OBJECTIVE: To determine changes in physical and social function during a prolonged preoperative waiting period and at 3 months after total knee arthroplasty.
SUBJECTS: Forty-three patients were evaluated on the day that surgery was decided, the day before surgery, and 3 months afterwards.
METHODS: Knee pain and function were assessed using a visual analogue scale and a functional assessment system. Isometric knee flexion extension strength and mobility were measured.
RESULTS: Knee pain and muscle strength remained unchanged during the mean waiting time of 10 (standard deviation 8) months. On the affected side, knee extension strength was 19% weaker than on the contralateral side and did not change pre-operatively. Post-operatively, knee pain decreased by 50%. Knee extension strength decreased by 26% and flexion strength by 12% compared with the initial assessments. Knee extension strength of the operated side was 42% lower than on the non-operated side. Knee flexion mobility was decreased by 8%, while the initially detected knee extension deficit of 10° (SD 7) remained unchanged. The functional assessment system did not detect any changes in function.
CONCLUSION: Waiting time did not affect knee pain or isometric knee extension/flexion strength. Three months post-operatively, knee pain had decreased significantly, but the strength of the operated knee was significantly lower than the pre-operative level.
Key words: osteoarthritis, knee arthroplasty, physical function, pain.
J Rehabil Med 2008; 40: 570–575
Correspondence address: Mirja Vuorenmaa, Department of Physical and Rehabilitation Medicine, Jyväskylä Central Hospital, Keskussairaalantie 19, FI-40620 Jyväskylä, Finland. E-mail: mirja.vuorenmaa@ksshp.fi
Submitted June 25, 2007; accepted March 4, 2008
Introduction
Osteoarthritis (OA) is a common joint disease that leads to a decrease in functional ability (1). In Finland, the prevalence of OA of the knee is approximately 5% among men and 7% among women (2). Primary osteoarthritis develops with age, whereas secondary arthritis is associated with underlying joint diseases, injury or growth disorders (3). Factors predisposing to OA of the knee are hereditary factors, overweight, female gender, excessive knee angle (valgus, varus), trauma to the knee, inflammatory joint diseases and heavy physical work (4, 5).
In its early stages OA of the knee causes pain during walking and in the later stages pain is present often at rest (6). As the disease progresses, the range of knee joint motion decreases, the joint becomes deformed and disability increases. OA leads to a reduction in thigh muscle strength (6–8). The conservative treatment options in the initial phases of OA are analgesic medication, physical therapies with cold and heat, electrotherapy, mobilization and acupuncture (3). Physical exercise has also been shown to improve the performance of activities of daily living (ADL) and to have a pain-relieving effect (1, 9, 10).
The decision to refer the patient for total knee arthroplasty (TKA) is based on knee pain, limited range of motion (ROM), deformity, degree of arthritis and limitation in physical function (11). In Finland, TKA was performed on 124/100,000 inhabitants in 2003 (12). At that time public health sector patients had to wait an average of one year for TKA surgery. Pre-operatively, poor knee joint ROM and high body mass index have been shown to be predictors of poor recovery after surgery at a 2-year follow-up (13).
Many studies have shown no increase in pain or deterioration in physical function in patients during a short preoperative waiting time ranging from 2 to 4 months (14–17). However, little is known about the effect of a longer waiting time on preoperative or early post-operative function.
Previous studies have mostly used subjective measures of pain and disability questionnaires. After joint replacement, recovery mostly occurs during the first 3 months (15, 18). The aim of this study was therefore to determine changes in patient’s subjective symptoms as well as objectively assessed knee function during a prolonged preoperative waiting period and short postoperative time of 3 months after TKA.
Patients and Methods
Subjects
A total of 60 patients referred for TKA were tested. Of these, 9 patients were not operated on during the 2 data collection periods and thus were excluded (4 patients decided not to have surgery and 5 had their surgery rescheduled). Of the 51 operated patients 43 (84%) returned for follow-up measurements at 3 months post-operatively. Of the 8 patients lost to follow-up, one had died, one knee prosthesis became infected, and 6 declined a check-up visit despite personal telephone contact. The demographic and clinical data of the excluded patients did not differ from those of the other subjects, except that dropouts reported shorter duration of knee pain. The majority of the subjects were women (86%) and the mean age of the subjects was 70 (standard deviation (SD) 5) years (Table I). The inclusion criterion for the study was OA of the knee rating 3–4 in the Ahlbäck classification (19). Exclusion criteria were age over 80 years, inflammatory joint disease, early knee arthroplasty and medically diagnosed serious disease, such as cancer. The study plan was approved by the ethics committee of the Central Finland Hospital District.
