The first step in the assessment of patients with gait abnormalities in physical and rehabilitation medicine settings is a clinical examination based on the International Classification of Functioning, Disabilities and Health. Body structure, activities and participation, and environmental factors (physical and human factors) must all be assessed. Qualitative and quantified assessments of gait are part of the activity and participation evaluation. Scales are also used to assess gait activities. Gait assessment tools can be used in laboratory environments for kinematic, kinetic, electromyographic and energy consumption analysis and other tools, such as videotape and walkways, can be used in clinical practice, while ambulatory assessment tools can be used to analyse patients’ usual everyday activities. The aims of instrumental gait assessment are: to understand the underlying mechanisms and the aetiology of the disorders, to obtain quantified gait parameters, to define suitable therapeutic methods, and to follow the course of the disease.
Key words: gait, assessment, kinematic, kinetic, electromyography, walkway, video, ICF.
J Rehabil Med 2008; 40: 497–507
Correspondence address: Laurent Bensoussan, Pôle de Médecine Physique et de Réadaptation, CHU Timone, 264, rue Saint Pierre, FR-13385 Marseille cedex 05, France. E-mail: laurent.bensoussan@ap-hm.fr
Submitted January 17, 2008; accepted May 13, 2008
*This is an educational review which is produced in collaboration with UEMS European Bord of Physical and Rehabilitation Medicine.
INTRODUCTION
The ability to walk can be impaired by the presence of lesions at various levels, such as in the nervous system, the musculoskeletal system, the cardiovascular system, and the respiratory and visual systems. Environmental conditions can also affect patients’ locomotor abilities. Physicians in physical and rehabilitation medicine (PRM) need to perform a complete assessment on their patients in order to analyse all the factors liable to interfere with their ability to walk and, where possible, to propose the best solutions for maintaining or improving their walking performance.
The first step in this examination is to diagnose all the lesions affecting any of the systems involved in walking. Only physicians are properly trained to carry out these procedures, which may lead to the application of specific treatments.
Poliomyelitis, for instance, can involve radiculopathy resulting from a conflict at the spinal level. After a computerized tomography scan, infiltration or surgery may be recommended to improve the walking and standing abilities of patients with this disorder.
Patients must be examined thoroughly in order to assess their walking abnormalities, based on the International Classification of Functioning, Disability and Health (ICF) (1, 2). All of the items in this system of classification must be analysed: impairments (body functions and body structures), activities and participation, and environmental factors. In this examination, other aspects must also be addressed, such as the existence of other complaints, the patients’ personal details, their medical history, and their quality of life. It is impossible to understand walking abnormalities without analysing all these aspects. We cannot understand gait abnormalities, such as a drop foot, if we have not studied the patient’s medical history and diagnosis (nervous and musculoskeletal disorders), the exact impairments involved (range of ankle motion, ankle flexor muscle strength, etc.), as well as establishing which activities are restricted or limited (walking on uneven ground, walking in a forest, walking on the beach), and the patient’s overall quality of life. The various parameters assessed (impairments, activities) have to be approached both qualitatively (by clinical examination) and quantitatively (by gait analysis). The clinical examination serves as the basis of this assessment and should be completed with a gait analysis.
This paper describes in detail the various aspects of this overall assessment. The 3 main questions to be addressed are as follows:
• Who are the patients? Assessing their lesions and impairments.
• How do they walk? Assessing their standing and walking performances.
• What are their lives like? Assessing their activities and participation, the environmental factors involved and their quality of life.
The first and second parts of the assessment can be performed at the PRM physician's office and in a special room in the department; the third part involves assessing patients in their home environment.
WHO IS THE PATIENT?
Patients’ complaints and wishes
PRM physicians must pay attention to the complaints and wishes of their patients and those of their family, which may be different. The patients must be put at ease. After taking time to listen to them, the PRM physician asks questions about the main symptoms, such as pain, weakness, contractures, sensory impairments, and falls. The physician must ask about the patients’ wishes: they would like to be able to walk outside unassisted, for instance, or to walk barefoot on the beach. Each symptom must be described as closely as possible in both qualitative and quantitative terms.
At the end of the full assessment procedure, PRM physicians have to respond to the complaints and wishes of patients and their families. PRM physicians must show that they have fully understood the problems encountered by patients and their families, and should explain as fully as possible what solutions can be envisaged and how they can be applied.
Patients’ personal details and medical history
Patients’ personal details prior to the onset of the medical problems can shed light on their personality. Information should be collected on the following items: the structure of the family, childhood, schooling, the highest educational level obtained, military service, social history, occupational history, leisure activities (e.g. sports, cultural, religious activities).
Medical data of interest are often obtained while collecting details about patients’ personal history, such as the anterior cruciate ligament lesion incurred by a patient while playing football when young.
Social functioning
PRM physicians should obtain details about the family (parents, spouse or partner and children), the place of residence, and the financial situation of the patients and that of their family. PRM physicians have to understand the effects of the patient’s walking abnormalities on their ability to function socially and that of their family.
Diagnosis and lesions
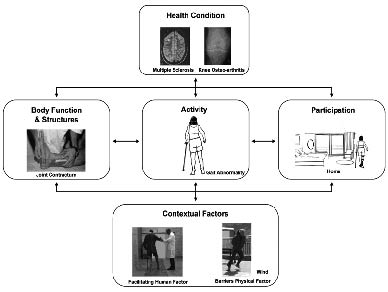
Diagnosing the patient’s pathology is the first step in the medical assessment procedure (Fig. 1). Only physicians have the ability to carry out this step. Although the diagnosis has often been established previously, in some cases it will need to be confirmed.
