OBJECTIVE: We studied balance control in patients with cervical spondylosis, on the hypothesis that ataxia and changes in postural responses occur concurrently as a consequence of structural problems in the cervical cord.
Subjects and patients: Seventeen patients and 17 healthy subjects were recruited. Based on magnetic resonance imaging, the patients were divided into 2 groups, with (n = 9) and without (n = 8) signs of myelopathy.
METHODS: Body sway was recorded under quiet stance on a force platform. Postural perturbations evoked early and late responses in soleus and tibialis anterior.
RESULTS: Most patients showed increased body sway during stance, which was larger in cervical spondylosis with myelopathy than cervical spondylosis. Early postural responses in the soleus were not affected. Late responses in soleus and tibialis anterior were delayed in cervical spondylosis with myelopathy. Across all patients, latency of tibialis anterior late response was correlated with lower limb sensory impairment and amplitude of body sway.
CONCLUSION: Abnormal transmission through the cervical cord of proprioceptive input to supraspinal centres and of descending commands to caudal cord levels are accountable for ataxia in cervical spondylosis with myelopathy. Stabilometry may be an economic and easy way in a clinical and rehabilitative setting to distinguish severe from mild forms of cervical spondylosis prior to physical treatment and to help the differential diagnosis from other diseases featuring similar signs.
Key words: ataxia, myelopathy, cervical spinal cord, posture, long-loop, EMG.
J Rehabil Med 2008; 40: 539–547
Correspondence address: Antonio Nardone, Posture and Movement Laboratory, Division of Physical Therapy and Rehabilitation, Scientific Institute of Veruno, Salvatore Maugeri Foundation (IRCSS), Via Revislate 13, IT-28010 Veruno (Novara), Italy. E-mail: antonio.nardone@fsm.it
Submitted October 2, 2007; accepted March 5, 2008
Introduction
Cervical spondylosis (CS) is a frequent clinical problem characterized by symptoms and signs consistent with cervical spine and spinal cord structural abnormalities. The pattern of symptoms and associated physical signs varies according to which structures are affected: radicular and myelopathic syndromes are produced by nerve root and spinal cord compression, respectively. In turn, cord compression can produce abnormal stimulation or conduction block of the nerve fibres travelling along the motor or sensory fascicles. Cervical spondylosis with myelopathy (CSM) may pose a challenge to differential diagnosis. For instance, when radiculopathy symptoms, such as pain at the cervical spine region or upper extremity paraesthesia, are negligible, but there is loss of upper limb fine motor function, muscle atrophy or paraparesis, it can be difficult to distinguish CSM from other diseases with clinical signs of “upper” motoneurone lesion or cervical “lower” motoneurone lesion.
CSM can affect several motor and sensory pathways travelling along the cord, including those conveying the postural command to the motoneurones and the proprioceptive input from the lower limbs to the supraspinal centres (1). Accordingly, the control of stance and the muscle responses to perturbations of posture can be affected in these patients. To our knowledge, however, no objective reports exist on the quality of stance in patients with CS and CSM. To what extent are these patients unstable? Are patients with CSM more or less unstable than patients affected by peripheral neuropathy? Is stance control different in diseases producing lower limb motor signs comparable to those observed in CSM, such as in other forms of spasticity? The answer to these questions may not be immediately apparent. For instance, recent studies have shown that spastic patients show no or negligible changes in balance control during quiet stance (2) in spite of the hyperactivity of their monosynaptic spinal reflex loop, which is usually considered to be relevant for stance control. On the other hand, patients with peripheral neuropathy do not necessarily show major postural unsteadiness if their deficit is limited to the largest myelinated fibres (3). A further related question is: if patients with CS are unstable, can simple postural tests dissect out patients with real cord compression and myelopathy from those without myelopathy or neck trouble of various origins (4–6)?
We report here the results of a study performed in patients with severe spondylosis with or without myelopathy and in normal subjects. We have tested the hypothesis that stance instability occurs in CS, and that it is connected with the abnormal function of the compressed nerve fibres travelling along the cord. Postural control has been assessed by means of a force platform upon which patients stood. In addition, balance-correcting responses have been also evoked in the leg muscles by delivering stance perturbations, since simple stabilometric measures alone may not necessarily give pathophysiological clues as to the nature of the presumed postural unsteadiness (3). Since perturbations evoke early and late electromyographic responses in leg muscles, the former being transmitted through segmental spinal circuits and the latter through long spinal and supraspinal pathways, we have hypothesized that the late, but not the early, response to perturbation would be delayed in CS patients with postural unsteadiness. This event would then contribute to explaining the potential unsteadiness in CSM, since the control of stance may rely, at least in part, on long-loop responses originating from leg muscle proprioceptors (2, 3).
