OBJECTIVE: The effects of stroke on stroke survivors are profound and cannot adequately be understood from a single approach or point of view. Use of qualitative study, in addition to quantitative research, provides a comprehensive picture of the consequences of stroke grounded in the experience of stroke survivors. The purpose of the present study was to examine the contribution of the published qualitative literature to our understanding of the experience of living with stroke.
DESIGN: Qualitative meta-synthesis.
Method: A literature search was conducted to identify qualitative studies focused on the experience of living with stroke. Themes and supporting interpretations from each study were compiled and reviewed independently by 2 research assistants in order to identify recurring themes and facilitate interpretation across studies.
RESULTS: From 9 qualitative studies, 5 inter-related themes were identified as follows: (i) Change, Transition and Transformation, (ii) Loss, (iii) Uncertainty, (iv) Social Isolation, (v) Adaptation and Reconciliation.
CONCLUSION: The present synthesis suggests the sudden, overwhelming transformation of stroke forms a background for loss, uncertainty and social isolation. However, stroke survivors may move forward through adaptation towards recovery. Meta-synthesis of qualitative research is needed to promote the inclusion of what we know about patient preferences and values in evidence-based practice.
Key words: qualitative study, stroke, rehabilitation.
J Rehabil Med 2008; 40: 595–602
Correspondence address: Katherine Salter, Research Associate, Centre for Aging, Rehabilitation and Geriatric Research, Room B-3019-c, Parkwood Hospital, 801 Commissioners’ Road East, London, Ontario, Canada N6C 5J1. E-mail: katherine.salter@sjhc.london.on.ca
Submitted November 2, 2007; accepted May 5, 2008
Introduction
Studies that have investigated stroke outcomes have historically focused primarily on physical functioning or functional ability in terms of activities of daily living (1–3). This approach represents a restricted definition of recovery. In recent years, there has been interest in an expanded range of outcomes in the study of recovery, including health status, social participation or quality of life and the use of an increasing number of patient-centred assessments. Unfortunately, most assessments of outcome still rely on the use of standardized questionnaires comprised of pre-determined questions, presumed to be of importance to the individual, with closed response sets (2, 4). Within this traditional model of outcome assessment, the healthcare professional, rather than the individual with stroke, is the “expert”. As a result, while much may be known about the impact of stroke on outcomes such as functional ability, for example, less is known about what this means to the individual who has experienced the stroke (5, 6).
The effects of stroke on the stroke survivor are profound and cannot be understood adequately from a single approach or point of view. Rather, multiple ways of understanding the experience of individuals with stroke should be considered. Use of qualitative study, in addition to quantitative research, provides a more comprehensive picture of the consequences of stroke, grounded in the experiences and perspectives of stroke survivors (7). This expanded understanding of stroke is essential in the development of interventions and services that are relevant to the individual stroke survivor. Findings of qualitative studies, therefore, should be included in the process of review and synthesis for the development of evidence-based practice (2, 7–9).
Meta-synthesis is a process of examination, comparison and interpretation of the findings of published qualitative studies intended to advance understanding of a selected topic of interest (10–13). Although the specific methodology continues to evolve, the process of meta-synthesis may represent a way to make the body of knowledge derived from qualitative study more accessible to clinicians, researchers and policymakers, thereby moving these findings toward inclusion in evidence-based practice (9, 14). At the present time, although descriptive reviews of the qualitative literature are available (1, 7), no published meta-syntheses of findings concerning the experience of living with stroke could be located. The purpose of the present study was to examine the contribution of the published qualitative literature to our understanding of the experience of living with stroke, through a process of meta-synthesis.
Methods
Based on previously published descriptions of process (10, 12, 15, 16), the present meta-synthesis comprised 3 steps: (i) identifying published papers for inclusion, (ii) quality appraisal and data extraction, and (iii) summarizing and synthesis.
