OBJECTIVE: To evaluate the effectiveness of acupuncture for fibromyalgia.
METHODS: Fifty-eight women with fibromyalgia were allocated randomly to receive either acupuncture together with tricyclic antidepressants and exercise (n = 34), or tricyclic antidepressants and exercise only (n = 24). Patients rated their pain on a visual analogue scale. A blinded assessor evaluated both the mean pressure pain threshold value over all 18 fibromyalgia points and quality of life using SF-36.
RESULTS: At the end of 20 sessions, patients who received acupuncture were significantly better than the control group in all measures of pain and in 5 of the SF-36 subscales. After 6 months, the acupuncture group was significantly better than the control group in numbers of tender points, mean pressure pain threshold at the 18 tender points and 3 subscales of SF-36. After one year, the acupuncture group showed significance in one subscale of the SF-36; at 2 years there were no significant differences in any outcome measures.
CONCLUSION: Addition of acupuncture to usual treatments for fibromyalgia may be beneficial for pain and quality of life for 3 months after the end of treatment. Future research is needed to evaluate the specific effects of acupuncture for fibromyalgia.
Key words: randomized trial, acupuncture, fibromyalgia.
J Rehabil Med 2008; 40: 582–588
Correspondence address: Rosa A. Targino, Avenida Doutor Arnaldo, 455, Departamento de Patologia, São Paulo, SP, Brazil. E-mail: targino@usp.br
Submitted August 10, 2007; accepted March 5, 2008
INTRODUCTION
Fibromyalgia is a diffuse musculoskeletal pain syndrome with multiple tender points that are widely and symmetrically distributed throughout the body (1). The main symptom is widespread musculoskeletal pain, lasting longer than 3 months, which is associated with chronic fatigue, cognitive dysfunction, sleep disorder, morning stiffness, anxiety and depression. For most patients, these chronic symptoms negatively affect their quality of life and performance (2–5). The aetiology of fibromyalgia remains unknown (6–8).
In Brazil, fibromyalgia is estimated to affect 2.5% of the population (8). This prevalence is similar to that in other countries (9–11).
In the year 2000, fibromyalgia was cited as the main cause of musculoskeletal pain among patients attending the Clinics Hospital, in São Paulo, Brazil (12). Despite increasing interest in and understanding of this complex syndrome, effective and specific treatment is still not available, and there are no US Food and Drug Administration-approved treatments (13, 14). Standard treatment typically involves the chronic use of medication for pain control. The aim of this study was to assess the efficacy of an alternative therapeutic approach.
Evidence from randomized trials shows that partial and short-term improvements in fibromyalgia symptoms can be achieved with low doses of antidepressants (15); physical activity such as aerobic exercise (16); relaxation techniques (17–18); and behavioural therapies (19–20).
Acupuncture is one of the oldest forms of therapy and is widely practised in the USA. Each year about 1 million Americans undergo acupuncture treatments, mainly to relieve pain caused by a variety of ailments (21). A consensus statement from the US National Institutes of Health (NIH) concluded that acupuncture may be useful as an adjunct treatment or may be an acceptable alternative treatment in a comprehensive management programme for fibromyalgia patients (22). In Brazil, there is increased interest in acupuncture; in 1995, a federal law established that the procedure can be performed only by physicians.
Systematic reviews looking at the effectiveness of acupuncture for fibromyalgia have found a limited number of high-quality scientific studies. There is moderate evidence that acupuncture is more effective than sham acupuncture in improving symptoms of fibromyalgia (23–25). The quality of the randomized trials in this area has been criticized because of small study populations and short duration of follow-up intervals (23–26). However, a recently published randomized trial demonstrated that acupuncture was no better than 3 different forms of sham acupuncture in relieving subjective pain among patients with fibromyalgia (27).
There is a need for acupuncture trials that include a large sample size of patients with similar and well-defined pain conditions. Such trials should utilize standardized and well-described acupuncture stimuli. These should be placed effectively in accordance with classical Chinese experience and utilize unequivocal primary outcome measures for the effect (28).
The objective of this study was to evaluate the benefit of adding acupuncture to the standard course of tricyclic antidepressants and exercise in patients with fibromyalgia. The 2 outcomes of interest were pain and quality of life, which were measured in a randomized trial with a 2-year follow-up period.
METHODS
Patients
We included female patients aged 20–70 years diagnosed with fibromyalgia according to the 1990 American College of Rheumatology (ACR) classification criteria (29). To be included, patients had to report moderate to severe pain intensity (visual analogue scale (VAS) > 4), and they had to be using antidepressant medication in an analgesic dose (between 12.5 and 75 mg/day).
Patients were recruited by physicians from the Clinics Hospital in São Paulo. They included doctors practising in the Pain Clinic of the Department of Neurology, those in the Rheumatology Clinic and those in the Division of Physical Medicine of the Institute of Orthopedics and Traumatology. ACR criteria were applied by one of the physicians (HHSK) to confirm the diagnosis prior to the enrolment to the study. Patients were not included in the case of severe psychiatric disease, the presence of neurological deficits, cardiac disease or glaucoma, and treatment with acupuncture within one year prior to the start of the study.