Methods
Patients
We recruited 17 normal subjects, mean age 63.1 years (standard deviation (SD) 10.7), and 17 patients with cervical compression of degenerative origin (Table I), mean age 62.4 years (SD 9.6), who were admitted for a period of physical therapy treatment. All patients had cervical spondylosis and canal narrowing, with or without disc degeneration or herniation. Eight of them had undergone laminectomy. There were no concomitant non-degenerative diseases of the cervical vertebrae or other diseases of the cervical cord. Patients with other brain, thoracic spinal cord, cauda equina, or peripheral nerve disorders were excluded. All patients were able to walk unassisted. The normal subjects had no cervico-brachial pain or other symptoms and signs suggestive of cervical vertebrae or cord problems. All normal subjects and patients gave informed consent to participate in the study. The experiments were conducted according to the Declaration of Helsinki and approved by the local ethics committee.
| Table I. Clinical characteristics of the cervical spondylosis patients, without and with myelopathy |
| Patients | Sex | Age (years) | Ashwortha | Motricity Indexb | Quadriceps T reflexc | Achilles T reflexc | Plantar responsed | Sensory Score (NIS)e | Narrow spinal canal |
| Without myelopathy |
| 1 | M | 67 | 1.5 | 100 | 4 | 1 | 2 | 0 | C4–C6* |
| 2 | F | 74 | 1.5 | 67 | 2.5 | 2.5 | 2 | 0.5 | C3–C7 |
| 3 | M | 74 | 0 | 88 | 2 | 2 | 3 | 0 | C3–C4* |
| 4 | F | 61 | 2 | 76 | 3.5 | 3.5 | 2 | 3 | C3–C7 |
| 5 | M | 51 | 0 | 63 | 1.5 | 1 | 2 | 0 | C4–C7 |
| 6 | M | 49 | 1 | 100 | 3 | 3.5 | 2 | 0 | C3–C7* |
| 7 | F | 73 | 0 | 84 | 3 | 4 | 0 | 2 | C3–C5* |
| 8 | F | 52 | 1 | 84 | 3 | 3 | 2 | 1 | C4–C7 |
| Median | | 64.0 | 1.0 | 84.0 | 3.0 | 2.8 | 2.0 | 0.3 | |
| With myelopathyf |
| 9 | M | 67 | 0 | 67 | 2.5 | 0.5 | 1.5 | 3 | C2 |
| 10 | M | 69 | 1 | 43 | 2 | 1 | 2 | 6 | C4–C6* |
| 11 | M | 72 | 0 | 76 | 2.5 | 2.5 | 3 | 4 | C3–C4 |
| 12 | M | 51 | 3 | 53 | 4 | 3 | 0.5 | 4 | C4–C5 |
| 13 | M | 67 | 2.5 | 70 | 4 | 4 | 0 | 1 | C2* |
| 14 | M | 57 | 0 | 84 | 3 | 3 | 3 | 1 | C4–C7 |
| 15 | M | 60 | 2 | 76 | 3 | 3 | 0.5 | 2 | C6–C7 |
| 16 | F | 47 | 3 | 76 | 3 | 4 | 1 | 4 | C2–C3* |
| 17 | M | 70 | 1.5 | 74 | 3.5 | 3.5 | 1.5 | 3 | C3–C5* |
| Median | | 67.0 | 1.5 | 74.0 | 3.0 | 3.0 | 1.5 | 3.0 | |
| aModified Ashworth Scale: from 5 (rigid in flexion or extension) to 0 (no increase in muscle tone). bMotricity Index leg score: from 1 (no movement) to 100 (normal strength). cMyotatic Reflex Scale: from 0 (reflex absent) to 4 (reflex enhanced) (9). dPlantar Response (Norris scale): from 0 (Babinski sign) to 3 (normal flexor response) (10). eNeurological Impairment Score (NIS): from 2 to 0 (normal) per item (touch-pressure, pricking pain, vibration and joint position sense) (11). fPresence of myelopathy based on hyperintensity of T2-weighted images on magnetic resonance imaging. From a to e, the values are the average from both legs. Asterisk indicates patients who had undergone laminectomy. |
Clinical data
All patients had been evaluated clinically. Patients were diagnosed on the basis of symptoms and signs of cervical radiculopathy or myelopathy, including pain in the neck or arms and arm and leg dysfunction, e.g. loss of sensitivity in the hands and/or feet. Several patients had increased reflexes in the knee and ankle. Some patients presented with stance ataxia and gait unsteadiness in addition to spastic gait. In several patients, electromyography (EMG) and nerve conduction velocity studies had confirmed peripheral nerve problems at the upper limb.
All patients had received cervical spine X-rays and magnetic resonance imaging (MRI). Cervical MRI reports were scrutinized for signal changes on T2-weighted images at the level of spinal compression, which were considered signs of myelopathy (7). These were found in 9 patients. No signs of myelopathy were found in 8 patients, although 2 of these patients had dural sac impression. The T2-weighted image criterion was used in the data analysis to separate the patients into 2 groups (CS, without or with myelopathy, CSM). Somatosensory or motor evoked potentials were not performed to characterize the patients, because the results of these studies do not necessarily correlate with the dysfunction (8). In 10 patients (4 with CS, 6 with CSM), routine somatosensory evoked potentials (SEP) from the upper and lower limbs had been previously collected in another setting and were available in their clinical documentation.
Spastic hypertonus of the lower limbs was evaluated by the Ashworth scale. Muscle strength was expressed with the Motricity Index. Patellar and Achilles tendon reflexes were elicited and scored according to the Myotactic Reflex Scale (9). The plantar response (Babinski’s sign) was scored by the Norris scale (10) (Table I). Neurological signs were quantified by means of the Neurological Impairment Score (NIS) based on reports of sensation at the level of the great toe bilaterally (touch-pressure, vibration with a 128 Hz-tuning fork, joint position, pricking pain) (11). NIS score reported in Table I is the sum of the values attributed to each item.