| Table I. Baseline demographics and clinical data of knee replacement patients |
| Variables | Complete cases n = 43 | Drop-out cases n = 8 | All n = 51 |
| Females, n (%) | 37 (86) | 4 (50) | 41 (80) |
| Age, years, mean (SD) | 70 (5) | 71 (3) | 70 (5) |
| Body mass index, kg/cm2 ,
mean (SD) | 31 (5) | 30 (4) | 31 (5) |
| Duration of knee pain, months, median (IQR) | 45 (20, 61) | 13 (10, 36) | 36 (14, 60) |
| Knee pain in VAS, mm,
median (IQR) | 56 (45, 72) | 61 (55, 69) | 60 (50, 70) |
| Arthrosis |
| Grade III, (%) | 9 (21) | 3 (38) | 12 (24) |
| Grade IV, (%) | 34 (79) | 5 (62) | 39 (76) |
| Duration of waiting list, months, median (IQR) | 8 (4, 14) | 19 (10, 23) | 8 (5, 17) |
| SD: standard deviation; IQR: interquartile range; VAS: visual analogue scale. |
Methods
Pain and function. Physical and social disability, as well as pain, were assessed using the modified functional assessment system (FAS), which has been validated for the evaluation of lower-extremity dysfunction in patients undergoing knee or hip replacement surgery (20, 21). The scale consists of 20 variables divided into 5 different sections: hip function, knee function, physical disability, social disability and pain (Table II). Each variable is scored between 0 and 4 (0 = no difficulty, 4 = significant difficulty or inability to complete).
| Table II. Scoring of functional assessment system (FAS) of low extremity dysfunction |
| Variable | 0 | 1 | 2 | 3 | 4 |
| Hip flexion | > 100º | 85–95º | 70–80º | 50–65º | < 50º |
| Extension deficit, hip | No deficit | 5º | 10º | 15º | > 15° |
| Abduction, hip | > 15º | 15º | 10º | 5º | 0° |
| Adduction, hip | > 15º | 15º | 10º | 5º | 0° |
| Knee flexion | > 115º | 100–110º | 85–95º | 70–80º | < 65° |
| Extension deficit, knee | No deficit | 5º | 10º | 15º | > 15° |
| Raising up from half-standing, cm | > 25 | 15–25 | 10–14 | 5–9 | < 5 |
| Raising up/sitting down, cm | 35 | 40 | 45 (ordinary chair) | 50 | > 55 |
| Step height, cm | 45 (tractor) | 40 (ordinary car) | 23 (bus, train) | 17 (stairs) | < 10 |
| Standing on one leg, sec | 40–60 | 25–39 | 15–24 | 5–14 | < 5 |
| Stair climbing | Full performance | One support, healthy
leg first | 2 support, healthy leg first | Personal solution, backwards | Unable |
| Gait speeds, m/sec | > 1.4 | 1.0–1.3 | 0.7–0.9 | 0.5–0.6 | < 0.5 |
| Walking aid | 0 | 2 sticks or crutches | Rolling walker | Gait chair | Unable to walk |
| Communication/transport | No restriction | Can drive a car, difficulties with bus, train | In car, cannot use anything else | In car with company | Handicap transportation |
| Work/housekeeping | No restriction | Can perform everything, but with pain | Work half-time, some help at home | Cannot work, some help at home | Help with everything |
| ADL-functions, other | No restriction | Needs to sit in all ADL-functions | Needs aids for stockings and shoes, cannot manage pedicure | Needs external help with stockings and shoes | Help with everything |
| Leisure time/hobbies | No restriction | Can do everything but with more pain | Can do 50% activities | Serious reduction of activities | Total reduction
in activities |
| Pain | No pain | Pain in load situation | Pain at rest | Pain at load and at rest | Permanent pain |
| Score 0–4: 0 = no difficulty, 4 = significant difficulty, unability to complete. ADL: activities of daily living. |
Muscle strength measurements. Isometric knee flexion and extension strength were measured at 80° knee flexion and 70° hip flexion using the David-200 dynamometer (Outokumpu, Finland) (22). Three submaximal warm-up sessions were performed before testing. The highest value of 3 maximal attempts in both directions was taken for analysis. The strength of the non-operative limb was measured first. Intensity of knee pain experienced both during the strength testing and during the previous week were assessed using a visual analogue scale (VAS; 0–100 mm) (23).
