07 vs 0.44, SD 0.06, p = 0.94) (Fig. 1). Carotid artery compliance (0.98, SD 0.3 vs 1.05, SD 0.4, p = 0.51) and β stiffness (4.92, SD 1.6 vs 5.7, SD 1.6, p = 0.08) (Fig. 2) did not differ significantly between groups. Also, there were no group differences for median [interquartile range] AIx (4.0% [–3.8 – 12.3] vs 4.5%, [–8.0 – 12.0], p = 0.78) (Fig. 3), nor were there differences between groups when the AIx was normalized to a heart rate of 75 bpm (1.0% [–6.0 – 7.5] vs –4.5%, [–13.8 – 4.8], p = 0.17) by Mann-Whitney U test.
| Table I. Characteristics of the subjects |
| Variable | Persons with SCI (n = 28) | Able-bodied controls (n = 24) |
| Age (years) | 22 (3) | 23 (3) |
| Gender (male/female), n | 17/11 | 12/12 |
| Body mass index (kg/m2) | 22 (4) | 24 (3) |
| Systolic blood pressure (mmHg) | 122 (14) | 119 (10) |
| Diastolic blood pressure (mmHg) | 72 (10) | 70 (7) |
| Resting heart rate (bpm)* | 73 (12) | 61 (9) |
| *p < 0.05. Values are given as mean (standard deviation). SCI: spinal cord injury. |
Fig. 1. Common carotid artery intima media thickness in physically active persons with spinal cord injury (SCI) and age-matched able-bodied controls
Fig. 2. Carotid β stiffness in physically active persons with spinal cord injury (SCI) and age-matched able-bodied controls.
Fig. 3. Median and interquartile range of augmentation index in physically active persons with spinal cord injury (SCI) and age-matched able-bodied controls (p = NS).
DISCUSSION
Our data show that carotid IMT, arterial compliance, β stiffness and AIx, all indices of large artery structure and function, were similar in physically active persons with SCI and age-matched able-bodied group. These results indicate that regular exercise participation in persons with SCI may be associated with favorable effects on the elastic properties of large arteries. To our knowledge, there are no studies of carotid IMT and stiffness in persons with SCI.
Cardiovascular disease is a leading cause of death in persons with SCI and individuals with SCI are more likely to become obese, acquire metabolic syndrome, smoke, and be physically inactive, all of which all contribute to adverse vascular effects. Carotid IMT, arterial stiffness and AIx are associated with cardiovascular risk factors such as smoking, metabolic syndrome, physical activity and increased risk of cardiovascular disease (3). However, lifestyle modification, such as aerobic exercise, appears to prevent and possibly reverse age-related increases in arterial function and wave reflection in able-bodied individuals (14). Due to a clustering of cardiovascular risk factors, such as autonomic dysfunction, increased prevalence of hypertension and a sedentary lifestyle (2), it is possible that sedentary persons with SCI have increases in carotid IMT and arterial stiffness at an early age. This was supported by Wecht et al. (11), who found that physically inactive persons with SCI had 16% greater arterial stiffness than matched able-bodied persons. Also, Orakzai et al. (5) reported that mean calcium score of inactive individuals with SCI was significantly greater than the control group. However, neither study examined active persons with SCI. Our results showed that physically active persons with SCI had similar sub-clinical atherosclerotic markers compared with aged-matched able-bodied persons, suggesting a protective role for physical activity.
Although the mechanisms underlying the effects of exercise training on reductions in arterial stiffness and wave reflection are not known, several potential mechanisms have been suggested. Regular exercise is associated with improved cardiorespiratory fitness in persons with SCI (7). High cardiorespiratory fitness is related to increased endothelial function, reduced carotid IMT (6) and reduced arterial stiffness (15). Also, exercise participation in persons with SCI is associated with reduced blood pressure, lipid profiles, insulin resistance, and improved autonomic tone (7), all factors known to influence large artery thickness and arterial stiffness (16, 17).
Several limitations of the present study should be noted. In addition to the sample population being small, this cross-sectional study cannot determine causality. Further interventional studies are needed to understand the effects of carotid thickness and arterial stiffness in this population. Our participants with SCI were not a homogenous group with respect to injury. But as a first study to examine carotid IMT and aortic AIx in active persons with SCI, we do not feel that this heterogeneity detracts from the overall findings. Active individuals with SCI, irrespective of injury classification, do not differ from able-body individuals with respect to arterial structure and function.