Between 2 April 2000 and 10 October 2001, 60 patients with the diagnosis of fibromyalgia were recruited to participate in the clinical trial. Two patients were not included: one did not agree to participate in the study; another had undergone acupuncture treatment in the previous 12 months. The remaining 58 patients fulfilled all inclusion criteria and agreed to participate in the trial. Table I summarizes the patients’ baseline characteristics.
| Table I. Baseline clinical and demographic characteristics of patients with fibromyalgia by treatment group |
| Characteristics | Acupuncture group n = 34 | Control group n = 24 |
| Gender (female), n (%) | 34 (100) | 24 (100) |
| Mean age, years, mean (SD) | 52.09 (10.97) | 51.17 (11.20) |
| Marital status, n (%) | | |
| Married or common-law | 18 (52.95) | 14 (58.33) |
| Single, divorced, widowed | 16 (47.05) | 10 (41.67) |
| Education, n (%) | | |
| Elementary incomplete | 7 (20.59) | 7 (29.17) |
| Elementary complete | 13 (38.24) | 10 (41.67) |
| High school | 10 (29.41) | 5 (20.84) |
| College | 3 (8.82) | 1 (4.16) |
| University | 1 (2.94) | 1 (4.16) |
| Race, n (%) | | |
| White | 23 (67.65) | 18 (75.01) |
| Black | 10 (29.41) | 6 (24.99) |
| Asian | 1 (2.94) | 0 (0) |
| Occupation, n (%) | | |
| Housewife | 20 (58.83) | 10 (41.66) |
| Working | 7 (20.58) | 9 (37.51) |
| Retired | 5 (14.71) | 4 (16.67) |
| On sick leave | 1 (2.94) | 1 (4.16) |
| Unemployed | 1 (2.94) | 0 (0) |
| Pain duration, months, mean (SD) | 118.8 (117.3) | 93.0 (75.25) |
| OUTCOME MEASURES: visual analogue scale; number of tender points (TePsN); pressure pain threshold (PPT18) (kgf/cm2). SD: standard deviation. |
Patients were informed about the treatment protocol and admitted to the study only after giving their written, informed consent. The study protocol was approved by the ethics review committee of the Clinics Hospital.
Interventions
Patients were randomly allocated to 1 of 2 treatment groups: acupuncture added to the standard care, or standard care alone. Randomization was performed using a computer-generated random sequence of numbers provided by the Hospital’s Informatics Departments. The randomization was conducted by one physician who was not involved with the inclusion or exclusion process.
Patients in the acupuncture group received 20 sessions, always performed by the same physician (RAT) who had 5 years of clinical acupuncture experience. The sessions occurred twice weekly and lasted 20 min each. The acupuncturist used disposable, sterilized, flexible stainless steel 0.25 × 40 mm needles. The classical acupuncture points employed were: Ex-HN-3 and bilateral LR3, LI4, PC6, GB34 and SP6 points (30). Needle penetration was 10–30 mm without extra rotational or manual stimulation after needle insertion. Depth of needle penetration was determined by the patient’s sensitivity until “chi” sensation was obtained. The inclination of the needle was 90º in all points except for Ex-HN-3 where it was 45º. Patients also received standard care which included 12.5–75 mg of tricyclic antidepressants per day, oral instruction to walk for 30 min twice a week at their own pace, to breathe deeply and to perform mental relaxation exercises for another 30 min. They were also told to perform twice-weekly stretching exercises involving the paraspinalis muscles, glutei, hamstrings, ankle plantar flexors and hip flexors. The dosage of the tricyclic antidepressant was individualized according to the routine medical treatment of our pain clinic.
Patients randomized to the control group received the same standard care; however they did not receive any acupuncture treatment. They were seen by a physician at the beginning of the study and during the follow-up visits. No additional visits were scheduled for the controls to compensate for the extra attention being received by patients in the acupuncture treatment group. Compliance with the use of either exercise or antidepressant drugs was based on patients’ reports during the outcome evaluation interviews.
Outcome assessment
The primary outcome measure was pain intensity at the first follow-up visit after the end of the 20 acupuncture sessions. This visit occurred 3 months after randomization (T1). Pain intensity was evaluated using a VAS (10 cm), where “zero” corresponds to no pain and “10” corresponds to the worst pain experienced by the patient.
Other pain-related outcomes were the number of tender points below 4 kg/cm2 (TePsN) and the mean pressure pain threshold (PPT) value over the 18 fibromyalgia points (PPT18), as quantified by a pressure algometry (Pain Diagnostics, Great Neck). Standard values, validity and reproducibility of PPT measured by pressure algometry have been demonstrated over normal muscles (31). The number of tender points is a criterion for the diagnosis of fibromyalgia. According to the ACR, there should be at least 11 of 18 tender point sites that are painful with digital palpation pressure of 4 kg. PPT18 was obtained by determining the sum of the PPT value of the 18 tender points divided by 18 and expressed in kgf/cm2. Higher PPT18 values indicate less severe symptoms.