Fig. 1. Disability assessment according to the International Classification of Functioning, Disability and Health (ICF) model. A health disorder (multiple sclerosis) may lead to impaired body functions and structures (sensory disorders, joint contracture), limitation of activities (gait abnormalities) and participation restrictions (at home). Osteoarthritis is a potential cause of impaired body functions and structures (joint deformities, decreased range of motion) and limitation of activities, such as gait and, conversely, pathological gait, can cause or aggravate osteoarthritis. Contextual factors may act as barriers or facilitators. Strong wind makes gait more difficult, especially when gait abnormalities are present. Human help facilitates physical activities and participation of the person with impaired mobility and vice versa; the impairment of body functions (loss of skin sensation with subsequent complications, joint range of motion limitations) and activity limitations (decreased walking and transfer ability) determines the level of assistance required by care-givers. Functioning and disability are viewed as outcomes of interaction between health conditions and contextual factors. Disability involves dysfunctioning at one or more of the following levels: the level of body or body parts (impairment), the whole person (activity limitations) and the whole person in the social context (participation restrictions).
It is important to establish whether the pathology is progressive. In the case of a progressive pathology, the changes in the patient’s walking abnormalities over time must be noted.
There is often a main diagnosis and secondary diagnoses. For instance, after traumatic brain injury, the main diagnosis will focus on the various lesions present at central nervous system (CNS) level, and the secondary diagnosis will deal with lesions at all the other levels, such as the musculoskeletal system or the peripheral nervous system, resulting in weakness or sensory loss.
With complex pathologies of this kind, the diagnosis will be based on several specialists’ assessments. For instance, a neuro-radiologist will choose the best magnetic resonance imagery technique for detecting after-effects on the brain. A neuro-ophthalmologist will be the most suitable person for assessing ocular lesions as well as CNS lesions.
All the relevant data on the patient must be collected and reviewed.
Lastly, the PRM specialists will draw up a complete list of the lesions detected, with the help of other specialists.
Medical history
The PRM physician must collect the patients’ medical history. All the data must be collected step by step as precisely as possible, from the onset of the first symptoms onwards. The medical reports on all the patients’ hospitalizations, examinations and treatments have to be collected.
Details of the patients’ locomotor performances, the history of their ability to dress themselves and cope with their own personal hygiene have to be collected, along with the milestones, such as the last time they were able to walk, to go up and down stairs, the first time they started to use equipment (canes, crutches, braces, wheelchair) at home or outside the home.
The medical reports of all the physicians who were dealing with the patient’s various medical problems should be collected.
In the case of each past disease, the residuals must be assessed, as they may interfere with current medical problems. For instance, there may be a contracture at ankle level after a complex fracture.
The PRM physicians must collect the family’s medical history and note any hereditary diseases running in the family, e.g.: “my mother and grandmother used to walk like me with drop feet, and they often fell down...”
Documents
Copies of the main reports should be arranged chronologically and attached to the patient’s files.
Treatment(s)
The various treatments undergone in the past or currently being undergone should be noted. Drugs used to treat cardiovascular or other neurological or psychiatric problems can alter patient’s standing and walking abilities. All the effects mentioned by the patient on their walking abnormalities have to be listed (those of drugs, physical therapy, occupational therapy, fittings, crutches, orthoses, prostheses, and equipment of all kinds).
Assessment of lesion(s) affecting body structures
Based on the various reports collected, a full list of the patient’s lesions should be drawn up, including all the lesions that have occurred during the patient’s lifetime that are liable to have impaired their walking ability.
Assessment of impairments
The physical examination of the patients must include all the bodily systems (3). The aim is to find any deviations from normal structures and functions.
Any abnormalities detected should be correlated with the diagnosis. This will partly determine which modes of treatment will be chosen.
PRM physicians must pay special attention to the musculoskeletal system, the neurological system, the cardiovascular system, the respiratory and visual systems and the skin. All these possible sites of impairment can be linked to the lesions and may affect the patient’s activities, especially their gait (Fig. 1). PRM physicians must attempt to attribute each abnormality to a lesion affecting one of the systems listed above.
This examination must be exhaustive. Questions can be asked about pain (the type, location, intensity, etc.). The defective joint can be examined in both lower limbs in terms of: morphology, alignment (varum, valgum, flessum, recurvatum), range of motion, laxity (in the frontal, sagittal and coronal planes) (4). The muscle examination must include an assessment of: the morphology (amyotrophy), the tonus (hypotonia, hypertonia), the functional length (retraction), strength, and endurance. Sensory impairments can be assessed in terms of each sensory mode. The skin and the cutaneous trophicity also need to be examined.
Impairments can be quantitatively assessed using: the visual analogue pain scale, goniometers to quantify the range of joint motion, the modified Ashworth scale (5) to quantify muscle spasticity, and the Medical Research Council’s clinical method (6) to assess muscle strength.
Only after this examination has been completed will it be possible to assess the patients’ gait and other activities. All the symptoms noted are relevant to patients’ disabilities and the limitation of their activities, and help to understand their motor disorders.
HOW DOES HE/SHE WALK?
General information about gait
The aim of gait (7–13) is: to move from one place to another, and to do so as safely and as efficiently as possible. Four motor tasks have to be performed to obtain normal gait:
• propulsion and control of the forward progression of the body,
• absorption of energy to minimize the shock at foot strike,
• supporting the whole body on the lower limb during the stance phase,
• controlling the foot trajectory to adapt the joint position to the supporting surface (during the stance phase) and to ensure good foot clearance (during the swing phase).
The various phases of gait in a single lower limb are called the gait cycle. The gait cycle has 2 components: the stance phase (accounting for 60% of the gait cycle), which corresponds to the duration of foot contact with the ground, and the swing phase (accounting for 40% of the gait cycle), which is the period during which the lower limb oscillates without making contact with floor. The stance phase can be subdivided into 2 parts: the double support period (accounting for 20% of the gait cycle) during which both feet are in contact with the ground: this phase occurs at the beginning (10% of the gait cycle) and the end (another 10% of the gait cycle) of the stance phase; the single-limb support phase (accounting for 40% of the gait cycle), when the opposite foot is oscillating during the swing phase. These percentages of the gait cycle apply only to locomotion at self-selected comfortable speeds.
The spatial parameters involved in gait are defined as follows:
• step length: the distance covered during one step measured from initial contact of one foot to initial contact of the other foot; the left step length and right step length are symmetrical in normal subjects;
• stride length: the distance covered during one stride measured from initial contact of one foot to the next initial contact of the same foot; the left stride length and right stride length are symmetrical in normal subjects;
• step width: the distance between the 2 feet in the frontal plane.