The initial measurements were performed at the orthopaedic outpatient clinic on the same day as the surgery assessment decision was made. The follow-up measurements were performed on the day before surgery and at 3 months after surgery. Two experienced physiotherapists jointly performed all the measurements. The same physiotherapist made the initial and follow-up measurements for each patient.
Surgical procedure. Surgery was performed under spinal or general anaesthesia. A mid-sagittal incision of the knee was performed and the medial parapatellar opening of the joint was used. The anterior cruciate ligament, meniscae and possible osteophytes were removed. The femoral and tibial bone cuts were performed with the help of appropriate jigs, and fitting with a trial prosthesis was performed before fixation of the final prosthesis components (AGC® Biomet, Warsaw, IL, USA) with cement. The same 2 surgeons performed all the operations.
Physiotherapy. When the decision in favour of operative treatment had been made, the patients received written instructions advising them to maintain themselves in good general condition and to maintain a good range of knee motion. In the surgical department on the day before surgery the patients were instructed on exercises to stimulate lower limb circulation, rising from bed and the use of churches. Postoperatively, in the orthopaedic ward, a continuous passive motion (CPM) machine was used 2–3 times per day for 0.5–1 h (24) at a time during the patients’ hospital stay, which varied between 5 and 7 days.
Isometric thigh exercises in sitting and prone lying, the straight leg raise exercise, gait re-education and cold treatment were started on the day after surgery. Patients received individual physiotherapy sessions 2–3 times per day, depending on need. On discharge home or to the ward of a local health centre, the patients received a written exercise programme. This included knee motion exercises and exercises to increase/maintain muscle activation using the weight of the leg as the resistance, knee flexion exercise, passive extension and knee extensor exercises as well as hip abduction and extension exercises in standing. These were recommended to be performed with 10–15 repetitions, 1–2 times per day. Patients were allowed to take a full weight-bearing or as much as tolerated on the operated leg, but for personal safety were recommended to use crutches after the operation for up to 6 weeks.
Statistical methods
The results are expressed as means or medians with SD, interquartile ranges (IQR), or 95% confidence intervals (95% CI). CI for the items of FAS index means were obtained by bootstrapping (1000 replications) method. The normality of variables was evaluated with the Shapiro-Wilk statistic. Statistical comparison between the operated and non-operated sides was made using the Mann-Whitney U test, analysis of variance (ANOVA) and Permutation test with Hommel’s adjustment. Correlation coefficients were calculated by the Pearson method. The α level was set at 0.05 for all tests.
Results
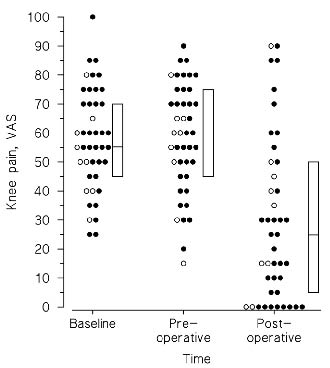
Mean waiting time from decision to time of surgery was 10 (SD 8) months (Table I). Knee pain on the operated side was 58 (SD 18) mm and did not change between the initial and pre-operative assessments. Postoperatively, pain decreased significantly to 29 (SD 28) mm (p < 0.001). No correlation was observed between degree of diagnosed OA and pain experienced at the different follow-ups (Fig. 1).
Fig. 1. Median (interquartile range) knee pain during the week before check-up time in grade III and IV of arthrosis (open dots = grade III, filled dots = grade IV). VAS: visual analogue scale.