In addition to these pain-related outcomes, patients’ quality of life was assessed by the validated Portuguese version of the MOS 36-item short form health survey (SF-36) scale (32). The scale quantifies patients’ quality of life in 8 multi-item scales measuring physical functioning, role limitations owing to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations owing to emotional problems and mental health (33). Higher values indicate better quality of life.
All outcome assessments were conducted at baseline, and again 3, 6, 12 and 24 months after the first evaluation. Patients rated their pain intensity using a VAS. Blinded evaluation of PPT18 and TePsN was carried out by a single physician (HHSK), while blind evaluation of quality of life was conducted by one psychologist (LPMS). Even though the patients knew which group they were in (either the acupuncture treatment group or the standard care group), they were instructed not to communicate this information to the outcome assessors.
Statistical analysis
This study was designed to have 80% power to detect a 1.2-point difference on the VAS before and after treatment, with a 0.05 probability of type I error. To determine the sample size, we used the results of a previous pilot study (34). In this study, a mean reduction of 2.07 in the acupuncture group and 0.9 in the control group was reported. The required sample size was 25 patients in each group (treatment and controls).
The analysis, which continued up to 12 months after randomization, was based on an intention-to-treat principle; this means that all randomized patients were included in the analysis, and they were analysed according to the randomized treatments. At the 24-month follow-up, 3 randomized patients were lost, and no attempt was made to input any value for their outcomes.
For the PPT18 variable, we used paired t-tests for within-group comparisons and Student’s t-tests for between-group comparisons. We used Wilcoxon rank-sum tests for within-group comparisons and Mann-Whitney U tests for between-group analysis of VAS, TePsN and SF-36. PPT18 was analysed using means and standard deviation (SD). VAS, TePsN and SF-36 values were analysed using median and range (35).
For categorical variables, we used either a χ2 test or Fisher’s exact test. Standard statistical software package SPSS 13.0 for Windows was used for the analyses. All reported p-values are 2-tailed and were considered significant at the 0.05 level.
RESULTS
Primary outcome measure
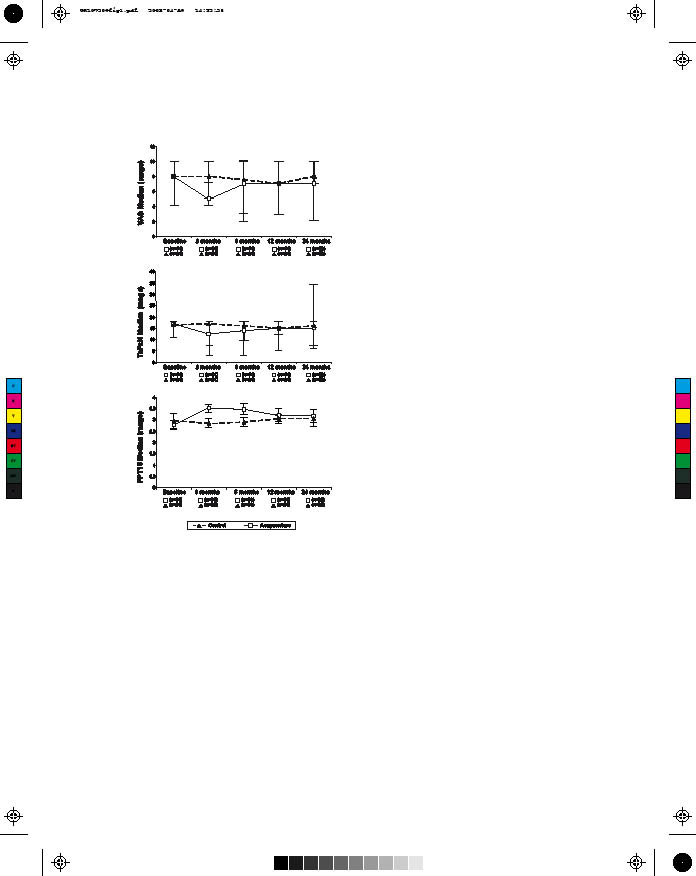
According to our primary outcome measure (pain using VAS), acupuncture added to usual care was more effective than standard care alone. At 3 months, the median VAS score in the group that received acupuncture was 5.0 (range 0–10) compared with 8.0 (range 4–7) in the group that received usual care only. This difference was statistically significant (p < 0.001) (see Table II and Fig. 1). VAS evaluations at 6, 12 and 24 months’ follow-up were not statistically different between the 2 groups (p > 0.05) (see Table II and Fig. 1).