Identifying published papers for inclusion relevant to the focus of study
The following electronic databases were searched for the years 1980–2007 using the text phrases “stroke” or “cerebrovascular accident” and “qualitative”: PubMed, Current Index to Nursing and Allied Health Literature (CINAHL), PsychInfo and Web of Science. The electronic literature search was supplemented by hand-searching reference lists from identified papers. To determine suitability for inclusion, the following screening questions were applied to each article (12, 15): (i) Does the paper report findings of qualitative research involving qualitative methods of data collection and analysis? (ii) Is the focus of the paper suited to the synthesis topic? Papers were considered for inclusion only if they reported the use of accepted qualitative methods to explore the experience of living with stroke from the perspective of individuals who had experienced stroke. Studies whose reported focus was from the perspective of caregivers, family members, or healthcare professionals were excluded, as were studies examining other, related topics, such as processes or goals for recovery and rehabilitation, satisfaction with care or availability of resources.
Although some authors do not recommend inclusion of studies using varying qualitative methods (11), others suggest that the findings themselves are of more importance and synthesis across perspectives provides the opportunity to enrich our understanding (13, 14, 17). All forms of qualitative study are interpretive and seek to enrich understanding and knowledge of the experience of a given group of individuals (10). Since meta-synthesis is based on multiple sources, methods, researchers and theories, it represents a form of triangulation, a method used to reduce bias, promote trustworthiness and enhance comprehensiveness of qualitative study (18, 19). Therefore, studies were not excluded or included on the basis of the reported qualitative methods employed. However, studies reporting the use of mixed methods (i.e. a qualitative component used to supplement a quantitative study) were excluded (15). In addition, studies consisting of uninterpreted stories or excerpts, or containing findings restricted to countable or codable remarks organized by interview question or prevalence of topic category were excluded. To be included, reports had to demonstrate an effort to describe themes or patterned responses based on topics raised by participants rather than simply classifying and counting responses (9, 20).
Quality appraisal and data extraction
While it is acknowledged that the quality of study used in any meta-analytic approach may influence the result, there is no definitive set of guidelines or simple checklist of elements with which to assess qualitative research. Indeed, the application of a checklist approach to quality assessment within qualitative research remains controversial (19). Given that application of rigid exclusion criteria on the basis of quality risks the loss of valuable and relevant findings, Sandelowski et al. (17) suggested that quality assessment in meta-synthesis should use criteria so general that they may be applied equally to any qualitative study. Accordingly, 2 core selection criteria have been proposed (14). First, information provided should support the notion that the research in question was conducted using accepted qualitative methods and, secondly, reported findings should appear to be well supported by the raw data (participant quotations). All articles identified in stage (i) were assessed using these 2 criteria for study quality. Studies that failed to meet either criterion were excluded.
Following a comprehensive review of the literature focusing on qualitative research methods, Murphy et al. (19) concluded that there are 2 main criteria that should be applied in the evaluation of qualitative research: credibility and relevance. Studies that met the core criteria for quality were subjected to further scrutiny using the following series of 7 questions based on the results of this review (19, 21).
Credibility.
• Were explanations of sampling strategies and data collection methods provided?
• Was the method of data analysis described and enough data displayed to allow the reader to determine whether the interpretations made by the researcher are supported by the data (auditability)?
• Did the authors acknowledge the influence of the research process and the presence of the researcher including the role of prior biases, assumptions and experience, on the collected data (reflexivity)?
• Has appropriate attention been given to contradictory data? Are negative cases taken into account?
• Did the authors explore alternative, plausible explanations for the data collected and incorporate a range of different perspectives (fair dealing)?
Relevance.
• Did the authors provide information regarding participants, setting and context so that the reader might be able to determine the relevance of the findings to other settings (transferability)?
• Did the authors discuss findings within a broader context, propose generalization of findings and/or suggest a direction for future research (analytic generalization)?
Two research associates (K.S. and C.H.) conducted the review of study quality. Results of the individual quality reviews were discussed and discrepancies resolved by consensus. In addition, the following information was extracted from each article: number and description of participants; format and setting for data collection; and type of analysis reported. Lists summarizing the original findings, themes, issues, concepts and interpretations were created for each of the selected papers.
Summarizing and synthesis
The synthesis of qualitative research has been described as the bringing together of findings on a chosen theme based on published findings rather than primary data (12). We chose to proceed with a descriptive meta-synthesis in which unaltered texts of research reports form the data for analysis and published findings are not deconstructed prior to synthesis (14). Lists of identified themes, important issues and concepts and supporting interpretations from all studies were reviewed independently by 2 research associates (K.S. and C.H.) in order to identify prominent, recurring themes across study findings. Working interactively, the 2 researchers then coded and reviewed identified themes within the context of the compiled lists in an iterative manner until no new themes could be identified.