The temporal parameters involved in gait are defined as follows:
• step time: the time measured from initial contact of one foot to initial contact of the other;
• stride time: the time measured from initial contact of one foot to the next initial contact of the same foot.
The walking speed has been defined as the average speed of the subject on a plane of progression (expressed in terms of distance/time). The comfortable walking speed or self-paced speed is the speed at which the energy cost per unit distance is minimum. Patients with walking abnormalities use many strategies to minimize the energy expenditure involved in normal walking.
During the swing phase, the aim is foot clearance and advancement of the limb. The clearance mechanisms used to control a swinging limb require specific events to lift the foot off the ground, namely hip and knee flexion and ankle dorsiflexion; stabilization of the pelvis is also crucial, and this is achieved by the pelvis abductors (including the gluteus medius), which control the pelvic drop that occurs during the swing phase. During the swing phase, the supporting limb uses several means of providing the other limb with sufficient clearance: performing ankle dorsiflexion and knee extension (for support) and raising the heel while performing ankle plantar flexion (for propulsion).
Qualitative functional assessment
Oral and written information
Patients' complaints and wishes: patients and their families are asked to prepare a written report listing all the ambulatory activities that are no longer possible, such as walking alone in the community, as well as the ambulatory activities that are still possible with the help of somebody else or using technical aids. It is also of interest to know what the patient wishes to be able to do: e.g. “I would like to be able to walk inside without the assistance of another person”.
Description of daily activities: this description must be collected carefully step by step, for the whole day, in order to determine how each of the daily activities is performed. It is worth obtaining this information first from the patient, and then from the family.
Clinical examination
Clinical examination focusing on the patient’s gait begins in the waiting room; the patient’s walking pattern is observed as they enter the consultation room.
The room used for the examination must be sufficiently large to be able to observe the patient in the frontal and sagittal planes.
Patients should be asked to wear only shorts in the case of men, and shorts and a bra in that of women. While the subject is walking, their feet, knees, hips, spine, arms, shoulders and head move synchronously to maintain balance and to move the body forward. All the body parts therefore have to be inspected to understand patients’ gait and/or their limping habits. Patients are assessed during the performance of various activities: the sitting position must be assessed before the others in order to observe the patients’ ability to maintain balance while sitting quietly and while being pushed in various directions.
Transferring is the ability to rise from sitting to standing, with or without the help of another person.
Standing is the ability to maintain a standing position. Do the patients need help? A lot of information can be obtained while helping somebody. Does the PRM physician have to exert vertical forces to support the patient in case of weakness or pain in a lower limb? Does the physician need to develop horizontal forces to support patients with equilibrium difficulties, or does he or she only have to touch the patient, to provide him or her with supplementary sensory information?
Dressing skills are a useful source of information. After obtaining the consent of the patients, it can be helpful to observe them while dressing or undressing the lower body. Patients with balance problems will need to be in a sitting position in order to put on their trousers and shoes.
Walking and performing other tasks are analysed if possible. The first walking speed tested should be the self-selected speed, and faster and slower ones should then be performed if possible. Walking faster or more slowly can increase the abnormalities or lead to a change in the walking strategies used. A subject can be asked to walk on uneven ground to increase the difficulty of the task. Ascending stairs is difficult for patients with leg muscle weakness (the hip flexors and ankle flexors are normally used to shorten the lower limb and the quadriceps and gluteus magnus to push the body upwards) and those with contractures during extension of the hip, knee or ankle. Descending stairs is difficult for those with weakness of the quadriceps and balance disorders. Whether they need to use a banister and to push with their hands on their knees is noted. Patients may also be asked to rise after lying on the floor. When the lower limb muscles are weak, as occurs in patients with muscular dystrophy, this kind of task can show whether patients would have difficulty in getting up after a fall.
The results of the qualitative functional assessment should be compared with the diagnosis and with the assessment of the impairment. The PRM physician needs to understand the compensatory strategies developed by the patient.
Gait disorders can be due to various factors, e.g. inefficient walking strategies, decreased safety levels, the presence of pain due to abnormal limb positions, instability, impaired balance, sensory deficits, weakness, insufficient limb clearance, limb deformities, anxiety, falling.
Walking abnormalities may be due, in the case of the stance phase, to an abnormal supporting base (ankle instability, equinus foot with toe contact), knee instability (knee buckling or hyperextension), hip instability (hip flexion or adduction); and in the case of the swing phase, to insufficient limb clearance (foot drop, toe drag) or impaired limb advancement (weakness, limited hip or/and knee flexion and ankle dorsiflexion).
Gait abnormalities (7) can be subdivided into stance phase dysfunction and swing phase dysfunction. In the case of the stance phase, the causes can include: an abnormal base of support, limb instability and trunk instability. In the case of the swing phase, they can include impaired limb clearance and impaired limb advancement.
Abnormal base of support. Equinovarus foot is a frequent occurrence in pathologies affecting the nervous system (upper motor neurone injury) or the musculoskeletal system. Contact with the ground is made by the forefoot, causing pain and instability. The knee can be hyper-extended during the stance phase. During the swing phase, there is a limb clearance problem, which requires compensatory strategies (increasing the hip flexion or the knee flexion; vaulting and hip hicking; hip abduction and semicircular gait).
Equinovalgus foot occurs in pathologies affecting the nervous system (upper motor neurone injury) and the musculoskeletal system. The foot contact involves the medial forefoot, resulting in pain in this area. The strategy used to compensate for the limb clearance deficits consists of increasing the hip and knee flexion.
Claw toes (flexion deformity of the toes) is a frequent occurrence in pathologies of the CNS, which results in pain during walking because of conflict with the shoe. The subject loads the limb gradually and shortens the step length and stance time on the affected side.
Extension of the great toe, i.e. hitchhiker’s great toe, is a frequent problem in patients with upper motor neurone complications, and this anomaly results in pain, changes in weight-bearing and abnormal push-off and forward propulsion towards final stance.