At the initial assessment the extension strength of the operative knee was 19% weaker than that of the non-operative knee (p > 0.001). Knee flexion strength did not show side differences (Table III). Three months after surgery the extension strength of the operated knee was 26% (p = 0.001) weaker than at the initial assessment and 42% weaker than that of the non-operated knee (p < 0.001). The flexion strength of the operated knee had weakened by 12% (p = 0.037) from the initial assessment. At the initial assessment during the extension strength testing, the pain experienced in the operative knee was significantly higher than that in the non-operative knee (Table III). The pain experienced during testing at 3 months after surgery was clearly lower, but was still greater on the operated than non-operated side in both extension and flexion strength. Pain during testing was inversely correlated with extension strength (r = –0.37; 95% CI –0.61 to –0.07) and flexion strength (r = –0.44; 95% CI –0.66 to –0.15) at 3 months post-operatively.
| Table III. Isometric knee strength and pain during the strength measurements |
| | Baseline | Change from baseline to preoperative check-up | Change from baseline to
3 months postoperative check-up | Difference between the legs at 3 months |
| Operative knee Mean (SD) | Non-operative knee Mean (SD) | Operative
knee Mean (95% CI) | Non-operative knee Mean (95% CI) | Operated
knee
Mean (95% CI) | Non-operated knee Mean (95% CI) | p-value |
| Isometric knee strength (N) |
| Extension | 186 (90) | 231 (119) | –5 (–18 to 8) | 1 (–9 to 10) | –48 (–66 to –30) | 5 (–13 to 24) | 0.001 |
| Flexion | 90 (36) | 96 (44) | 0 (–8 to 8) | 1 (–7 to 8) | –10 (–20 to –1) | 1 (–9 to 10) | < 0.001 |
| Pain during the trial (VAS, mm) |
| Extension | 34 (24)* | 19 (22)* | 1 (–6 to 8) | 5 (–10 to 2) | –7 (–16 to 2) | –8 (–16 to –2) | 0.003 |
| Flexion | 21 (24) | 17 (20) | –11 (–20 to –0) | –5 (–10 to 0) | –5 (–13 to –3) | –8 (–16 to 1) | < 0.001 |
| *Difference between the legs at baseline (p = 0.001). SD: standard deviation; 95% CI: 95% confidence interval; VAS: visual analogue scale. |
Gait speed did not change at follow-up: at the initial assessment it was 1.1 (SD 0.4) m/sec and at 3 months postoperatively 1.2 (SD 0.4) m/sec. On the operated side mean single leg stance time was 5.6 (SD 6.6) sec preoperatively and 10.3 (SD 14.7) sec postoperatively (p = 0.013). The extension strength of the operated knee correlated with measured gait speed (r = 0.48–0.70, p = 0.002–0.001), single leg stance time (r = 0.35–0.39, p = 0.029–0.013) and stride height (r = 0.45–0.64, p = 0.004–0.001) at each check-up.
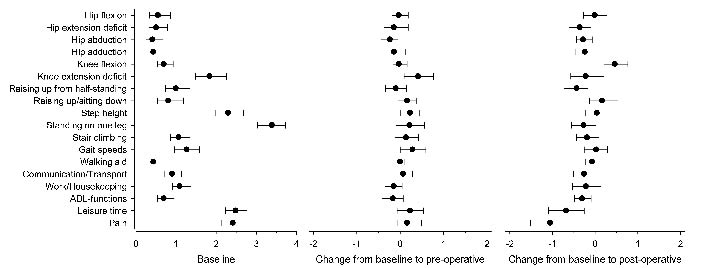
According to the FAS, the greatest problem experienced at the baseline assessment was maintaining balance (Fig. 2). At follow-up the changes in functional abilities were small (mean change < 1). Three months postoperatively, pain on the FAS scale was lower, while mean knee flexion movement had decreased from 112 (SD 12)° to 103 (SD 13)° (p = 0.031). Knee extension deficit at the initial assessment was 10 (SD 7)° and this did not change at follow-up.
Discussion
During the prolonged preoperative waiting period no significant changes took place in pain or in the objective functional measurements of knee muscle strength and mobility, showing that the delay in receiving surgery did not further reduce knee function in these patients. Previous studies have found that a preoperative waiting period of 2.5–4.5 months did not decrease subjectively perceived physical function or health-related quality of life in joint replacement patients (15–17, 25). The patients in the present study had had symptoms for almost 4 years before the decision to operate was made. These patients might have postponed surgery for personal reasons. They may have had deficits in function and muscle strength for a long time before the orthopaedic assessment, as some studies have shown (4, 6, 8).