| Table II. Results of VAS and TePsN PPT18. Values are reported as median (range) for VAS and TePsN and as mean (SD) for PPT18 |
| Variable | Acupuncture Median (range) or Mean (SD) | Control Median (range) or Mean (SD) | p-value |
| Baseline (T0) | n = 34 | n = 24 | |
| VAS | 8.0 (4.0–10.0) | 8.0 (4–10) | |
| TePsN | 17.0 (11–18) | 16.5 (11–18) | |
| PPT18 | 2.78 (0.53) | 2.96 (0.81) | |
| 3 months (T1) | n = 34 | n = 24 | |
| VAS | 5.0 (0.0–10.0) | 8.0 (4.0–7.0) | < 0.001‡** |
| TePsN | 12.5 (3–18) | 17.0 (7–18) | < 0.001‡** |
| PPT18 | 3.53 (0.69) | 2.84 (0.53) | < 0.001†** |
| 6 months (T2) | n = 34 | n = 24 | |
| VAS | 7.0 (2.0–10.0) | 7.5 (3.0–10.0) | 0.18‡ |
| TePsN | 14.0 (3–18) | 16.0 (10–18) | 0.016‡* |
| PPT18 | 3.47 (0.70) | 2.90 (0.55) | 0.002†** |
| 12 months (T3) | n = 34 | n = 24 | |
| VAS | 7.0 (0.0–10.0) | 7.0 (3.0–10.0) | 0.65‡ |
| TePsN | 15.0 (5–18) | 15.0 (12–18) | 0.47‡ |
| PPT18 | 3.19 (0.86) | 3.05 (0.47) | 0.46† |
| 24 months (T4) | n = 32 | n = 23 | |
| VAS | 7.0 (0.0–10.0) | 8.0 (2.0–10.0) | 0.58‡ |
| TePsN | 15.0 (6–18) | 16.0 (7–18) | 0.16‡ |
| PPT18 | 3.18 (0.80) | 3.05 (0.88) | 0.60† |
| †Unpaired t-test; ‡Mann Whitney U test; *statistically significant (p< 0.05); **statistically significant (p< 0.005). SD: standard deviation; VAS: visual analogue scale; TePsN: number of tender points; PPT18: mean pressure pain threshold value over the 18 fibromyalgia tender points (kgf/cm2). |
Secondary outcome measures
The addition of acupuncture also improved other outcome measures (TePsN, PPT18 values, and 5 subscales of the SF-36) at the 3-month follow-up (T1) (see Tables II, III and Fig. 1).
However, at the 6-month follow-up (T2), the benefits of acupuncture vs standard care were maintained only for TePsN, PPT18 (Table II; Fig. 1) and for one subscale (general health) of the SF-36 (Table III).
At the 12-month follow-up (T3), only one subscale (role physical) of the SF-36 showed a statistically significant difference in favour of the acupuncture group (see Tables II, III and Fig. 1). At the 24-month follow-up (T4), there were no statistically significant differences between patients in the acupuncture and the control group in any measure of pain or quality of life (see Tables II, III and Fig. 1).
| Table III. Results for SF-36 subscales |
| Variable | Acupuncture Median (range) | Control Median (range) | p-value |
| Baseline (T0) | n = 34 | n = 24 | |
| PF | 37.5 (10.0–70.0) | 30.0 (5.0–70.0) | |
| RP | 0.0 (0.0–100.0) | 0.0 (0.0–75.0) | |
| BP | 27.0 (0.0–82.0) | 31.0 (10.0–590.0) | |
| GH | 38.5 (5.0–85.0) | 45.0 (15.0–87.0) | |
| VT | 32.5 (0.0–80.0) | 40.0 (5.0–75.0) | |
| SF | 50.0 (0.0–87.5) | 50.0 (0.0–100.0) | |
| RE | 16.0 (0.0–100.0) | 0.0 (0.0–100.0) | |
| MH | 46.0 (0.0–76.0) | 46.0 (0.0–88.0) | |
| 3 months (T1) | n = 34 | n = 24 | |
| PF | 50.0 (20.0–90.0) | 42.5 (0.0–90.0) | 0.021* |
| RP | 25.0 (0.0–100.0) | 0.0 (0.0–75.0) | |
| BP | 41.5 (12.0–74.0) | 31.5 (10.0–51.0) | 0.002** |
| GH | 55.0 (15.0–92.0) | 48.5 (10.0–97.0) | |
| VT | 55.0 (20.0–90.0) | 37.5 (0.0–70.0) | 0.022* |
| SF | 62.5 (25.0–100.0) | 50.0 (12.5–100.0) | |
| RE | 100.0 (0.0–100.0) | 0.0 (0.0–100.0) | 0.004** |
| MH | 62.0 (4.0–92.0) | 46.0 (0.0–84.0) | 0.008* |
| 6 months (T2) | n = 34 | n = 24 | |
| PF | 50.0 (10.0–85.0) | 45.0 (5.0–80.0) | |
| RP | 0.0 (0.0–100.0) | 0.0 (0.0–7.5) | |
| BP | 31.0 (10.0–74.0) | 31.0 (10.0–61.0) | |
| GH | 58.5 (25.0–92.0) | 43.5 (2.0–87.0) | 0.027* |
| VT | 47.5 (0.0–75.0) | 45.0 (0.0–75.0) | |
| SF | 50.0 (12.5–100.0) | 62.0 (12.5–100.0) | |
| RE | 50.0 (0.0–100.0) | 0.0 (0.0–100.0) | |
| MH | 56.0 (20.0–92.0) | 56.0 (0.0–80.0) | |
| 12 months (T3) | n = 34 | n = 24 | |
| PF | 50.0 (25.0–95.0) | 50.0 (0.0–90.0) | |
| RP | 0.0 (0.0–100.0) | 0.0 (0.0–50.0) | 0.038* |
| BP | 32.5 (0.0–74.0) | 36.0 (0.0–62.0) | |
| GH | 52.0 (12.0–97.0) | 52.0 (10.0–92.0) | |
| VT | 52.5 (0.0–100.0) | 37.5 (5.0–9.5) | |
| SF | 62.5 (12.5–112.5) | 75.0 (0.0–212.5) | |
| RE | 33.3 (0.0–100.0) | 50.0 (0.0–100.0) | |