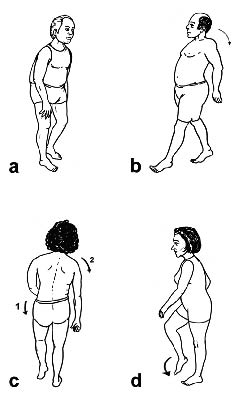
Limb instability. Limb instability can lead to knee collapse or hyperextension. The collapse can be associated with weakness of the quadriceps. It is one of the reasons for falls in patients with peripheral neuropathic or central neuropathic disorders. Sometimes the subjects have to push their knee back with their hand to lock the knee (Fig. 2a). Hyperextension of the knee can result either from weakness of the quadriceps, in which case the knee is hyperextended to block it, or from an equinus foot, which has biomechanical effects on the knee. Hyperextension of the knee is frequently associated with pain.
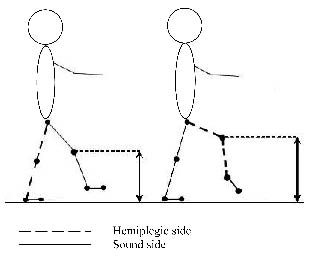
Trunk instability. Possible reasons for trunk instability include excessive hip flexion during the stance phase, hip extensor weakness when the position of the trunk is back with upper limb held at the back of the trunk (Fig. 2b), hip hiking to compensate for a limb clearance problem (Fig. 3) , and hip adduction, which can interfere with limb clearance and advancement. When the weakness affects the gluteus medius, Trendelenburg limping occurs: during the stance phase, the pelvis drops on the side of the oscillating limb and a lateral tilting of the trunk occurs (Fig. 2c).
Fig. 2. (a) Right quadriceps femoris weakness. The patient pushes his right knee with his hand in order to overcome quadriceps weakness and extend the knee during the stance phase of the gait cycle. (b) Gluteus maximus lurch. The patient uses trunk extension to compensate for gluteus maximus weakness. (c) Trendelenburg gait in a patient with right gluteus medius weakness. The inability of the right gluteus medius to stabilize the pelvis during right lower limb single stance phase results in contralateral pelvic drop (1). To limit the deviation of the centre of gravity towards the sound side due to the pelvic drop, the patient bends his trunk towards the weak side, shifting his weight over the supporting limb (2). (d) Steppage gait. Limb clearance impairment during the swing phase, due to lack of ankle flexion, is compensated for by excessive hip and knee flexion.
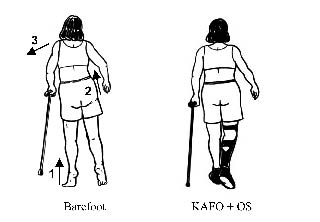
| Fig. 3. Qualitative and quantitative assessment of gait and balance in a multiple sclerosis patient with right hemiplegia. In the left-hand figure, the patient is shown walking barefoot with vaulting (1), hip hiking (2) and lateral trunk bending (3) strategies. A knee ankle foot orthosis (KAFO) was prescribed to correct a painful knee hyperextension and to improve the patient’s gait. In the right-hand figure, these 3 characteristics of pathological gait were improved due to the use of the KAFO and orthopaedic shoes (OS). The table gives the same patient’s gait analysis and posturographic parameters. There was a significant improvement in the gait velocity, step length and balance assessment parameters when the patient used her KAFO and OS. The difference in single support time between the lower limbs decreased when the test was performed with the patient wearing the KAFO and OS. SD: standard deviation. |
| |
| Gait analysis results |
| | Barefoot | KAFO + OS |
| Velocity (m/sec) | 0.39 | 0.90 |
| | Left | Right | Left | Right |
| Step length (cm), mean (SD) | 39 (7.39) | 45 (6.46) | 51 (3.66) | 66 (4.41) |
| Single support (sec), mean (SD) | 0.94 (0.08) | 0.44 (0.06) | 0.59 (0.05) | 0.38 (0.02) |
| Posturography results |
| | Barefoot | KAFO + OS |
| Area (cm2) Eyes open Eyes closed | | | | |
| 5.93 48.85 | | 1.16 1.63 | |
Limb clearance and advancement. Various compensatory strategies are used by patients with limb clearance and advancement problems. In hemiplegic patients with a stiff knee, the knee is kept extended during the swing phase of gait and the following compensatory mechanisms are used: a compensatory trunk and ipsilateral hip motion (the hip hiking that consists of elevating the hip of the swinging limb) and a contralateral limb motion (the vaulting that consists of going up on the toes on the stance side).
Hip circumduction is sometimes used during the swing phase to compensate for the lengthening of the limb resulting from a stiff knee and inadequate hip flexion.
Another strategy used by hemiplegic subjects consists of increasing the hip adduction to compensate for the reduced hip flexion ability during limb advancement.
Drop foot is associated with a lack of dorsiflexion during the swing phase. This kind of limping is called steppage when the hip and knee flexion is increased to compensate for the drop foot (Fig. 2d).
Digital video evaluation
These walking and standing parameters are usually not quantified. The events are either not conspicuous enough or occur too fast to be perceived during clinical assessment. It is therefore necessary to carry out a quantitative functional assessment. With the advent of digital video cameras and dedicated software programmes, slow motion video capture and data storage and retrieval are now possible. Slow motion is of interest for analysing and comparing clinical parameters on different occasions. One year after a video is shot, it can be used to analyse the changes in a patient’s gait (improvement or worsening). For ethical reasons, the patients must be asked to give their informed consent in writing prior to video recording sessions.
Quantitative functional assessment
A quantitative functional assessment can be carried out using either appropriate scales or the latest tools and methods for quantitatively assessing posture and movement. Generic scales such as the Functional Independence Measure (14) can be used to assess activities in general.
Scale for assessing walking
PRM physicians studying individuals or groups of patients can use suitable scales. These scales can either be applicable to all types of patients, in which case they are called generic scales, or to a single type of patient, in which case they are called specific scales.