Three months postoperatively average pain during the previous week was 50% less than at baseline, which result is consistent with earlier findings (26–30). A pain level of above 30 mm on the VAS is classified as moderate pain, and in some cases such patients need pain killers, while a pain level of under 30 mm is classified as mild pain, i.e. pain that does not interfere with the ability to perform ADLs (31). In 58% of the patients mild pain was reported and 23% of patients reported no pain at all. Nevertheless, moderate or severe pain was reported in 20% of the cases.
The changes in functional activities measured on the FAS at follow-up were minor. The inter-tester reliability of the FAS has been reported to be good (0.99–1.00) and its content and face validity have been shown to be excellent (20). The responsiveness of the FAS has not been studied. As seen in Fig. 2, the majority of patients score were 0 or 1 on the FAS in baseline. We do not know if the patients improved their function between baseline/pre-operative to 3 months post-operative, because our method (the FAS) seems insensitive to improvements in our population of patients.
Fig. 2. Means of functional assessment system with 95% CI at the baseline and changes both from baseline to pre-operative (10-month) and to post-operative (3-month) follow-ups. ADL: activities of daily living; 95% CI: 95% confidence interval.
We chose follow-up-time of 3 months to allow healing of the wound and soft-tissue. Earlier studies have shown that most of the improvement occurs within the first 3 months after the operation (15, 32, 33).
People may estimate their mobility higher by self-reported questionnaires than has been found by objective physical function tests (34). In these patients positive self-report may be an effect of the pain relief experienced after the knee arthroplasty. Thus, it is important to include objective measurements in follow-up studies and not self-reported questionnaires alone. Knee ROM, both toward flexion and extension at 3 months postoperatively was lower than the preoperative level. Previous studies have also reported a 5–15° decrease in knee flexion at follow-up during 2–6 months after surgery (28–30, 35–37). Conservatively treated individuals with OA have been shown to use a smaller knee angle in ADL performance than healthy controls due to pain and stiffness (38–39). Different ADLs require a wide ROM of the knee joint. Knee flexion needs in humans are: for walking 65–70°, for ascending stairs 84°, for descending stairs 90°, and for sitting 90°. Tying shoelaces and rising from a chair are possible with approximately 105° knee flexion (40). Changes in mobility may also lead to abnormal posture and cause compensatory hip movement. Therefore, owing to impaired knee mobility, our subjects would have been expected to encounter difficulties in some ADLs 3 months after surgery. However, the FAS assessment applied was not sensitive enough to detect these disabilities.
In this study preoperatively measured flexion and extension strength on the operative side were lower than on the non-operative side. Previous studies have demonstrated similar findings; flexion strength on the operated side has been 25–34% weaker and extension strength 24–41% weaker than on the non-operated side (33, 41). In the study by Lamb & Frost (42) lower limb leg press strength on the operative side was pre-
operatively 31% weaker than in the contra-lateral limb. However, preoperative physiotherapy or exercise has not been shown to improve recovery after surgery in studies with follow-up times of between 3 months and 2 years (26, 35, 43, 44).
The results of our study are consistent with earlier reports showing 26–40% lower knee extension and flexion strength levels 3 months post-surgery (27, 41, 42, 45–49). Pain may prevent optimal muscle activation (50). Also in the present study, pain experienced at the time of strength testing continued to be associated with thigh strength after surgery. As muscle strength weakens, much of the patient’s strength reserve is used in performing ADLs. Even a minor additional disease or bed rest can reduce strength reserve to a level that prevents independent coping. Older persons may use up to 97% of their maximal strength when rising from a chair (51). Difficulties in rising from a chair have been reported when knee extension strength is less than 10 kg and hip flexor strength less than 15 kg (52). It is not possible to fully recover from the operation in 3 months. Retraining muscle strength after disuse takes long time and without specific training often remains incomplete (53–55).
Knee flexor and extensor strength levels affect gait speed and prosthesis loading (49, 50, 53, 54). It has been reported previously that arthroplasty patients’ gait speed is reduced by 15–20%, and does not fully return within one year after surgery (39, 46, 56, 57). In this study gait speed was low preoperatively and no significant changes were found in gait speed or balance at follow-up. The risk of falling was probably still high, as a short single leg stance time correlates with an increased risk of falling (58). The risk of falling is also increased in instances where there is a need to walk at near maximal speeds, such as at traffic lights where the average gait speed required is 1.4 m/sec (59), which, on average, the present patients did not have.