All of our subjects were exercise-trained and the results may not be generalized to non-trained persons with SCI. We are unable to determine whether carotid IMT and stiffness are reduced in physically active persons with SCI compared with sedentary persons with SCI. Thus, it cannot be concluded that arterial structure and function is “normal” in physically active persons with SCI. It is possible that altered values reported in the literature in sedentary persons with SCI do not reflect pathology or pathophysiology, but rather an altered living condition. Thus, the indices of arterial structure and function reported herein may not be “normal” or “preserved” for active persons with SCI, but reflect an adaptation to training. Further studies are needed to clarify these issues in sedentary persons with SCI.
In conclusion, these data indicate that regular exercise in persons with SCI preserved central and systemic arterial function compared with aged-matched able-bodied participants. Our results suggest that regular exercise in persons with SCI has a favorable effect on large elastic artery thickness and arterial stiffness in this population.
REFERENCES
1. Garshick E, Kelley A, Cohen SA, Garrison A, Tun CG, Gagnon D, et al. A prospective assessment of mortality in chronic spinal cord injury. Spinal Cord 2005; 43: 408–416.
2. Myers J, Lee M, Kiratli J. Cardiovascular disease in spinal cord injury. Am J Phys Med Rehabil 2007; 86: 142–152.
3. Kullo IJ, Malik AR. Arterial ultrasonography and tonometry as adjuncts to cardiovascular risk stratification. J Am Coll Cardio 2007; 49: 1413–1426.
4. Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systemic review and meta-analysis. Circulation 2007; 115: 459–467.
5. Orakzai SH, Orakzai RH, Ahmadi N, Agrawal N, Bauman WA, Yee F, et al. Measurement of coronary artery calcification by electron beam computerized tomography in persons with chronic spinal cord injury: evidence for increased atherosclerotic burden. Spinal Cord 2007; 45: 775–779.
6. Lakka TA, Laukkanen JA, Rauramaa R, Salonen R, Lakka HM, Kaplan GA, Salonen JT. Cardiorespiratory fitness and the progression of carotid atherosclerosis in middle-aged men. Ann Intern Med 2001; 134: 12–20.
7. Jacobs PL, Nash MS. Exercise recommendations for individuals with spinal cord injury. Sports Med 2004; 34: 727–751.
8. Arnett DK, Evans GW, Riley WA. Arterial stiffness: a new cardiovascular risk factor? Am J Epidemiol 1994; 140: 669–682.
9. Seals DR. Habitual exercise and the age-associated decline in large artery compliance. Exerc Sport Sci Rev 2003; 31: 68–72.
10. Boreham CA, Ferreira I, Twisk JW, Gallagher AM, Savage MJ, Murray LJ. Cardiorespiratory fitness, physical activity, and arterial stiffness: the Northern Ireland Young Hearts Project. Hypertension. 2004; 44: 721–726.
11. Wecht JM, Weir JP, DeMeersman RE, Spungen AM, Bauman WA. Arterial stiffness in persons with paraplegia. J Spinal Cord Med 2004; 27: 255–259.
12. Wilkinson IB, MacCallum H, Flint L, Cockcroft JR, Newby DE, Webb DJ. The influence of heart rate on augmentation index and central arterial pressure in humans. J Physiol 2000; 525: 263–270.
13. Heffernan KS, Jae SY, Echols G, Lepine N, Fernhall B. Arterial stiffness and wave reflection following exercise in resistance trained men. Med Sci Sports Exerc 2007; 39: 842–848.
14. Tanaka H and Safar ME. Influence of lifestyle modification on arterial stiffness and wave reflections. Am J Hypertens 2005; 18: 137–144.
15. Binder J, Bailey KR, Seward JB, Squires RW, Kunihiro T, Hensrud DD, et al. Aortic augmentation index is inversely associated with cardiorespiratory fitness in men without known coronary heart disease. Am J Hypertens 2006; 19: 1019–1024.
16. Zieman SJ, Melenovsky V, Kass DA. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler Thromb Vasc Biol 2005; 25: 932–943.
17. Mancini GB, Dahlof B, Diez J. Surrogate markers for cardiovascular disease: structural markers. Circulation 2004; 109 Suppl 1: IV22–IV30.