Results
Identifying published papers for inclusion relevant to the focus of the study
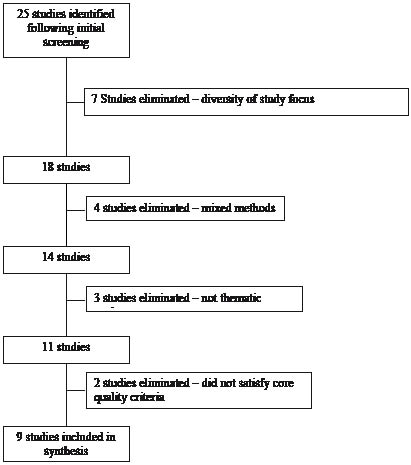
Titles and abstracts from the results of the initial searches were reviewed to determine suitability for inclusion according to the established criteria. Twenty-five studies were identified that reported the results of qualitative research (screening question (i)) concerning the experience of living with stroke from the perspective of the stroke survivor (screening question (ii)).
On closer examination, 7 additional studies were eliminated on the basis of relevance of study focus to the synthesis topic (22–28). Four studies reported the use of mixed methods (5, 29–31) and an additional 3 studies (2, 32, 33) presented findings more in keeping with a topical survey, rather than a thematic analysis (20), and provided results as frequency of countable or codable remarks within categories. These 7 studies were also excluded. Therefore, 11 studies remained for the second step.
Quality appraisal and data extraction
All 11 studies identified for inclusion in step (i) reported the use of accepted qualitative methods for data collection and analysis. However, 2 studies did not meet the second core criterion and did not provide sufficient data to support the findings reported (34, 35) (see Fig. 1). Therefore, 9 studies (8, 36–43) were included for data extraction and more detailed quality assessment. Recorded features of included studies appear in Table I, while the consensus results of the quality assessment are presented in Table II.
Fig. 1. Final selection of studies.
| Table I. Features of studies included for analysis |
| Study | n | Participants | Setting and format for data collection | Data analysis style reported |
| Becker 1993 (36) (USA) | 100 | 64 women, 36 men; aged 50–105 years, 52% were married, 48% had 2 or more chronic conditions. Informants were participating in 2 related studies (64 from one, 36 from the other). | Semi-structured interviews lasting approximately 1 h. In the first group (n = 64), participants were interviewed in hospital as soon as they were medically stable. In the second (n = 36), interviews began at approximately 4 months post-stroke. All participants were followed for 12 months. Interviews were conducted in hospital units and in participants’ homes. | Thematic analysis following the systematic approach of Kaufman. |
| Häggström et al. 1994 (37) (Sweden) | 29 | 19 men, 10 women; aged 60–91 years, 18–22 months post-stroke, most living at home with spouse at time of study, 62% had an eating disorder. | Participant observation and semi-structured interviews based on the presentation of 2 photographs. 27 interviews were conducted in participant home, 2 in an institutional setting. | Thematic analysis based on theory of phenomenological hermeneutics. |
| Secrest & Thomas 1999 (38) (USA) | 14 | 7 men, 7 women; aged 40–93 years, 9 to 23 years post-stroke. All had completed inpatient rehabilitation, were living at home and were independent in ADLs, though with continuing deficits. 8/14 participants had some aphasia. | In-depth interviews lasting 1.5–2 h, were conducted in either the private homes of the participants or the offices of the researcher, as per participant preference. | Thematic analysis according to existential phenomenological theory. |
| Pilkington 1999 (39) (Canada) | 13 | 9 men, 4 women, aged 40–91 years, admitted to hospital with stroke. | Series of 3 semi-structured interviews, each lasting approximately 20–90 min. First interviews were conducted during hospital admission, then at 1 and 3 months post-stroke. Follow-up interviews were conducted at home, in a rehabilitation facility or in the office of the researcher. | Thematic analysis of longitudinal, descriptive exploratory design. |