On discharge from hospital patients received instructions on strengthening exercises, using their own leg weight as a resistance, and knee motion exercises, as well as advice to return to normal daily activities, which were not sufficient to restore knee function to the pre-operative level. To achieve this, progressive strength training would be needed. Studies with long-term follow-up are needed to determine the effectiveness of more active rehabilitation after knee arthroplasty.
In conclusion, patients had considerable pain and dysfunction at the time that the operation decision was made. Waiting time did not affect knee pain or isometric knee extension/flexion strength. Three months post-operatively, knee pain had decreased significantly, but the strength of the operated knee was significantly lower than the pre-operative level.
Acknowledgement
This study was supported by the Medical Research Fund of Jyväskylä Central Hospital
References
1. Maurer BT, Stern AG, Kinossian B, Cook KD, Schumacher HR. Osteoarthritis of the knee: isokinetic quadriceps exercise versus an educational intervention. Arch Phys Med Rehabil 1999; 80: 1239–1299.
2. Manninen P, Heliövaara M, Riihimäki, H, Suomalainen 0. Physical workload and risk of severe knee osteoarthritis. Scand J Work Environ Health 2002; 28: 25–32.
3. Marks R, Allegrante JP. Non-operative management of osteoarthritis. Critical Rev Phys Rehabil Med 2001; 13: 131–158.
4. Slemeda C, Brandt KD, Heilman DK, Mazzuca S, Braunstein EM, Katz BP, Wolinsky FD. Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med 1997; 127: 97–104.
5. Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arth Rheum 1998; 41: 1343–1355.
6. Hall MC, Mockett SP, Doherty M. Relative impact of radiographic osteoarthritis and pain on quadriceps strength, proprioception, static postural sway and lower limb function. Ann Rheum Dis 2006; 65: 865–870.
7. Steultjens MPM, Dekker J, van Baar ME, Oostenrdop RAB, Bijlsma JWJ. Range of joint motion and disability in patients with osteoarthritis of knee or hip. Rheumatology (Oxford) 2000; 39: 955–961.
8. O’Reilly SC, Jones A, Muir KR, Doherty M. Quadriceps weakness in knee osteoarthritis: The effect on pain and disability. Ann Rheum Dis 1998; 57: 588–594.
9. Ettinger WH, Burns R, Messier SP, Applegate W, Rejeski WJ, Morgan T, et al. Randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. The fitness arthritis and seniors trial (FAST). JAMA 1997; 277: 25–31.
10. Barker KB, Nelson ME, Felson DT, Layne JE, Sarno R, Roubenoff R. The efficacy of home based progressive strength training in older adults with knee osteoarthritis: a randomized controlled trial. J Rheumatol 2001; 28: 1655–1665.
11. Dieppe P, Basler H-D, Chard J, Croft P, Dixon J, Hurley M, et al. Knee replacement surgery for osteoarthritis: effectiveness, practice variations, indications and possible determinants of utilization. Rheumatology 1999; 33: 73–83.
12. Nevalainen J, Keinonen A, Mäkelä A, editors. The 2002–2003 implant yearbook on orthopaedic endoprothesis. Finnish Arthroplasty Register. 2005 Publications of National Agency for Medicine 1/2005. Helsinki: National Agency of Medicine.
13. Lizaur A, Marco L, Cebrian R. Preoperative factors influencing the range of movement after total knee arthroplasty for severe osteoarthritis. J Bone Joint Surg 1997; 79: 626–629.
14. Kelly KD, Voaklander DC, Johnston DW, Newman SC, Suarez-Almazor ME. Change in pain and function while waiting for major joint arthroplasty. J Arthroplasty 2001; 16: 351–359.
15. Nilsdotter AK, Lohmander LS. Age and waiting time as predictors of outcome after total hip replacement for osteoarthritis. Rheumatology (Oxford) 2002; 41: 1261–127.
16. Hirvonen J, Blom M, Tuominen U, Seitsalo S, Lehto M, Paavolainen P, et al. Health-related quality of life in patients waiting for major joint replacement. A comparison between patients and population controls. Health Quality Life Outcomes 2006; 4: 3.