| MH | 56.0 (8.0–100.0) | 58.0 (8.0–88.0) | |
| 24 months (T4) | n = 32 | n = 23 | |
| PF | 57.5 (10.0–95.0) | 55.0 (5.0–85.0) | 0.234 |
| RP | 25.0 (0.0–100.0) | 0.0 (0.0–100.0) | 0.290 |
| BP | 41.0 (0.0–100.0) | 41.0 (–20.0–84.0) | 0.993 |
| GH | 57.0 (20.0–87.0) | 55.0 (20.0–87.0) | 0.898 |
| VT | 50.0 (10.0–95.0) | 50.0 (15.0–90.0) | 0.864 |
| SF | 62.5 (0.0–112.5) | 50.0 (25.0–100.0) | 0.079 |
| RE | 66.67 (0.0–100.0) | 33.3 (0.0–100.0) | 0.936 |
| MH | 60.0 (4.0–100.0) | 52.0 (20.0–92.0) | 0.274 |
| Mann-Whitney U test: *statistically significant (p < 0.05); **statistically significant (p < 0.005). PF: Physical Functioning, RP: Role Physical, BP: Bodily Pain, GH: General Health, VT: Vitality, SF: Social Functioning, RE: Role Emotional, MH: Mental Health. |
Patients’ VAS, TePsN and PPT18 scores in the acupuncture group also showed improvement compared with their pre-treatment values and all follow-up evaluations including at 24 months’ follow-up (p < 0.005). No significant differences (p > 0.05) were noted in patients in the standard care group at any time (Fig. 1).
Patient compliance with the acupuncture treatment was 97.1% (i.e. 33 patients came to all 20 acupuncture sessions). Only one patient did not complete the full course, abandoning the acupuncture treatment after receiving 17 sessions because of complete relief of pain. All data from the randomized patients were analysed in all evaluations, except for the 24-month follow-up, where the follow-up rate was 94.1% in the acupuncture group and 95.8% in the control group.
Fig. 1. Comparisons between acupuncture and control group’s scores for visual analogue scale (VAS), number of tender points (TePsN) and pressure pain threshold (PPT8). Values expressed as median (range) for VAS and TePsN and as means (standard deviation) for the PPT18.
DISCUSSION
This study showed that the addition of acupuncture to the usual treatment for fibromyalgia, compared with the control group, improved all pain outcome measures (VAS, TePsN and PPT18) in short-term follow-up; for intermediate-term follow-up after acupuncture treatment, pain measured by TePsN and PPT18 was also reduced. At both follow-up intervals, there was improvement noted in the TePsN and in the mean pain pressure threshold values over all PPT18. Our results, however, did not demonstrate benefits at the longer term follow-up in any of the pain outcome measures.
We found that quality of life improved more among patients in the acupuncture treatment group compared with those in the standard care group. However, these benefits were more pronounced at the short-term follow-up and in specific subscale measurements of the SF-36, namely physical functioning, bodily pain, vitality, and emotional and mental health. We only detected a significantly better score for the role physical subscale of the SF-36 at 12 months’ follow-up.
Patients’ VAS, TePsN and PPT18 scores in the acupuncture group also showed improvement compared with their pre-treatment values and all follow-up evaluations. It was interesting to find that patients with such a severe disease improved if they received acupuncture added to the standard care.
Our study also demonstrated that, at short-term follow-up, 88% of patients in the acupuncture group experienced a relevant improvement in pain intensity after 20 sessions of acupuncture, 79% of patients showed improvement in their TePsN score, and 88% of patients showed improvement in their PPT18 score. After 2 years, this improvement drops to 62, 64, and 61%, respectively.
Several previous randomized (27, 36–42) and non-randomized (43, 44) trials have demonstrated a beneficial effect from acupuncture in fibromyalgia patients. The only contradictory results were found by Assefi et al. (27), who could not demonstrate any benefit of acupuncture in relieving pain compared with 3 different types of sham treatment (27). One explanation may be that Assefi et al. (27) did not use any adjunctive therapies with acupuncture to treat the patients.