Clinical balance and mobility tests. Clinical tests have been developed for investigating the maintenance of the standing position during quiet stance with eyes open or eyes closed (Romberg test), to assess the ability to perform voluntary movements and to measure the time taken to complete manoeuvres including complex sequences of functional movements, e.g. the Timed Up and Go test (TUG) (15). In addition, the Functional Ambulation Categories (FAC) (16) provides a simple index to mobility, and timed walking tests can also be used to analyse speed, endurance and cardiorespiratory fitness.
• Timed Up-and-Go test: TUG (15) can be used to assess a subject’s ability to maintain balance during transfer and gait, using a stop-watch to measure the time taken to perform the task. The task consists of standing up from a chair, walking 3 m, turning 180°, returning and sitting down. During the performance of the test, subjects are allowed to use their usual walking aid. One training trial and 2 assessment trials are performed. The time taken by the subject is the mean value obtained in the 2 assessment trials. TUG showed a good level of reliability and responsiveness after specific training, and high levels of sensitivity and specificity in detecting patients who are likely to fall. The results depend on the type of shoes, chair and walking aids used. In addition, it does not measure patients’ “pure balance” abilities, but their performance of a series of different motor tasks. The “total time” used as the sole outcome measure may therefore mask specific deficits occurring in single tasks and manoeuvres (such as standing up, turning, etc.). The Expanded Timed "Up & Go" test is therefore recommended to time the single components (e.g. from sitting to standing, gait initiation, turning around) of the task, using a multi-memory stopwatch.
• Functional Ambulation Categories: the FAC (16) were designed for use in therapeutic environments in order to record the amount of personal assistance required by patients when walking. There are 6 ordinal categories, ranging from “0 – unable to walk” to “5 – independent walking”. This instrument is simple to use in clinical practice, and its validity and reliability have been clearly established, as well as its sensitivity to change during the transition from immobility to walking. To decrease the ceiling effect of the FAC, some authors, such as Brun et al. (17), have proposed a new FAC with 9 categories ranging from “0 – unable to walk” to “8 – independent on stairs”.
Multi-item ordinal scales for assessing balance, mobility and gait. Clinical balance tests are helpful for documenting balance status and the changes occurring as the result of interventions. Multi-item ordinal scales provide useful tools, as they can easily be used to determine simple everyday task performances. The subjects’ performances in a set of motor tasks are usually rated on a 3–5-point scale or with a stop-watch to time how long balance can be maintained in a particular posture. Two of the most commonly used functional balance and gait assessment tools are the Berg Balance Scale (BBS) (18, 19) and Postural Assessment Scale for Stroke Patients (20).
• Berg Balance Scale (18): this is the most widely used of these scales, and has been validated as a balance assessment tool. It includes 14 items relating to balance performance and requires subjects to maintain positions of varying difficulty and perform specific tasks, such as standing and sitting unassisted, as well as tasks including transition phases, such as moving from sitting to standing and vice versa, turning to look over the shoulder, picking up an object from the floor, turning 360° and placing alternate feet on a stool. The score is based on the subject’s ability to perform the 14 tasks independently and/or to meet given time or distance requirements. Each item is scored on a 5-point ordinal scale ranging from 0 (unable to perform) to 4 (normal performance) so that the aggregate score ranges from 0 to 56: the higher the score, the better the performance. The BBS takes 15 min to administer. Inter-rater reliability and internal consistency are high. Test-retest reliability in hemiparetic patients are also high. Concurrent validity has been assessed in comparison with the Fugl-Meyer test and the Postural Assessment Scale for Stroke Patients. Construct validity has been assessed by correlating the BBS with other disability scales, and has proved to be fairly high with the Barthel Index (21), TUG, Tinetti balance subscale and Dynamic Gait Index, gait velocity and measures of centre of foot pressure. Moreover, the BBS is sensitive to changes in stroke patients’ performance (after 14–90 days) and is appropriate for use with subjects with central vestibular dysfunction (22). Patients with central or peripheral vestibular dysfunction were found to have a high, medium and low risk of falling, corresponding to scores of 0–20, 21–40 and 41–56, respectively (18). In another paper, a score of 45 was found clearly to separate elderly subjects with a risk of falling from those not at risk (23). In any case, BBS has proved to be a more powerful functional test than TUG for discriminating between elderly fallers and non-fallers (24).
• Postural Assessment Scale for Stroke Patients: the Postural Assessment Scale for Stroke patients (PASS) (20) was based on the Fugl-Meyer assessment of balance and mobility (FMA), and has been developed with 3 main ideas in mind: (i) the ability to maintain a given posture and to maintain balance while changing position must both be assessed; (ii) the scale should be applicable to all patients, including those with very poor postural performance; and (iii) it should contain items with increasing levels of difficulty. The PASS contains 12 4-level items of various levels of difficulty for assessing the ability to maintain or change a given lying, sitting, or standing posture. Items 1–5 examine the ability to maintain a posture (sitting without support, standing with support, standing without support, standing on the non-paretic leg and standing on the paretic leg). The remaining 7 items analyse the ability to change posture (from supine to the affected side, from supine to the non-affected side, from supine to sitting up on the edge of the table, from sitting on the edge of the table to supine, from sitting to standing up, from standing to sitting down, and picking up a pencil from the floor). The PASS method has been found to be suitable for assessing the postural abilities of stroke patients during the first few months after stroke in both neurological and rehabilitation contexts (20). The PASS method was recently found to show similar or slightly better psychometric characteristics than the BBS and FMA (25).
Gait assessment tools and methods
Four quantitative methods can be used to assess gait, focusing on the kinematic and kinetic parameters, electromyographic data and energy expenditure (7–13, 26–31):
• Kinematic methods: analysis of temporal and spatial measures and motion analysis, focusing on the time and space aspects of the motion pattern. The temporal and spatial parameters can be assessed, and methods of motion analysis used. To assess the temporal and spatial parameters, the methods available include: ink and paper methods, foot switches, an instrumented walkway that can be used in clinical practice, or more sophisticated systems involving patient instrumentation. The aim of motion analysis systems is to obtain a quantitative description of the motion of body segments by placing markers on the body, which are detected by optoelectronic systems (Fig. 4). Various techniques can also be used, such as photographic and cinematographic techniques, accelerometers and goniometers (32). The latest systems involve the use of a high-speed camera along with either passive markers (infrared-reflecting markers placed on the body segments) or active markers. After the data acquisition step, the second step consists of tracking the markers (which is a time-consuming task) to describe the subject’s movements. With systems of this kind, it is possible to determine the joint angles, linear and angular velocities, and patterns of acceleration. Combined kinetic information methods yield the moments (the forces acting on a joint), powers, mechanical energy and energy transfer data. These systems of data acquisition used to determine kinematic parameters are frequently too complex (they are too time-consuming, and involve the apparatus being placed on the subject) to be used in clinical applications, but they provide useful research tools.