| Burton 2000 (40) (UK) | 6 | 4 women, 2 men (2 married, 2 widowed, 1 single, 1 divorced, aged 52–81 years, all eventually discharged home) recruited during inpatient rehabilitation for first-ever stroke and followed for at least 1 year period is indicated | A total of 73 informal and unstructured interviews approximately 35 min in length were conducted in private. | Content/thematic analysis based on grounded theory methodology. |
| Ellis-Hill et al. 2000 (41) (UK) | 8 | 5 men, 3 women; aged 56–82 years with spouses. Following stroke, all were admitted to hospital for more than 10 days and by 1 year, all experienced “good” physical recovery and some independence in basic ADLs. | Life narrative interviews lasting 1–2 h conducted while in hospital, at 6 months and 12 months following stroke. Initial interviews were conducted in a quiet room in the hospital. Interviews at 6 and 12 months were conducted in the participants’ homes. | Thematic analysis. |
| Dowswell et al. 2000 (42) (UK) | 30 | 30 stroke survivors and 15 carers were purposively sampled from participants in a randomized controlled trial. | Semi-structured interviews conducted in the homes of participants. Stroke survivors and carers were interviewed separately. | Thematic analysis. |
| O’Connell et al. 2001 (8) (Australia) | 40 | 37 stroke survivors and carers (+ 3 key informants), aged 20–89 years, 2–180 months post-stroke. | Semi-structured, focus group interviews lasting 60–90 min. Setting for the focus groups was not reported. | Content analysis. |
| Murray & Harrison 2004 (43) (UK) | 10 | 4 men, 6 women; aged 38–81 years, 6 divorced, 2 widowed, 1 married and 1 single, 4–20 years post-stroke. All experienced continuing deficits. | 5 face-to-face semi-structured interviews and 5 e-mail interviews. Interviews lasted approximately 50–90 min. E-mail exchanges continued for an average of 6 weeks. E-mails were received either at home or at work. Setting of face-to-face interviews was not reported. | Thematic analysis using the “Interpretive Phenomenological Analysis” method. |
| ADLs: activities of daily living. |
| Table II. Results of quality assessment |
| Study | Credibility | Relevance |
| Data collection | Auditability | Reflexivity | Negative cases | Fair dealing | Transferability | Analytic generalization |
| Becker, 1993 (36) | × | × | | × | × | × | × |
| Haggstrom et al., 1994 (37) | × | × | × | | | × | × |
| Secrest & Thomas, 1999 (38) | × | × | × | | | × | × |
| Pilkington, 1999 (39) | × | × | | | | | × |
| Burton, 2000 (40) | × | × | × | | | | × |
| Ellis-Hill et al., 2000 (41) | × | × | × | × | | × | × |
| Dowswell et al., 2000 (42) | × | × | | × | × | | × |
| O’Connell et al., 2001 (8) | × | × | | | × | | × |
| Murray & Harrison, 2004 (43) | × | × | × | × | | × | × |
All studies included in the present synthesis provided descriptions of data collection and analysis, presented findings clearly based on the data collected, and discussed those findings within a broader context, making suggestions for application and/or further research. Less well represented were features such as reflexivity, reporting of negative cases, fair dealing and transferability.
Synthesis of identified themes
On review of the compiled lists of themes, concepts and interpretations, it became apparent that participants in different studies had voiced many of the same experiences. From independent and interactive readings of the data, 5 major themes were identified; (i) Change, transition and transformation, (ii) Loss, (iii) Uncertainty, (iv) Social Isolation and (v) Adaptation and Reconciliation. These are presented in Table II, along with examples of data from the primary studies that support each theme.
Further readings revealed that the concept of transformation (theme (i)) was dominant and could be conceived as a continuous backdrop present in all other themes. None of the themes could be considered as entirely separate and distinct. Rather, they appeared to interact against an ever-present background of change and transformation.