It is possible that the treatment benefit observed in our trial was due to a synergistic effect of combining acupuncture with antidepressants (23, 45). In comparison with antidepressant drugs alone, Cassisi et al. (45) also demonstrated benefits when acupuncture was combined with antidepressants. Dosage of the tricyclic antidepressant used by our patients was prescribed according to the routine medical treatment of our pain clinic and was kept the same throughout the entire study period. We agree with Millea & Holloway (16), that the dosage of tricyclic antidepressant must be individualized, given variable absorption, metabolism and excretion (16). Dosage varied from 12.5 to 75 mg/day and most of our patients (84.5%) received 50 mg/day. There was no significant difference between the dosages used in both groups (p = 0.329, χ2 test). Therefore, different medication dosages among patients did not confound our results.
Similar to Martin et al., (41), our patients were homogenous in diagnosis, characteristics and severity of symptoms. We also evaluated a female and predominantly white population, though from a developing country. We agree with Martin et al. (41), that future research should extend these observations to men and other ethnic and racial groups.
Most studies (27, 39–42) have evaluated the effect of acupuncture compared with sham treatment. We agree again with Martin et al. (41), that placement of the acupuncture needles at incorrect or sham points may provide neuromodulatory inputs to the sensory nervous system producing physiological changes that are indistinguishable from changes due to stimulation of “true” acupuncture points. We also believe that the placebo-simulated configuration described by Martin et al. (41), is a better, more realistic placebo acupuncture treatment that should be employed in future studies. They demonstrated that acupuncture was significantly better than placebo stimulation only one month after the end of a set of acupuncture treatments at standardized fixed points (41). Similar to our results, they did not find significantly different results in long term follow-up of 7 months (41).
A usual-care comparison group, like the one used in our pain clinic, has not been described in the literature until now. We decided to evaluate the effect of acupuncture on pain and quality of life compared with a usual care group. In our study, therefore, acupuncture was evaluated as a complementary part of the medical treatment of fibromyalgia and not as an isolated approach. We understand that, due to the complexity of fibromyalgia syndrome, associated with the severity of symptoms, monotherapy modalities are not indicated.
Similar to other randomized controlled trials that evaluated the effect of acupuncture in fibromyalgia patients (27, 41), we made a potentially controversial decision to standardize the acupuncture points in order to allow reproducibility of the technique and to help us to assess the efficacy of a specific acupuncture procedure. We realize that the use of acupuncture at fixed points may differ from acupuncture that is practised in clinical settings where therapy is usually individualized (27, 36). We agree with Assefi et al. (27), that there is no consistent data suggesting that individualized acupuncture is superior to fixed-point prescriptions. Also, no gold standard exists for the selection of acupuncture points for treatment of fibromyalgia. In the absence of data, similarly to Assefi et al. (27), we designed a protocol based on our clinical experience. We selected acupuncture points that could provide symptomatic relief in our patients, since the pathogenesis and aetiology of fibromyalgia remains unknown. Interestingly, Martin et al. (41) selected similar acupuncture points to those used in our study (LI4, SP6 and PC6). We did not use ST36, H7 and LR2. We selected GB34, LR3 and Ex-HN-3 instead. Our study reported similar results to those by Martin et al. (41), who found that acupuncture was effective to provide significant symptomatic relief in patients with fibromyalgia in the short-term but not the long-term.
There are a number of limitations to this study. The allocation of randomization was not concealed. Information on compliance regarding the use of exercise, deep breathing, walking, mental relaxation and antidepressant drugs was based only on patients’ reports during the outcome evaluation periods. Patients’ expectations about acupuncture were not assessed, and we cannot rule out the possibility that improved outcomes in the acupuncture group might have been due to the fact that these patients had more visits to healthcare providers, received more attention and social contact, and were more exposed to the therapist-patient relationship. Similarly to other authors (27, 42), we used a non-disease-specific scale to evaluate the quality of life of our patients, which is not specifically designed for fibromyalgia patients. However, the Fibromyalgia Impact Questionnaire (FIQ) had not been validated into Portuguese at the time of our study.
All randomized controlled trials published in the literature that have studied the effect of acupuncture in fibromyalgia patients have been performed in developed countries (27, 36–43, 45). Our study is the first randomized controlled trial, to our knowledge, to have evaluated the effect of acupuncture for the treatment of fibromyalgia in a developing country and with a long-term follow-up of 24 months.
There is evidence that the effects of acupuncture may last for years after a course of treatment (44). Waylonis (44) also found that the benefit lasted from one month to one year after treatment. Others, such as Deluze et al. (40), did not present any long-term results. In fact, their patients were only evaluated before the first acupuncture session and after that treatment. The other 2 high-quality randomized controlled trials only followed patients up to 6 months (27) and 7 months (41) after completion of their treatment. In our study, we followed patients up to 24 months. Our results, however did not demonstrate any longer term benefit of acupuncture in the pain outcome measures. We could only detect a significantly better score for the role physical subscale of the SF-36 at the 12-month follow-up.