Stabilometry
Subjects stood still for 51 sec on a force platform (Kistler, type 9281B, Switzerland) with feet spaced 10 cm apart. Each trial within a series was repeated twice, alternately with eyes open (EO), when subjects gazed at a target placed at a distance of 50 cm at eye level, and eyes closed (EC). The force signals were sampled at 10 Hz, and a program calculated the centre of foot pressure (CoP). From the instantaneous positions of CoP, the average position of CoP along the anteroposterior axis was calculated. CoP position was normalized as a percentage of the total foot length. Balance assessment was carried out by computing the sway path, i.e. the length of the path travelled by the CoP, computed as the distance between the coordinates of the successive acquired instantaneous CoP positions, and the sway area, i.e. the surface swept during the trial by the line joining the position of the mean CoP to the successive positions of the moving instantaneous CoP.
Leg muscle responses to postural perturbation
Subjects stood with EO on a tilting platform (Lomazzi & Co., Legnano, Italy). Perturbations consisted of 20–30 (depending on patient compliance) toe-up and toe-down rotations of 3° at 50°/sec. The interval between perturbations varied between 8 and 10 sec. Toe-up and toe-down rotations were presented in pseudo-random order, with a balance between the 2 types in each patient. The surface EMG was bilaterally recorded from soleus (Sol) and tibialis anterior (TA) muscles. EMG was amplified (× 10,000), band-pass filtered (100 Hz – 3 kHz, –6 dB/octave) and converted analogue-to-digital at 100 kHz. Signals were full-wave rectified and averaged.
Responses to toe-up rotations consisted of 2 successive EMG bursts (short-latency, SLR; medium-latency response, MLR) in the stretched Sol muscle. A late response in the TA muscle occurring after about 140 ms in normal subjects was termed antagonist reaction (AR) (12). Responses to toe-down rotations consisted of a MLR in the stretched TA and an AR in the Sol. The responses were identified on the superimposed traces of the rectified and averaged signals recorded from the muscles of the 2 legs. The onset of the responses was set at the time when the rectified and averaged EMG burst increased beyond 2 SDs of the mean value of the pre-stimulus activity (13, 14).
For normal subjects and patients, the area of the Sol and TA background activity was calculated within a 100-ms time-window prior to the platform perturbation. The area of the evoked Sol SLR and of the Sol and TA MLR was then measured from the onset to the end of the respective EMG burst. The area of the AR response of Sol and TA was calculated within a window lasting 80 ms after their onset.
Data analysis
For assessing differences in the clinical data, the Mann-Whitney U test between CS and CSM patients was run. For the stabilometric trials, we averaged the sway values from the 2 trials recorded for each visual condition in each subject. Logarithmic transformation of sway area and sway path was made before statistical analysis. Unless otherwise stated, values are expressed as means (SD) for each group. For each of these 3 variables (sway area, sway path and position of CoP), a two-way analysis of variance (ANOVA) with 3 subject groups (normal, CS, CSM) as independent variables and with visual condition (EO and EC) as repeated measures was performed. For the EMG responses to perturbation, prior to analysis, we averaged the mean values of latency and area from both legs. A one-way ANOVA between the 3 groups (normal, CS, CSM) was then performed for each response. Post-hoc comparisons were made using the Newman-Keuls post-hoc test. The software Statistica (StatSoft Inc, USA) was used for all statistical analyses.
Results
Patients were divided into 2 groups based on the presence of MRI signs of spinal cord lesion. The clinical findings for the 2 groups are reported in Table I. The median values of several of the reported variables did not differ between groups. However, there was a marginally inferior motor function (Motricity Index) (Mann-Whitney U test, p = 0.07) in the CSM group than in CS group. The NIS, calculated on the clinical sensory scores of the lower limb items, indicated a more severe sensory impairment in the CSM group (Mann-Whitney U test, p < 0.05). SEPs from the lower limbs were reported to be abnormal in 1 out of 4 patients of the CS group and in 2 out of the 6 tested patients of the CSM group.
Body balance on the stable platform
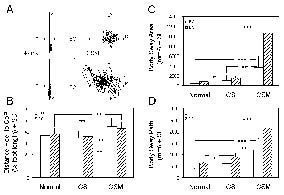
Fig. 1A shows examples of stabilometric recordings in a normal subject and in a patient with CSM during stance under EO and EC conditions. The large increase in body sway of the patient under both visual conditions, but particularly with EC, is obvious. In addition, under both visual conditions, the stabilogram was displaced to a more forward position in the patient with respect to the normal subject, a sign of forward inclination of the body.
Fig. 1B shows that the mean position of the CoP during quiet stance with EO and EC was more advanced in CSM patients than in those with CS or in the normal subjects. Two-way ANOVA on the CoP antero-posterior position with 3 groups (normal, CS and CSM) × 2 visual conditions (EO and EC) showed an effect of groups (F = 7.1, df = 2,30, p < 0.005) but not of vision; accordingly, no interaction between groups and vision was observed. The post-hoc test showed that no difference was present between normal subjects and patients with CS. Patients with CSM were more forward inclined than either normal subjects or patients with CS under both visual conditions (p < 0.005, for all comparisons).
Fig. 1C summarizes the mean values of body sway area under EO and EC in normal subjects and in the 2 patient groups. Two-way ANOVA showed that body sway area differed between the 3 groups (F = 15.5, df = 2,30, p < 0.0005) and between visual conditions (F = 61.9, df = 1,30, p < 0.0005) with an interaction between groups and vision (F = 7.4, df = 2,30, p < 0.005). The post-hoc test showed that the differences between groups were due to the increased body sway area of the patients with CS and CSM. Body sway area of CS patients was larger than in normal subjects (p < 0.05 for both EO and EC) but smaller than in CSM patients (EO, p < 0.005; EC, p < 0.0005).