17. Kapstad H, Rustøen T, Hanestad BR, Moum T, Langeland N, Stavem K. Changes in pain, stiffness and physical function in patients with osteoarthritis waiting for hip or knee joint replacement surgery. Osteoarthritis Cartilage 2007; 15: 837–843.
18. Kramer JF, Speechley M, Bourne R, Rorabeck C, Vaz M. Comparison of clinic- and home-based rehabilitation programs after total knee arthroplasty. Clin Orthop Relat Res 2003; 410: 225–223.
19. Ahlbäck S. Osteoarthrosis of the knee. Radiographic investigation. Acta Radiol Diagn 1968; Suppl 277: 7–72.
20. Öberg U, Öberg B, Öberg T. Validity and reliability of new assessment of lower- extremity dysfunction. Phys Ther 1994; 74: 861–871.
21. Öberg U. Functional Assessment System of lower-extremity dysfunction. Linköping University Medical Dissertations No 485. 1996. Department of Orthopaedic Surgery, Department of Caring Sciences Linköping University, Linköping, Sweden.
22. Häkkinen K, Komi P, Kauhanen H. Scientific evaluation of specific loading of the knee extensors with variable resistance, isokinetic and barbell exercises. In: Marconnet P, Komi P, editors. Medicine and Sport Science. Basel: Karger AB; 1987, p. 224–327.
23. Dixon S, Birth H. Reproducibility along a 10 cm visual analogue scale. Ann Rheum Dis 1981; 40: 87–89.
24. Gose JC. Continuous passive motion in the postoperative treatment of patients with total knee replacement. A retrospective study. Phys Ther 1987; 67: 39–42.
25. Kelly KD, Voaklander DC, Johnston WC, Suarez-Almazor ME. Equity in waiting times for major joint arthroplasty. Can J Surg 2002; 45: 269–276
26. D’ Lima JA, Colwell C, Beverly A, Morris RN, Hardwick RN, Kozin F. The effect of preoperative exercise on total knee replacement outcomes. Clin Orthop Relat Res 1995; 326: 174–182.
27. Rissanen P, Aro S, Slätis P, Sintonen H, Paavolainen P. Health and quality of life before and after hip or knee arthroplasty. J Arthroplasty 1995; 10: 169–175.
28. Block JE, Westlake SM, Meredith LM, Sheppard MS. Total knee arthroplasty: the effect of early discharge on outcome at 6–8 weeks postoperative. Physiother Can 1999; 51: 45–51.
29. Perhonen M. Komi PV, Häkkinen K, von Bonsdorff H, Partio E. Strength training and neuromuscular function in elderly people with total knee endoprosthesis. Scand J Med Sci Sports 1992; 2: 234–243.
30. Mizner RL, Petterson SC, Stevens JE, Axe MJ, Snyder-Mackler L. Preoperative quadriceps strength predicts functional ability one year after total knee arthroplasty. J Rheumatol 2005; 32: 1533–1539.
31. Collins LS, Moore AR, Mcquay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain 1997; 72: 95–97.
32. Shields RK, Enloe LJ, Leo KC. Health related quality of life in patients with total hip or knee replacement. Arch Phys Med Rehabil 1999; 80: 572–579.
33. Kennedy DM, Stratford PW, Hanna SE, Wessel J, Gollish JD. Modeling early recovery of physical function following hip and knee arthroplasty. BMC Musculoskelet Disord 2006; 7: 100.
34. Walker DJ, Heslop PS, Chandler C, Pinder IM. Measured ambulation and self-reported health status following total joint replacement for the osteoarthritic knee. Rheumatology 2002; 41: 755–758.
35. Lorentzen JS, Petersen MM, Brot C, Madsen O. Early changes in muscle strength after total knee arthroplasty. Acta Orthop Scand 1999; 70: 176–117.
36. Rodgers JA, Carvin G, Walker CW, Morford RN, Urban J, Bedard J. Preoperative physical therapy on primary total knee arthroplasty. J Arthroplasty 1998; 13: 414–421.
37. Beaupre LA, Davies DM, Jones CA, Ginats JG. Exercise combined with continuous passive motion or slider broad therapy compared with exercise only: a randomized trial of patients following total knee arthroplasty. Phys Ther 2001; 81: 1029–1037.