| Table III. Process of thematic analysis |
| Identified theme | Examples of supporting data from primary studies |
| Change, transition and transformation | “Feelings of sudden and overwhelming catastrophe”(40); “sudden incident for which they were not prepared and which changed life irrevocably” (8); “entering a new foreign world” (41); “almost every patient reported how stroke had radically changed their lives” (42); “every participant expressed intense suffering amidst the sudden, devastating changes that accompanied the stroke” (39); “stroke brought about changes in all participants” (38); “all informants viewed stroke as a profound disruption to their lives, destroying the fabric of predictable everyday life” (36). “Roles and responsibilities were threatened” (37); “re-adjustment & appraisal of social role, usually in comparison to life before stroke, rarely a positive step” (37); “ongoing process of re-interpretation” (37); “major changes due to loss of work, financial difficulties, loss of friends, workmates, leisure activities and social activities” (4). “Stroke mediates all new problems and situations for the individual – ever-present, always”(37); “disruption in the continuity of participant’s experience of self was seen in all the interviews” (35); “sense of discontinuity with the person’s sense of self” (35). |
| Loss | “Loss of control (over bodies and individual circumstances)” (37); “in describing what life was like now, participants spoke at length about restrictions and losses of taken-for-granted freedoms, abilities and ways of relating” (36); “struggling with the loss of their independence and abilities” (35); “loss of confidence and a psychologically-imposed loss of physical control” (40); “erosion of independence” (4); “loss of confidence in the body in general” (38); “loss of self” (43). “Feelings of helplessness and frustration were frequently expressed in relation to enforced changes of role”(39); “feelings of dependence provoked negative reactions” (37); “an emotional reaction to loss is woven through several transcripts” (35); “suffering emerges amid unaccustomed restrictions and losses” (36). |
| Uncertainty | “Sense of worsening leading to fear and disappointment” (37); “inability to understand what happened…to be unable to identify a cause led to loss in confidence in the body in general and a long-lasting fear of recurrence” (38); uncertainty (identity), confusion (about what has happened) and worries (about the future)” (34); “future became painfully and consciously uncertain” (33); “restrictions and losses also surfaced in participants’ concerns and worries about the future” (36) ; “bodies became something perplexing and unreliable and they tried to understand what had been happening to them and how to get their bodies under their control again” (38); “body was the locus of uncertainty” (33). |
| Social isolation | “All informants reported feeling at some time as though they were isolated or stuck in a cage”(37); “increased social isolation” (33); “most social interactions and the physical activities that accompanied them were curtailed by the limitations created by the stroke (33); “relative to the pre-stroke period, there had been clear deterioration in the social lives of the majority of the respondents”(39); “social interaction of participants had diminished following their stroke, and their friendships in particular had deteriorated as they became socially withdrawn” (40); “close friends and workmates stopped phoning and visiting as they found it uncomfortable communicating with the stroke survivor” (4); “break with others…enhances discontinuity of self”, “experience can be particularly painful” (35); “stroke damaged existing relationships” “made it difficult for new relationships to form” (40). |
| Adaptation and reconciliation | “Some informants were able to focus on positive aspects of their lives over which they felt they had control” (37); “as if to balance the loss of control, participants spoke of experience in which they were in control. These included mastering new skills, adapting old skills and changing their environment” (35); “appreciation of the ordinary shifts perspectives” (36); “patients focused on tiny, incremental gains in an effort to create continuity…once it was possible to do those things, they were filled with hope” (33); “for some, appreciation that progress was made was tempered by dissatisfaction with the rate of progress or lack of further progress”(39); “optimism (with rehabilitation) diminished as they realized the slow process of recovery or their lack of progress” (4); “at 1 year, the majority of respondents were still working to get a sort of negotiated settlement – a realignment between body, self and society” (38). |
Change, transition and transformation. Ideas of change and transformation were expressed in all of the studies included in this synthesis. Stroke was characterized as a sudden and overwhelming catastrophe (8, 36, 39, 40), a fundamental life change (41) and profound disruption (42); one which separated survivors from their everyday life and forced them into a new and foreign existence (36, 40, 41). Stroke “changed life irrevocably” (8), and had a significant impact on emotions (8, 43), personality (42), abilities (36, 41), activities (8), roles and social relationships (8, 40). Stroke was seen as something that was always present, mediating experiences (36, 40), creating effort where there had been none and disrupting the survivors’ sense of self (38, 41, 43).
The concept of an ongoing process of re-interpretation of the self, or of being transformed by stroke, was expressed in the themes and supporting interpretations of the majority of studies. Stroke, and the changes and losses experienced as a result of stroke, challenged the participants’ sense of self and precipitated a sense of discontinuity or estrangement from the person they had been prior to stroke (38, 43). Participants questioned whether they were the same person at all and struggled to confront perceived changes in an attempt to reconcile their present selves with their pre-stroke selves (36, 38). For some, this was based primarily on comparisons with their pre-stroke selves and a desire to get back to who they were before the stroke event. For example, changes over time were “grudgingly acknowledged and some patients were self-critical of progress made”; they expressed dissatisfaction and frustration with both themselves and their recovery, which they “measured in terms of self prior to stroke”(42). For others, it was a process of transformation; of negotiating a new identity that included their changed abilities (36, 43).