Fig. 1D shows that body sway path behaved similarly to SA, the greater increase being found in the patients with CSM, although some increase was also found in patients with CS. Two-way ANOVA showed that body sway path differed between the 3 groups (F = 12.8, df = 2,30, p < 0.005) and between visual conditions (F = 55.8, df = 1,30, p < 0.0005); the group-vision interaction was not significant. The post-hoc test showed a difference in body sway path between normal subjects and patients with CS (p < 0.05 under both EO and EC). The patients with CSM showed a clearly increased body sway path with respect to both normal subjects (p < 0.0005 for both EO and EC) and CS patients (EO, p < 0.005; EC, p < 0.0005).
Fig. 1. (A) Stabilometric recordings during quiet stance with eyes open (EO) and eyes closed (EC) in a normal subject and a patient with cervical spondylosis with myelopathy (CSM). Direction of sway: A, anterior; P, posterior; L, left; R, right. (B) Distance between heel and centre of foot pressure (CoP), as percentage of foot length, in the groups of normal subjects, of patients with cervical spondylosis without (CS) and with myelopathy (CSM), under EO and EC conditions. The larger the heel-CoP distance, the more forward inclined the body. (C) Body sway area and (D) sway path in the same groups of normal subjects and patients, under both visual conditions. *p < 0.05; **p < 0.005; ***p < 0.0005. SD: standard deviation; SE: standard error.
Leg muscle responses to postural perturbations
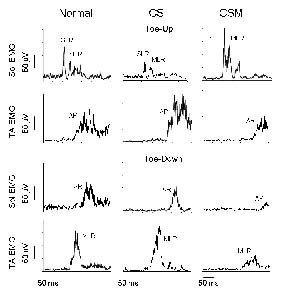
Typical averaged EMG responses of Sol and TA muscles to toe-up and toe-down platform rotations, obtained from a normal subject, a patient with CS and a patient with CSM, are reported in Fig. 2. In the normal subject, toe-up evoked a SLR and a MLR in Sol, followed by an AR in TA. Toe-down perturbation evoked a MLR in TA, followed by an AR in Sol. In the patient with CS, the pattern of EMG responses was similar to that of the normal subject during both toe-up and toe-down rotations. Conversely, in the patient with CSM, changes in both latency and amplitude of the TA MLR, Sol AR and TA AR were observed.
Fig. 2. Rectified and averaged (n = 20) electromyographic (EMG) traces of soleus (Sol) and tibialis anterior (TA) muscles during toe-up (upper 2 traces) and toe-down rotation (lower 2 traces) of the supporting platform, in a normal subject (left column), in a cervical spondylosis (CS) (middle column) and a cervical spondylosis with myelopathy (CSM) patient (right column). The vertical dashed lines indicate the onset of the platform movement. SLR: short-latency response; MLR: medium-latency response; AR: antagonist reaction.
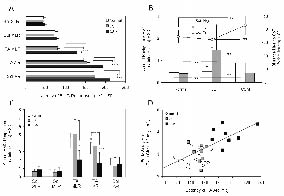
One-way ANOVA was separately performed on latency of each of the responses of both normal subjects and patients. ANOVA showed no difference in the latency of Sol SLR and MLR between groups (Fig. 3A). On the contrary, the latency of TA MLR and TA AR and of Sol AR differed between groups (TA MLR, F = 84.7, df = 2,31, p < 0.0005; TA AR, F = 30.8, df = 2,31, p = 0.0005; Sol AR, F = 14.8, df = 2,31, p < 0.0005). The post-hoc test showed that the latency of TA MLR was longer in patients with CSM than in either normal subjects or CS patients (p < 0.0005), while no difference was found between the 2 latter groups. The latency of both TA AR and of Sol AR were longer (p < 0.0005) in CSM patients than in either normal subjects or CS patients, the 2 latter groups again showing similar values.
The area of the background EMG activity during quiet stance and of the response bursts was also analysed (Fig. 3B). Sol background was different between groups (F = 8.2, df = 2,31, p < 0.005). In particular, it was larger (Newman-Keuls, p < 0.005) in patients with CSM than in normal subjects and patients with CS. TA background had the opposite configuration (F = 7.7, df = 2.31, p < 0.005), being larger in patients with CS than normal subjects and patients with CSM (Newman-Keuls, p < 0.005). This pattern was related to the body orientation in space, being the mean CoP minimally backward in CS but advanced in CSM patient groups with respect to normal subjects (Newman-Keuls, p < 0.005) (see Fig. 1B).
Fig. 3. (A) Onset latency and (C) area of Sol SLR, Sol MLR, TA AR to toe-up rotations, and of TA MLR and Sol AR to toe-down rotations in normal subjects, CS and CSM patients. *p < 0.05; ***p < 0.0005. (B) Area of the background activity of Sol and TA muscles, in the 100-ms period preceding the platform perturbation, in the 3 groups of subjects. (D) Relationship between body sway area with eyes closed and onset latency of TA AR. The line is fitted through the data points of all patients. Same labels as in Figs. 1 and 2. Sol: soleus; SLR: short-latency response; MLR: medium-latency response; TA: tibialis anterior; AR: antagonist reaction; CS: cervical spondylosis; CSM: cervical spondylosis with myelopathy. SD: standard deviation; EMG: electromyography.