Fig. 4. Example of kinematic assessment in a hemiplegic subject. During the swing phase, the knee is lifted higher on the hemiplegic side than on the sound side to compensate for the equinus (29).
• Kinetic parameters: analysis of the forces and loads triggering motion. To record kinetic parameters, force plates can be used along with strain gauges or piezoelectric elements. The ground reaction forces, which are the opposite reaction to the force applied by the subjects on the force plate, can be recorded. The focal point where the ground reaction forces are applied is known as the centre of pressure. Two types of force can be recorded: vertical forces (which are similar to the body weight) and medial-lateral and anterior-posterior shear forces (propulsion or breaking forces) (Fig. 5). Other relevant kinetic parameters include the pressure (force/area) exerted under the foot, but to determine these parameters, force plates do not suffice: special footwear equipped with pressure sensors is required to measure the forces exerted under different parts of the foot (sensor insoles cannot be used to determine the spatial parameters), or walkways with sensors embedded (some of these devices include more than 10,000 sensors on the active surface, and they can be used to determine not only the pressure but also the spatial and temporal gait parameters without requiring any calibration) (Fig. 3).
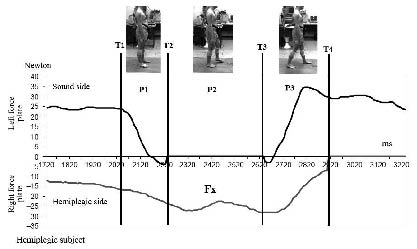
Fig. 5. Example of an Fx curve (Fx is the medio-lateral component of the ground reaction force in the horizontal plane) recorded in a hemiplegic subject during gait initiation. The 3 phases P1, P2 and P3 are: the postural phase (PI) starting at time Tl, corresponding to the onset of the peak in Fx (left force plate), which corresponds to the start of the weight transfer phase, and ending at time T2, corresponding to the end of the force plate recording of the moving leg (left force plate); the monopodal phase (P2) starting at time T2 and ending at time T3, corresponding to the initial contact of the moving leg, when the force plate recording started up again (left force plate); and the double-support phase (P3) starting at time T3 and ending at time T4 with the take-off of the supporting leg, when no further signals were recorded on the other force-plate (right force plate) (29).
• Electromyographic (EMG) methods: analysis of muscle activities and identification of the timing and relative intensity of muscle activity. EMG recordings provide a useful means of determining muscle activation patterns during gait. The activity of superficial muscles can be recorded with surface electrodes and that of deep muscles with fine-wire electrodes. Some EMG systems are telemetric.
• Oxygen consumption: energy expenditure analysis provides a useful means of determining the cost of walking to subjects equipped with prostheses or orthoses, or the cost of walking to patients with various pathologies.
All of these tools can be used in various combinations.
The following tools are required for gait assessment purposes at PRM departments:
• Room standards (dimensions, light, walls, equipment such as stairs with 2 banisters, 5- and 10-m lines on the floor).
• A chronometer.
• A walkway equipped with pressure sensors is useful for making routine assessments and recording the temporal and spatial parameters of gait and the pressure under the patients' feet.
• Optoelectronic cameras and markers that can be glued onto anatomic landmarks on the patient's body to obtain kinematic data.
• Force platform(s): with 2 force plates, one can assess the weight distribution under each lower limb and the standing equilibrium. Ground reaction forces can also be recorded in this way during the stance phase of walking.
• EMG equipment to record the activity of the muscles of interest throughout the gait cycle, using contact electrodes.
• Oxygen consumption measurements during gait can be carried out comfortably for the patient using easy-to-wear devices.
The tasks performed in these tests could include: walking at different speeds with and without walking aids, wearing orthopaedic shoes, orthoses, going up and down stairs.
With these tools, data of various kinds can be obtained, such as:
• temporo-spatial parameters, step length and width, single and double support durations;
• kinematic parameters (such as the knee height in stroke patients during the swing phase);
• kinetic parameters (such as the foot pressures, vertical forces while landing in knee arthritis patients, sagittal forces in stroke patients, displacement of the centre of pressure);
• EMG activities;
• energy parameters (such as the oxygen consumption rates before and after orthopaedic surgery on the lower limbs in children with cerebral palsy).
The most frequent changes in the gait parameters observed in patients with abnormal gait are a decrease in the walking speed, asymmetrical steps, a decrease in weight-bearing in the limb involved, an increase in the oxygen consumption rates, and changes in the EMG patterns.
WHAT ARE THEIR LIVES LIKE?
It is of great interest for PRM physicians to assess the level of participation of disabled persons in various activities in their usual home environments, outside the PRM department. This information can be obtained directly from the patients and their families (Fig. 1).
It is important to assess what is the disabled person’s level of participation in activities at home, at work (if relevant), during holidays, and in sports, cultural, religious and political activities.
Development of ambulatory posture and movement monitoring methods: new tools and methods are currently being developed for quantifying posture and movement parameters after a disabled person has left the PRM department. These methods based on accelerometers and gyroscopes make it possible to record the activities of a disabled person at home for long periods. Further improvements are required before their routine clinical use becomes possible, in line with the devices used in the field of cardiology for permanently monitoring patients’ heart activity and blood pressure.
The scales that can be used to assess patients’ participation include the Craig Handicap Assessment and Reporting Technique (CHART) scale used to assess the participation of patients with traumatic brain injuries (33).