One advantage of acupuncture treatment is that it produces fewer adverse side-effects compared with many drugs used to treat fibromyalgia symptoms (22). Two patients in the acupuncture group (5.8%) developed temporary oedema of the left hand at the LI4 needle insertion site. McCartney et al. (46) (2000) similarly reported a case of bilateral hand oedema after use of bilateral LI4 acupuncture points to treat chronic low-back pain and sciatica. Similar to Assefi et al. (27), Martin et al. (41) and Costa (42), acupuncture treatments were also very well tolerated by our patients. Our patients did not report discomfort, soreness, vasovagal symptoms, bruising or haematomas during the treatment period, and did not report other complaints during the follow-up evaluations.
Only 3 patients (5.2%) were lost to follow-up during our trial. This loss rate is much lower than rates reported by Deluze et al. (40) and by Cassissi et al. (45). In our trial, losses occurred only at the 24-month follow-up.
We did not measure any specific effects of acupuncture alone on pain or on quality of life. Further research will be needed to evaluate the specific individual effects of acupuncture. We feel that adding acupuncture to standard care is justified, especially when the cost of this treatment is weighed against the costs of this painful chronic condition, all of which must be borne by patients, their families and by society in general.
In conclusion, the addition of acupuncture to usual treatment for fibromyalgia may be beneficial for pain reduction and quality of life, but only in the first 3 months after the end of the treatment. Future research will be needed to evaluate the specific effects of acupuncture for fibromyalgia.
Funding
No external funding was received for this study.
REFERENCES
1. Merskey H, Bogduk N, editors. Classification of chronic pain. Description of chronic pain syndromes and definitions of terms. Seattle: IASP Press; 1994, p. 45.
2. Hawley DJ, Wolfe F. Pain, disability, and pain/disability relationships in seven rheumatic disorders: a study of 1,522 patients. J Rheumatol 1991; 18: 552–1557.
3. Henriksson C, Gundmark I, Bengtsson A, Ek AC. Living with fibromyalgia. Consequences for everyday life. Clin J Pain 1992; 8: 138–144.
4. Henriksson CM. Living with continuous muscular pain – patient perspectives. Part I: encounters and consequences. Scand J Caring Sci 1995; 9: 67–76.
5. White KP, Speechley M, Harth M, Ostbye T. Comparing self-reported function and work disability in 100 community cases of fibromyalgia syndrome versus controls in London, Ontario: the London Fibromyalgia Epidemiology Study. Arthritis Rheum 1999; 42: 76–83.
6. Alarcon GS, Bradley LA. Advances in the treatment of fibromyalgia: current status and future directions. Am J Med Sci 1998; 315: 397–404.
7. Pongratz DE, Sievers M. Fibromyalgia-symptom or diagnosis: a definition of the position. Scand J Rheumatol Suppl 2000; 113: 3–7.
8. Senna ER, De Barros AL, Silva EO, Costa IF, Pereira LV, Ciconelli RM, et al. Prevalence of rheumatic diseases in Brazil: a study using the COPCORD approach. J Rheumatol 2004; 31: 594–597.
9. Russell IJ. Fibromyalgia syndrome. In: Loeser JD, Butler SH, Chapman CR, Turkey DC, editors. Bonica’s management of pain. 3rd edn. Philadelphia: Lippincott Williams & Wilkins; 2001, p. 543–556.
10. Lindell L, Bergman S, Petersson IF, Jacobsson LT, Herrstrom P. Prevalence of fibromyalgia and chronic widespread pain. Scand J Prim Health Care 2000; 18: 149–153.
11. White KP, Speechley M, Harth M, Ostbye T. The London Fibromyalgia Epidemiology Study: the prevalence of fibromyalgia syndrome in London, Ontario. J Rheumatol 1999; 26: 1570–1576.
12. Teixeira MJ, Teixeira WGJ, Santos FPS, Andrade DCA, Bezerra SL, Figueiro JB, et al. Clinical epidemiology of musculoskeletal pain. Rev Med (Sao Paulo) 2001; 80: 1–21.
13. Arnold LM, Keck PE, Jr, Welge JA. Antidepressant treatment of fibromyalgia. A meta-analysis and review. Psychosomatics 2000; 41: 104–113.
14. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004; 292: 2388–2395.
15. Arnold LM. Biology and therapy of fibromyalgia. New therapies in fibromyalgia. Arthritis Res Ther 2006; 8: 212.
16. Millea PJ, Holloway RL. Treating fibromyalgia. Am Fam Physician 2000; 62: 1575–1582.
17. Keel PJ, Bodoky C, Gerhard U, Muller W. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998; 14: 232–238.
18. Rucco V, Feruglio C, Genco F, Mosanghini R. Training autogeno versus tecniche analogiche Ericksoniane nella terapia della sindrome fibromialgica [Autogenic training versus Erickson’s analogical technique in treatment of fibromyalgia syndrome]. Riv Eur Sci Med Farmacol 1995; 17: 41–50 (In Italian).