The area of EMG bursts of Sol SLR, Sol MLR and Sol AR was not different between groups (Fig. 3C). On the contrary, the area of the TA MLR and TA AR were different (MLR, F = 4.6, df = 2.31, p < 0.05; AR, F = 8.1, df = 2.31, p = 0.005). TA MLR was larger in CS than in CSM patients (Newman-Keuls, p < 0.05). On the contrary, no difference was found between normal subjects and CS patients. TA AR behaved similarly to TA MLR, being larger in CS patients than in normal subjects (p < 0.05) or patients with CSM (p < 0.0005).
Relationship between response latencies and body sway
We searched for a correlation between sway area and latency of the muscle responses to perturbation (TA MLR, TA AR, Sol AR). While no relationship was found between sway area and TA MLR under either EO or EC (not shown), a positive correlation was found across the patients between sway area with EC and TA AR (y = 0.01x + 0.92, R2 = 0.41, p < 0.05) (Fig. 3D). A clear-cut separation appears between CSM and CS patients, the former showing the longest latencies of TA AR and correspondingly the largest sway area. One patient with CSM had a very long delay of the TA AR and was not able to stand upright with EC; the relevant data point is not plotted in the graph. A positive correlation was also found between sway area with EC and Sol AR (y = 0.01x + 1.38, R2 = 0.28, p < 0.05) (not shown).
Relationship between response latency and clinical indexes of motricity and sensation
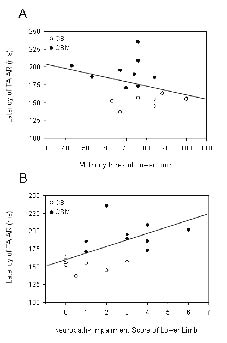
In Fig. 4A and B, the latency of the TA AR is plotted against the clinical scores of motricity and sensation assessed for the lower limbs. While there was no correlation between TA response latency and the motricity index (Fig. 4A) (y = –0.6 x + 219.3, R2 = 0.11, p = n.s.), a correlation was found between TA response latency and the sensory score (Fig. 4B) in spite of the rather large scatter of the data points (y = 8.1x + 158.0, R2 = 0.32, p < 0.0005).
Fig. 4. The latency of the tibialis anterior (TA) antagonist reaction (AR) is plotted against the clinical scores of motricity (A) and sensation (B) assessed for the lower limbs. While the correlation between the latency and the motricity index was not significant, a significant correlation (p < 0.0005) was found instead with the sensory score.
Discussion
As a whole, patients recruited in this study were more unstable than normal subjects, as shown by the larger than normal body sway during quiet stance. In addition to increased sway, these patients were also slightly more forwards inclined than normal subjects, a posture probably connected with the search for a more secure position, common to other disorders such as polyneuropathy (15–17).
Stance ataxia is limited to patients with myelopathy
We have indeed chosen to separate the patients with respect to MRI findings, in the belief that this criterion would be free from possible errors connected with the clinical examination. Furthermore, MRI has become the imaging study of choice as the initial screening process for patients in whom cord CSM is suspected. While MRI may occasionally detect pathology in asymptomatic patients, overall the advantages of MRI outweigh its problems (18). When the 2 groups of patients were considered, we found that only those showing hyperintensity of T2-weighted images at cervical cord level (CSM) had grossly abnormal stabilometric data and latencies of late responses to postural perturbation. These figures were different from those found in cervical spondylosis and canal narrowing but without myelopathy (CS). The patients with CS showed, in fact, mild unsteadiness during quiet stance with respect to normal subjects, and normal latencies for all postural responses. The body sway values in the CS group were indeed larger than in the control group, but remained below the upper limit of laboratory for normality. However, the distribution of the individual data points of patients with CS was distinct from the CSM group. Therefore, major stance ataxia is not necessarily a correlate of severe spondylosis per se, in spite of the latter producing neck symptoms of various origins, but shows up only when MRI signs of cervical cord lesion are obvious.
The sensory score of the lower limb was consistent with the MRI-based patient subdivision, since the median value of the sensory score (NIS, see Table I) was just 0.3 in the patients with CS and 3.0 in the patients with CSM. Furthermore, when the latencies of the long-loop responses were related to the sensory score, a correlation was found: the more affected the sensation, the longer the response latency. However, while the MRI criterion completely segregated the body sway values of the 2 group of patients (the smallest sway of the CSM was larger than the largest sway of the CS group), the NIS was less critical to sway. When the entire CS population was divided in 2 groups (smaller and larger than the median NIS value) there was a major overlap of sway values data between the 2 groups. Therefore, it seems that the MRI criterion is not inferior to a clinical criterion for setting a watershed between patients with CS and CSM, at least as far as postural instability and latency of long-loop responses are concerned.
Is unsteadiness explained by neck disorders or by cervical cord myelopathy?
Disturbance of the neck musculature can provoke dizziness or unsteadiness, the so-called cervical vertigo or cervicogenic dizziness. Cervical mechanoreceptor dysfunction has been suggested as a cause of dizziness in whiplash-associated disorders (19). However, it is unclear to what extent sensory disorders of the neck result in objective disturbance to body equilibrium. Previous authors have shown this to occur (4), although others have pointed out large dissimilarities in postural performance across patients (20). Difficulty in relaxing neck postural muscles or fatigue of these muscles (5, 6), which may be at the origin of abnormal fatigue-related sensory inflow to the brain, can also lead to increased body sway. The findings in patients with CS without myelopathy are in favour of the view that neck problems, particularly if accompanied by dysaesthesia and neck pain connected with compression of nerve fibres or roots at their entry in the spinal canal, can lead to quantifiable, but only minor, instability.