Assessing environmental factors
There are 2 main methods of assessing environmental factors: a detailed written report prepared by the family, and a visit to the patient’s home. Two main types of environmental factors are involved: human and physical.
Human factors
Members of the patients’ close family are asked to write a day-to-day report describing the support given to the disabled person. This can be direct physical assistance with daily activities or new ways of organizing everyday activities within the family. The support provided by friends, acquaintances, peers, colleagues, neighbours and community members also has to be assessed. The support provided by health professionals and health-related professionals must also be recorded in detail. Attitudes of close family members, friends and caregivers are not constant, and therefore have to be re-assessed from time to time.
Material environmental factors
PRM physicians should assess the changes in their patients’ walking abilities that occur when they are walking on various surfaces and in various environments. The layout of a patient’s home can give rise to problems. For example, if there are stairs in the home the subject may have difficulty in going up and down these stairs. Occupational environments also have to be assessed in order to prevent risks (the risk of falling, for instance). It may be necessary either to alter the environment or to decide to change the tasks that have to be performed (weight-lifting should be avoided, for instance). Special products and equipment may be required by disabled persons for their personal use in everyday life, to improve their personal indoor and outdoor mobility and help them with their transport problems.
The scales that can be used to assess participation include the Craig Hospital Inventory of Environmental Factor (CHIEF) scale (34), which was designed to assess the environmental factors involved in the case of patients with traumatic brain injuries.
Assessing quality of life
Walking ability, which is part of patients’ functional status, can be one of the main predictors of quality of life (QoL), in the case of stroke patients, for instance. QoL can be assessed using the QoL Visual Analogue Scale or the SF-36 questionnaire.
WALKING REPORT
Report on patients with walking abnormalities: who they are, how they walk and what their lives are like
At the end of the assessment process, PRM physicians must write a report on the lesions liable to interfere with the patient’s walking abilities, the main impairments that have been assessed and quantified, the qualitative and quantified walking parameters, the limitations to the patient’s participation and quality of life, which results partly from gait abnormalities. PRM physicians should present and explain the results of their assessment and their conclusions to the patients and their families.
At the end of this report, a treatment programme will be proposed to the patient, which will take into account the patient’s lesions and impairments (who is the patient?), their locomotor abilities (how does he/she walk?) and their environment and participation (what is their life like?).
PRM physicians will draw up a treatment programme based on the assessment, which will be explained to the patient and the family. With the agreement of the patient, the report will be transmitted to the care-givers. Further assessments of the patient’s walking abilities will enable the PRM physician to determine whether the patient has improved as the result of this treatment. Examples of possible treatments are: a rehabilitation programme, medication, botulinum toxin injection, fittings, or surgery.
Options for surgery can include:
• treatment of lesions, by applying an arthrodesis to an unstable and painful equino varus foot;
• treatment of impairments, by strengthening a weak quadriceps;
• treatment of abilities, by prescribing rehabilitation to improve equilibrium in a patient with a damaged cruciate knee ligament, etc.
The PRM physician's conclusions will be compared with the patient's personal impressions.
CONCLUSION
Gait abnormalities should be assessed on the basis of an exhaustive clinical examination. After a full assessment of the lesions, this examination should be carried out in line with the ICF model, including: impairments (body functions and body structures), activities and participation, environmental factors, as well as the patients' complaints and wishes, their personal data, past medical history, lesions, and QoL. This assessment can be completed by performing instrumental assessments to obtain quantified data. Gait analysis using clinical and instrumental methods and accurate diagnosis is necessary to be able to select appropriate interventions, design gait re-training programmes, assess the effectiveness of a treatment or a fitting, develop objective criteria for long-term management options (criteria for deciding about surgical interventions, for example), follow up patients and monitor the progression of their gait abnormalities over time.
ACKNOWLEDGEMENTS
Pr Franco Franchignoni, Unit of Occupational Rehabilitation and Ergonomics, Salvatore Maugeri Foundation, Clinica del Lavoro e della Riabilitazione, IRCCS, Veruno, Italy has contributed with suggestions in the preparation of this educational review.
REFERENCES
1. World Health Organization. International classification of functioning, disability and health. ICF full version. Geneva: WHO; 2001. Available from: http://www.who.int/classifications/icf/site/
2. Gutenbrunner C, Ward AB, Chamberlain MA. White book on physical and rehabilitation medicine in Europe. J Rehabil Med 2007; Suppl 45: 6–47.
3. Delarque.A, Pellas.F. Bilan fonctionnel des membres inférieurs. In: Held JP, Dizien O, editors. Traité de médecine physique et de réadaptation. Paris: Flammarion; 1998, p. 119–131.
4. Delarque.A, Viton.JM. Bilan articulaire des membres. In: Held JP, Dizien O, editors. Traité de médecine physique et de réadaptation. Paris: Flammarion; 1998, p. 30–42.
5. Bohannon RW, Smith MB. Interrater reliability on a modified Ashworth scale of muscle spasticity. Phys Ther 1987; 67: 206–207.
6. Medical Research Council. Aids to the examination of the peripheral nervous system. Memorandum number 45. London: Her Majesty’s Stationary Office; 1976.
7. Esquenazi A, Talaty M. Normal and pathological gait analysis. In: Grabois M, editor. Physical and rehabilitation: the complete approach. Malden (MA): Blackwell Science; 2000, p. 242–262.
8. Baker R. The history of gait analysis before the advent of modern computers. Gait Posture 2007; 26: 331–342.
9. Baker R. Gait analysis methods in rehabilitation. J Neuroeng Rehabil 2006; 3: 4.
10. Inman VT, Ralston HJ, Todd F, editors. Human walking. Baltimore: Williams & Wilkins; 1981.
11. Perry JP, editor. Gait analysis: normal and pathological function. Thorofare, NJ: Slack; 1992.
12. Whittle MW, editor. Gait analysis: an introduction, 2nd edn. Oxford: Butterworth-Heinemann; 1996.
13. Winter DA, editor. The Biomechanics and motor control of human gait: normal, elderly and pathological. Waterloo (Ontario): University of Waterloo Press; 1991.