19. Bradley LA, Alberts KR. Psychological and behavioral approaches to pain management for patients with rheumatic disease. Rheum Dis Clin North Am 1999; 25: 215–232, viii.
20. Buskila D. Fibromyalgia, chronic fatigue syndrome, and myofascial pain syndrome. Curr Opin Rheumatol 2000; 12: 113–123.
21. Ezzo J, Berman B, Hadhazy VA, Jadad AR, Lao L, Singh BB. Is acupuncture effective for the treatment of chronic pain? A systematic review. Pain 2000; 86: 217–225.
22. NIH Consensus Conference. Acupuncture. JAMA 1998; 280: 1518–1524.
23. Berman BM, Ezzo J, Hadhazy V, Swyers JP. Is acupuncture effective in the treatment of fibromyalgia? J Fam Pract 1999; 48: 213–218.
24. Lee TL. Acupuncture and chronic pain management. Ann Acad Med Singapore 2000; 29: 17–21.
25. Mayhew E, Ernst E. Acupuncture for fibromyalgia – a systematic review of randomized clinical trials. Rheumatology 2007; 46: 801–804.
26. Crofford LJ, Appleton BE. Complementary and alternative therapies for fibromyalgia. Curr Rheumatol Rep 2001; 3: 147–156.
27. Assefi NP, Sherman KJ, Jacobsen C, Goldberg J, Smith WR, Buchwald D. A randomized clinical trial of acupuncture compared with sham acupuncture in fibromyalgia. Ann Intern Med 2005; 143: 10–19.
28. Sjölund BH. Acupuncture or acupuncture? Pain 2005; 114: 311–312.
29. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 1990; 33: 160–172.
30. World Health Organization (WHO). A proposed standard international acupuncture nomenclature. Geneva: World Health Organization; 1991.
31. Fischer AA. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 1987; 30: 115–126.
32. Ciconelli RM, Ferraz MB, Santos W, Meinao I, Quaresma MR. Brazilian Portuguese version of the SF-36. A reliable and valid quality of life outcome measure. Rev Bras Reumatol 1999; 39: 143–150.
33. Ware JE, Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473–483.
34. Targino, RA, Imamura M, Kaziyama HHS, Souza LPM, Hsing WT, Imamura ST. Pain treatment with acupuncture for patients with fibromyalgia. Curr Pain Headache Reports 2002; 6: 379–383.
35. Lund I, Lundeberg T. Aspects of pain, its assessment and evaluation from an acupuncture perspective. Acupunct Med 2006; 24: 109–117.
36. Sprott H, Franke S, Kluge H, Hein G. Pain treatment of fibromyalgia by acupuncture (abstract). Arthritis Rheum 1996; 39: S91.
37. Sprott H, Franke S, Kluge H, Hein G. Pain treatment of fibromyalgia by acupuncture. Rheumatol Int 1998; 18: 35–36.
38. Sprott H, Jeschonneck M, Grohmann G, Hein G. Änderung der Durchblutung über den tender points bei Fibromyalgia-Patients nach einer Akupunkturtherapie (gemessen mit der Laser-Doppler-Flowmetrie). Wien Klin Wochenschr 2000; 112: 580–586 (in German).
39. Lautenschlager J, Schnorrenberger CC, Müller W. Akupunktur bei generalisierter Tendomyopathie (Fibromyalgie-Syndrom). Dtsch Zschr Akup 1989; 32: 122–128.
40. Deluze C, Bosia L, Zirbs A, Chantraine A, Vischer TL. Electroacupuncture in fibromyalgia: results of a controlled trial. BMJ 1992; 305: 1249–1252.
41. Martin DP, Sletten CD, Williams BA, Berger IH. Improvement in fibromyalgia symptoms with acupuncture: results of a randomized controlled trial. Mayo Clin Proc 2006; 81: 749–757.
42. Costa EDGM. Evaluate the efficacy of acupuncture as a treatment for fibromyalgia: prospective study, randomized and controlled [PhD thesis].deral University of São Paulo UNIFESP; 2001.
43. Pasotti D, Montanari E, Capobianchi B. L` agopuntura nella Syndrome Fibromyalgica Primaria (S.F.P.): primi risultati di una ricerca [The acupuncture in Primary Fibromyalgia Syndrome (P.F.S.): first result of the research]. G Ital Rifflessot Agopunt 1990; 2: 23–31 (In Italian).
44. Waylonis GW. Long-term follow-up on patients with fibrositis treated with acupuncture. Ohio State Med J 1977; 73: 299–302.
45. Cassisi G, Roncaglione A, Cecherelli F, Donolato C, Gagliardi G, Todesco S. Trattamento agopunturale della fibrylagia primaria. Confronto con mianserina [Acupuncture treatment of primary fibromyalgia in comparison with mianserine]. G Ital Riflessot Agopunt 1995; 7: 33–36 (In Italian).
46. McCartney CJ, Herriot R, Chambers WA. Bilateral hand oedema related to acupuncture. Pain 2000; 84: 429–430.