On the other hand, the major stance ataxia that occurs in true CSM has not been documented previously. A pathophysiological explanation for this instability is the impaired transmission in the ascending and descending cord pathways, since this condition is associated with the increase in the latency of the balance-correcting responses to postural perturbation (see below). This delay in the postural response latencies is not present in the patients with CS. It could be argued therefore that ataxia in the patients with CSM is directly based on the dysfunction of the compressed cervical cord (21).
In the case of CSM, the dysfunction of the spinal cord induces a severe instability under both EO and EC conditions, resembling that observed in sensory neurone diseases (17), where the pathology involves the dorsal root ganglion cells. Therefore, myelopathy affects body stability most when patients shift from visual to proprioceptive control of postural sway. On the other hand, the discrepancy between the EO and EC conditions speaks against weakness of the lower limb muscles as a cause of instability: if this were the major cause of the unsteadiness, sway EO should also show a major increase. This interpretation is in keeping with the finding that the clinical data did not point to major weakness in the lower limb muscles, while the sensory index was much more affected. Other reports have shown that, when sway is recorded in neuropathic patients presenting with severe weakness in the muscles around the ankle, its value can be normal and not related to weakness scores (3).
Segmental and suprasegmental pathways mediating the postural responses
Early and late responses to toe-up rotation. This perturbation stretched the Sol muscle and consistently evoked a SLR and a MLR in the same muscle and an AR in the TA. In both groups of patients, both Sol responses were not different in latency from normal subjects. This is interesting for 3 reasons. First, it confirms of the spinal origin of both responses (22): the SLR is the counterpart of the monosynaptic reflex, while the MLR is probably dependent on the group II spindle input, also acting at segmental level (13). Secondly, the data confirm that these patients had no lower limb peripheral neuropathy that could have reduced the conduction velocity of the fibres through which both responses travel. The latter condition could accompany postural ataxia, often found in peripheral neuropathies (15, 16). Thirdly, it suggests that the afferent volley following the stretch is comparable in the 3 populations, although no evidence is provided that the afferent volley is equal in the 3 subject groups.
The AR in the TA muscle was instead delayed and reduced in size. These changes occurred however only in the CSM, whereas the response latency was nearly unchanged in patients with CS. The decreased size of the response was probably connected with the increased Sol background activity in the CSM. One may note that the increase in latency might have been, if anything, underestimated, since the slightly forward-inclined attitude of these CSM patients should have produced a shortening of the latency of this response (13). Thus, the TA AR delay in CSM is consistent with a severely abnormal transmission of the proprioceptive input to the suprasegmental centres (22–24).
Early and late responses to toe-down rotation. The MLR in the TA muscle and the AR in the Sol to toe-down rotations were delayed in the CSM but not in the CS patients. The MLR of the TA muscle has been suggested to be a spinal response dependent on group II spindle afferent fibres feeding spinal reflex circuits (13). It is not immediately clear why it should not remain intact in CSM, given that the analogous MLR of the Sol muscle to toe-up rotation was unaffected in all patients (see above). We propose the following, not mutually exclusive, explanations for the increased latency and decreased size of TA MLR. The postural attitude of the patients with CSM, featuring a slightly forward body tilt, might at least partially explain the longer latency and smaller amplitude of the TA MLR, since the toe-down platform rotation stretches a shorter and slacker TA muscle in forward tilted subjects (13). Furthermore, the large background activity in the Sol in the quiet-stance period preceding the perturbation (consistent with the forward inclined posture) might have reduced the excitability of the TA motor pool by reciprocal inhibition. In addition, the delay in the TA MLR might also be a counterpart of the imbalance in the descending drive to the extensor and flexor muscles that accompanies the spastic paraparesis of the patients with CSM (2). This might produce an abnormal increase in excitability of the short-latency reflexes and a concurrent disfacilitation of the reflex pathways subserving the MLR. Finally, while the early part of the burst is certainly conveyed by the group II afferent fibres through oligosynaptic segmental circuits, the burst component appearing some 20 ms after the response onset is due to a transcortical reflex travelled by group Ia fibres (25). Therefore, the late component of the TA MLR burst can be curtailed by the injury of these pathways along their passage in the compressed cervical cord, which possibly explains the diminished size of the response.
The changes in latency of the Sol AR evoked by the toe-down platform rotation greatly resemble those observed in the TA AR in the toe-up rotation. This finding confirms the hypothesis that both responses travel through long spinal or supraspinal relays (17, 23, 24).
Unsteadiness and balance-correcting responses
The relationship between increased sway and delayed latency of both TA and Sol AR suggests that the proprioceptive information from both flexor and extensor leg muscles and the responses evoked by this input normally cooperate in the control of quiet stance. In other forms of postural unsteadiness (e.g. Friedreich’s ataxia), a specific finding was the delayed onset of this stabilizing late response (24). TA AR is also delayed in sensory neurone diseases patients (17), who experience serious stance unsteadiness. Interestingly, in the present study, the TA AR latency appears to be correlated with the increased body sway. This establishes a connection between the presumed conduction deficits along the sensory pathways (26) and the ataxia. Not unexpectedly, sway is in fact much larger in CSM than in peripheral neuropathy: in the latter patients, the central pathways are intact and the latency of TA AR shows a smaller increase merely connected to the diminished conduction velocity of the peripheral nerve fibres (15, 16).