14. Hamilton BB, Granger CV, Sherwin FS, Zielezny M, Tashman JS. A uniform national data system for medical rehabilitation. In: Fuhrer MJ, editor. Rehabilitation outcomes. analysis and measure. Baltimore: PH Brookes Publishing Co.; 1987, p. 135–147.
15. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39: 142–148.
16. Holden MK, Gill KM, Magliozzi MR. Gait assessment for neurologically impaired patients. Standards for outcome assessment. Phys Ther 1986; 66: 1530–1539.
17. Brun V, Mousbeh Z, Jouet-Pastre B, Benaim C, Kunnert JE, Dhoms G, et al. Clinical assessment of stroke hemiplegic gait: suggestion for a modification of the functional ambulation classification. Ann Readapt Med Phys 2000; 43: 14–20.
18. Berg K, Wood-Dauphinee S, Williams JI, Maki B. Measuring balance in the elderly: Validation of an instrument. Can J Public Health 1992; 83 Suppl 2: S7–S11.
19. Franchignoni F, Velozo CA. Use of the Berg Balance Scale in rehabilitation evaluation of patients with Parkinson’s disease. Arch Phys Med Rehabil 2005; 86: 2225–2226.
20. Benaim C, Pérennou DA, Villy J, Rousseaux M, Pelissier JY. Validation of a standardized assessment of postural control in stroke patients: the Postural Assessment Scale for Stroke Patients (PASS). Stroke 1999; 30: 1862–1868.
21. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J 1965; 14: 61–65.
22. Whitney S, Wrisley D, Furman J. Concurrent validity of the Berg Balance Scale and the Dynamic Gait Index in people with vestibular dysfunction. Physiother Res Int 2003; 8: 178–186.
23. Bogle Thorbahn LD, Newton RA. Use of the Berg Balance Test to predict falls in elderly persons. Phys Ther 1996; 76: 576–583.
24. Chiu AY, Au-Yeung SS, Lo SK. A comparison of four functional tests in discriminating fallers from non-fallers in older people. Disabil Rehabil 2003; 25: 45–50.
25. Mao HF, Hsueh IP, Tang PF, Sheu CF, Hsieh CL. Analysis and comparison of the psychometric properties of three balance measures for stroke patients. Stroke 2002; 33: 1022–1027.
26. Sutherland DH. The evolution of clinical gait analysis part I – kinesiological EMG. Gait Posture 2001; 14: 61–70.
27. Sutherland DH. The evolution of clinical gait analysis part II – kinematics. Gait Posture 2002; 16: 159–179.
28. Sutherland DH. The evolution of clinical gait analysis part III – kinetics and energy assessment. Gait Posture 2005; 21: 447–461.
29. Bensoussan L, Mesure S, Viton JM, Delarque A. Kinematic and kinetic asymmetries in hemiplegic patients’ gait initiation patterns. J Rehabil Med 2006; 38: 287–294.
30. Luc M, Bensoussan L, Viton JM, de Bovis VM, Collado H, Pouget J, et al. Gait recovery in a distal spinal muscular atrophy patient wearing a patellar tendon-bearing orthosis and orthopaedic shoes. J Rehabil Med 2007; 39: 181–184.
31. Bensoussan L, Viton JM, Schieppati M, Collado H, Milhe de Bovis V, Mesure S, et al. Changes in postural control in hemiplegic patients after stroke performing a dual task. Arch Phys Med Rehabil 2007; 88: 1009–1015.
32. Tesio L, Monzani M, Gatti R, Franchignoni F. Flexible electrogoniometers: kinesiological advantages with respect to potentiometric goniometers. Clin Biomech (Bristol, Avon) 1995; 10: 275–277.
33. Whiteneck GG, Charlifue SW, Gerhart KA, Overhosler JD, Richardson GN. Quantifying handicap: a new measure of long-term rehabilitation outcomes. Arch Phys Med Rehabil 1992; 73: 519–526.
34. Whiteneck GG, Harrison-Felix CL, Mellick DC, Brooks CA, Charlifue SB, Gerhart KA. Quantifying environmental factors: a measure of physical, attitudinal, service, productivity, and policy barriers. Arch Phys Med Rehabil 2004; 85: 1324–1335.
| Multiple choice questions (MCQ) |
| 1. | Which of the following statements about scales for assessing walking is correct? |
| | a) The Functional Independence Measure is a specific scale. |
| | b) The Functional Ambulation Categories assess the ability to stand up from a chair, walk 3 m, and turn 180°. |
| | c) The Postural Assessment Scale for Stroke Patients includes 14 items relating to balance performance. |
| | d) The Postural Assessment Scale for Stroke Patients was based on the Berg Balance Scale. |
| | e) Berg Balance Scale has proved to be a more powerful functional test than the Timed Up and Go test for discriminating between elderly fallers and non-fallers. |
| 2. | Which of the following statements about gait in healthy adults is correct? |
| | a) In quadriceps weakness, the typical limping pattern is the steppage pattern. |
| | b) The swing phase duration is greater than the stance phase duration. |
| | c) The stance phase accounts for 40% of the gait cycle and the double support period accounts for 20%. |
| | d) The stride length is measured from the left to the right foot. |
| | e) The step width is the distance between the 2 feet in the frontal plane. |
| 3. | In a subject with a completely defective right quadriceps muscle responsible for frequent falls, what kind of compensatory strategy can be used to avoid knee collapse? |
| | a) Never extending the knee joint. |
| | b) Backward trunk bending before initial contact. |
| | c) Pushing with the hand on the knee back. |
| | d) Flexion of the knee before initial contact. |
| | e) Lateral trunk bending before initial contact. |
| 4. | Which of the following statements about kinematic methods is untrue? |
| | a) They can be used to assess the temporal and spatial parameters of gait. |
| | b) Goniometers can be used for kinematic assessments. |
| | c) Kinematic parameters can be obtained with accelerometers. |
| | d) Ink and paper methods can be used to obtain kinematic parameters. |
| | e) Only passive markers can be used with optoelectronic systems. |
| Correct answers: 1:e, 2:e, 3:c, 4:e. |