38. Walker CRC, Myles C, Nutton R, Rowe P. Movement of the knee in osteoarthritis. J Bone Joint Surg 2001; 83: 195–198.
39. Ouellet D, Moffet H. Locomotor deficits before and two months after knee arthroplasty. Arthritis Rheum 2002; 47: 484–493.
40. Laubenthal KN, Smidt GL, Kettekamp DB. A quantative analysis of knee motion during activities of daily living. Phys Ther 1972; 52: 34–43.
41. Berman AT, Basacco SJ, Israelite C. Evaluation of total knee arthroplasty using isokinetics testing. Clin Orthop Relat Res 1991; 271: 106–113.
42. Lamb SE, Frost H. Recovery of mobility after knee arthroplasty, expected rates and influencing factors. J Arthroplasty 2003; 18: 575–582.
43. Weidenheilm L, Mattson E, Broström L-Å, Wersäll-Robertsson E. Effect of preoperative physiotherapy in unicompartmental prosthetic knee replacement. Scand J Rehabil Med 1993; 25: 33–39.
44. Beaupre LA, Lier D, Davies DM, Johnston DBC. Effect of a preoperative exercise and education program on functional recovery, health related quality of life, and health service utilization following primary total knee arthroplasty. J Rheumatol 2004; 31: 1166–1173.
45. Huang C-H, Cheng C-K, Lee Y-T, Lee K-S. Muscle strength after successful total knee replacement. A 6–13-year follow-up. Clin Orthop Relat Res 1996; 328: 147–154.
46. Walsh M, Woodhouse LJ, Thomas SG, Finch E. Physical impairments and functional limitations: a comparison of individuals 1 year after total knee arthroplasty with control subjects. Phys Ther 1998; 78: 248–258.
47. Berth A, Urbach D, Awiszus F. Improvement of voluntary quadriceps muscle activation after total knee arthroplasty. Arch Phys Med Rehabil 2002; 83: 1432–1436.
48. Silva M, Shepherd EF, Jackson WO, Pratt JA, McClung CD, Schmalzied TP. Knee strength after total knee arthroplasty. J Arthroplasty 2003; 18: 605–611.
49. Rossi MD, Hasson S. Lower-limb force production in individuals after unilateral total knee arthroplasty. Arch Phys Med Rehabil 2004; 85: 1279–1284.
50. Stokes M, Young A. The contribution of reflex inhibition to arthrogenous muscle weakness. Clinic Sci 1984; 67: 7–14.
51. Hughes MA, Myers S, Schenkman ML. The role of strength in rising from a chair in the functionally impaired elderly. J Biomechanics 1996; 12: 1509–1513.
52. Ferrucci L, Guralnik JM, Buchner D, Kasper J, Lamb SE, Simonsick
EM, et al. Departures from linearity in the relationship between measures of muscular strength and physical performance of the lower extremities: the women’s health and aging study. J Gerontol A Biol Sci Med Sci 1997; 52: M275–285.
53. Stevens JE, Mizner RL, Snyder-Macler L. Quadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritis. J Orthop Res 2003; 21: 775–779.
54. Jones AC, Voaklander DC, Suarez-Almazor ME. Determinants of function after total knee arthroplasty. Phys Ther 2003; 83: 696–706.
55. Kannus P, Jozsa L, Renström P, Järvinen M, Kvist M, Lehto M, et al. The effects of training, immobilisation and remobilisation on musculoskeletal tissue. 2. Remobilization and prevention of immobilisation atrophy. Scand J Med Sci Sports 1992; 2: 164–176.
56. Bohannon RW. Comfortable and maximum walking speed of adults aged 20–79 years: reference values and determinants. Age Ageing 1997; 26: 15–19.
57. Fuchas S, Frisse D, Laas H, Thorwesten L, Tibesku CO. Muscle strength in patients with unicompartmental arthroplasty. Am J Phys Med Rehabil 2004; 83: 650–654.
58. Vellas B, Romeo L, Baumgartner R, Rubenstain L, Garry P. One-leg balance is an important predictor of injurious falls on older persons. J Amer Geriatr Society 1997; 45: 735–738.
59. Avlund K, Schroll M, Davidsen M, Loborg B, Rantanen T. Maximal isometric muscle strength and functional ability in daily activities among 75-years old men and women. Scand J Med Sci Sports 1994; 4: 34–40.