Myelopathy can bilaterally affect both ascending and descending pathways mediating the balance-correcting responses
One may note that any long-loop reflex need not be transcortical: the segmental circuits pre-motoneuronal to the upper and lower limb motoneurones are also interconnected by long propriospinal pathways, which may also subserve the coordination of the 4 limbs during locomotion (27). The cord compression would therefore interact with either or both the ascending and descending pathways and the supraspinal centre subserving the long-loop response, thereby delaying the onset of the responses and possibly decreasing their size. In this context, it has been shown that, due to cord compression, abnormal temporal summation of multiple descending potentials following transcranial magnetic stimulation produces delays of motor neurone firing in cervical spondylosis (28).
Owing to the limited number of patients with routine SEPs examinations, no correlation was attempted between the delayed latency of the long-loop responses and the slowed conduction velocity of descending or ascending central pathways. However, we would point out that lower limb short-latency SEP responses were abnormal in 1 out of 4 patients with CS. Moreover, SEPs were altered in only 2 out of 6 patients with CSM. On reflection, these oddities are not surprising, since all patients were able to walk unassisted, in spite of the MRI-established myelopathy and major stance ataxia: only in severely affected patients have SEPs been shown to be delayed (29). This may be partly due to SEPs mainly depending on the transmission along large-diameter fibres, while Sol and TA ARs may rely on the impulses travelling along the medium-diameter fibres. The strength of the electrical stimulus at the parameters normally used (just above motor threshold) is probably insufficient to fully activate the spindle group II fibres: the mean diameter of the motor axons is slightly smaller than that of the Ia (30) but above that of the group II fibres (31). On the other hand, the SEP is almost saturated at 2.5 × (32), at which group II fibres should be recruited in a fair proportion. But the initial part of the SEP would hardly reflect the contribution of such a volley, because the waves conveyed by higher threshold, small-diameter afferent fibres (at 2 ×) are embedded in the SEP waveforms (33). Therefore, one cannot readily predict the postural unsteadiness or the delay of TA and Sol ARs from SEPs and vice versa. Unfortunately, the stretch-elicited SEPs had not been recorded in the present study (34). It is, however, unlikely that the myelopathy led to major muscle rheological modifications as occurs in long-standing hemiparesis, changes that might have produced substantial differences in the afferent volleys following stretch. In fact, most patients had only mild spasticity, and the reflex excitability was not different between CS and CSM, as tested by the tendon reflexes. In addition, in a previous investigation in different populations with severe spasticity, we did not observe changes in latency of the leg muscle responses to stretch (2).
In conclusion, cervical spondylosis does produce signs of instability during quiet stance. Unless the spinal cord is directly affected by the narrowing of the cervical canal, however, no major unsteadiness occurs. In contrast, MRI signs of myelopathy are accompanied by large increases in body sway. These data corroborate the notion that the control of upright stance is based not only on spinal proprioceptive feedback, but also on supraspinal integration leading to appropriate posture adjustments on a feed-forward basis (16).
On the clinical side, stabilometry can represent an easy and economic way of screening CSM from CS. In addition to the clinical neurological examination, stabilometric evaluation prior to physiotherapy targeting neck problems in patients without MRI might help to exclude from the therapeutic programme those with potential myelopathy, who might undergo dramatic consequences from inappropriate treatment. The finding of a large neurological sensory impairment score accompanied by abnormal body sway would be a strong indication for MRI examination. Stabilometry may also be a valuable tool after the intervention of surgical decompression of the cervical cord for quantifying the amelioration of balance and the effectiveness of treatment in the formerly ataxic patients. However, because this investigation has been performed on a small number of patients, the results should be confirmed on a larger population.
Acknowledgements
This study was supported by the “Ricerca Finalizzata 2002” grant # 174 from the Italian Ministry of Health, “FIRB 2001” grant # RBNE01FJ4J and “PRIN 2005” grant # 2005059738 from the Italian Ministry of University.
References
1. Takayama H, Muratsu H, Doita M, Harada T, Yoshiya S, Kurosaka M. Impaired joint proprioception in patients with cervical myelopathy. Spine 2005; 30: 83–86.
2. Nardone A, Galante M, Lucas B, Schieppati M. Stance control is not affected by paresis and reflex hyperexcitability. The case of spastic patients. J Neurol Neurosurg Psychiat 2001; 70: 635–643.
3. Nardone A, Tarantola J, Miscio G, Pisano F, Schenone A, Schieppati M. Loss of large-diameter spindle afferent fibres is not detrimental to the control of body sway during upright stance: evidence from neuropathy. Exp Brain Res 2000; 135: 155–162.
4. Karlberg M, Johansson R, Magnusson M, Fransson PA. Dizziness of suspected cervical origin distinguished by posturographic assessment of human postural dynamics. J Vestib Res 1996; 6: 37–47.
5. Stapley PJ, Beretta MV, Dalla Toffola E, Schieppati M. Neck muscle fatigue and postural control in patients with whiplash injury. Clin Neurophysiol 2006; 117: 610–622.
6. Schieppati M, Nardone A, Schmid M. Neck muscle fatigue affects postural control in man. Neuroscience 2003; 121: 277–285.
7. Takahashi M, Sakamoto Y, Miyawaki M, Bussaka H. Increased MR signal intensity secondary to chronic cervical cord compression. Neuroradiology 1987; 29: 550–556.
8. Tavy DL, Franssen H, Keunen RW, Wattendorff AR, Hekster RE, Van Huffelen AC. Motor and somatosensory evoked potentials in asymptomatic spondylotic cord compression. Muscle Nerve 1999; 22: 628–634.
9. Hallett M. NINDS Myotatic Reflex Scale. Neurology 1993; 43: 2723.
10. Norris FH, Calanchini PR, Fallat RJ, Panchari S, Jewett B. The administration of guanidine in amyotrophic lateral sclerosis. Neurology 1974; 24: 721–728.
11. Dyck PJ, Litchy WJ, Lehman KA, Hokanson JL, Low PA, O’Brien PC. Variables influencing neuropathic endpoints: the Rochester Diabetic Neuropathy Study of Healthy Subjects. Neurology 1995; 45: 1115–1121.
12. Nardone A, Giordano A, Corrà T, Schieppati M. Responses of leg muscles in humans displaced while standing: effects of types of perturbation and of postural set. Brain 1990; 113: 65–84.
13. Schieppati M, Nardone A, Siliotto R, Grasso M. Early and late stretch responses of human foot muscles induced by perturbation of stance. Exp Brain Res 1995; 105: 411–422.
14. Schieppati M, Nardone A. Medium latency stretch reflexes of foot and leg muscles analyzed by cooling the lower limb in standing humans. J Physiol (Lond) 1997; 503: 693–700.
15. Nardone A, Schieppati M. Group II spindle fibres and afferent control of stance. Clues from diabetic neuropathy. Clin Neurophysiol 2004; 115: 779–789.
16. Nardone A, Grasso M, Schieppati M. Balance control in peripheral neuropathy: Are patients equally unstable under static and dynamic conditions? Gait Posture 2006; 23: 364–373.
17. Nardone A, Galante M, Pareyson D, Schieppati M. Balance control in Sensory Neuron Disease. Clin Neurophysiol 2007; 118: 538–550.
18. Baron EM, Young WF. Cervical spondylotic myelopathy: a brief review of its pathophysiology, clinical course, and diagnosis. Neurosurg 2007; 60 Suppl 1: S35–S41.
19. Treleaven J, Jull G, Sterling M. Dizziness and unsteadiness following whiplash injury: characteristic features and relationship with cervical joint position error. J Rehabil Med 2003; 35: 36–43.
20. Michaelson P, Michaelson M, Jaric S, Latash ML, Sjolander P, Djupsjobacka M. Vertical posture and head stability in patients with chronic neck pain. J Rehabil Med 2003; 35: 229–235.
21. Hainline B, Tuszynski MH, Posner JB. Ataxia in epidural spinal cord compression. Neurology 1992; 42: 2193–2195.
22. Ackermann H, Diener HC, Dichgans J. Changes in sensorimotor functions after spinal lesions evaluated in terms of long-latency reflexes. J Neurol Neurosurg Psychiatry 1987; 50: 1647–1654.
23. Field-Fote EC, Dietz V. Single joint perturbation during gait: Preserved compensatory response pattern in spinal cord injured subjects. Clin Neurophysiol 2007; 118: 1607–1616.
24. Diener HC, Dichgans J, Bacher M, Guschlbauer B. Characteristic alterations of long-loop “reflexes” in patients with Friedreich’s disease and late atrophy of the cerebellar anterior lobe. J Neurol Neurosurg Psychiatry 1984; 47: 679–685.
25. Petersen N, Christensen LO, Morita H, Sinkjaer T, Nielsen J. Evidence that a transcortical pathway contributes to stretch reflexes in the tibialis anterior muscle in man. J Physiol (London) 1998; 512: 267–276.
26. Tani T, Yamamoto H, Kimura J. Cervical spondylotic myelopathy in elderly people: a high incidence of conduction block at C3–4 or C4–5. J Neurol Neurosurg Psychiatry 1999; 66: 456–464.
27. Knikou M. Neural coupling between the upper and lower limbs in humans. Neurosci Lett 2007; 416: 138–143.
28. Nakanishi K, Tanaka N, Kamei N, Hamasaki T, Nishida K, Touten Y, Ochi M. Significant correlation between corticospinal tract conduction block and prolongation of central motor conduction time in compressive cervical myelopathy. J Neurol Sci 2007; 256: 71–74.
29. Restuccia D, Di Lazzaro V, Lo Monaco M, Evoli A, Valeriani M, Tonali P. Somatosensory evoked potentials in the diagnosis of cervical spondylotic myelopathy. Electromyogr Clin Neurophysiol 1992; 32: 389–395.
30. Schalow G, Zäch GA, Warzok R. Classification of human peripheral nerve fibre groups by conduction velocity and nerve fibre diameter is preserved following spinal cord lesion. J Auton Nerv Syst 1995; 52: 125–150.
31. Simonetta-Moreau M, Marque P, Marchand-Pauvert V, Pierrot-Deseilligny E. The pattern of excitation of human lower limb motoneurones by probable group II muscle afferents. J Physiol 1999; 517: 287–300.
32. Fukuda H, Sonoo M, Ishibashi M. Muscle afferent contributions to tibial nerve somatosensory evoked potentials investigated using knee stimulations. Clin Neurophysiol 2007; 118: 2104–2111.
33. Huttunen J. Effects of stimulus intensity on frontal, central and parietal somatosensory evoked potentials after median nerve stimulation. Electromyogr Clin Neurophysiol 1995; 35: 217–223.
34. Starr A, McKeon B, Skuse N, Burke D. Cerebral potentials evoked by muscle stretch in man. Brain 1981; 104: 149–166.