Loss. The ideas of loss were described through a variety of experiences and appeared to be linked to the overwhelming changes associated with stroke. Participants across studies spoke of loss of control, confidence and independence. For instance, in one study, the authors suggested that the “world of a person who has a stroke is grounded in loss and effort” and they struggle “with the loss of their independence and abilities” and “for many, their previously unreflected-on, taken-for-granted way of being in the world has now become a conscious effort” (38). Similarly, other participants’ stories reflect “restrictions and losses of taken-for-granted freedoms, abilities and way of relating” (39). Going home “reinforced a sense of loss” and “did not measure up to their own criteria for normality” (36). The disruption in the continuity of perceived self was also noted as a loss of self, or of “pre-stroke me” (40) as well as in a loss of identity associated with the “enforced change in roles” (42).
Losses were often described in a climate of unpleasant feelings (37–39). Pilkington (39) proposed a theme entitled “suffering emerges amid unaccustomed restrictions and losses”, while others reported participants’ descriptions of sadness and mourning (37). In addition, helplessness, anger and frustration were described in response to losses of control and independence (40, 42). “Many felt resigned to a passive role” (40).
Uncertainty. Given the “initial overwhelming nature of stroke” (40), participants across 7 of the synthesized studies described feelings of anxiety or uncertainty about what the future might hold for them and some expressed fears of another stroke (39, 41). Becker (36) reported that the “future became painfully uncertain” and the body was “the locus of uncertainty”. Early feelings of progress were interrupted by periods of slowed or halted recovery (8, 40), some wondered if they would ever “get back to normal” (39). The physical body became unreliable and unpredictable, a source of disappointment (38, 41).
Social isolation. The importance of relationships, social connections and participation was evident. Relationships supported, comforted and consoled individuals following stroke. For example, Pilkington (39) noted that “loving supportive relationships brought them (individuals with stroke) comfort and encouragement”. Having connections with others helped “bridge the schism in the discontinuity of their lives” and “meant reciprocity, being with and understood by someone and experiencing help from others”, while disconnection “enhances the discontinuity of self” and was “particularly painful” (41).
Unfortunately, the majority of participants across studies appeared to experience feelings of increasing social isolation, social withdrawal and/or altered relationships with both families and friends. Participants felt distanced from other people in that it was “difficult to explain their experiences to others” who found it impossible to “imagine what it must be like to live following a stroke” (41) and found communication with the stroke survivor to be too uncomfortable (8). This separation from others seemed to promote a climate in which the stroke survivors felt as though they were misunderstood or even treated rudely or dismissively because of their disabilities, both visible and invisible (8, 41, 43). Some participants expressed discomfort with their current selves, in terms of both physical ability and appearance (36, 41, 42), and became more withdrawn in order to avoid becoming a burden to family, friends and acquaintances (42).
Adaptation and reconciliation. From the backdrop of change and transformation, the ideas of resiliency and adaptation emerged. As time passed from the stroke event, some informants began to focus on more positive aspects of their lives over which they had regained a sense of control (38–40, 42). For example, some participants “spoke of experiences in which they were in control…these included mastering new skills, adapting old skills and changing their environment” (38). For some, this process of re-focusing and adaptation was associated with feelings of hope for recovery (36, 37, 39).
Although it may seem to be an end-point of transformation, adaptation itself is not static. Rather, it may be viewed as a difficult process of reconciliation between the past and present selves. Recovery was often described in terms that referenced the pre-stroke self and abilities of the individual. For instance, informants spoke of “getting back to normal” or “continuing as before” (39). Initial optimism regarding progress toward these goals tended to diminish over time, particularly as recovery slowed or stalled (8, 40, 42). Dowswell et al. (42) suggested that there “appeared to be no fully successful adjustment to stroke” and that the process of adjustment was “bedevilled by constant reference back to life before stroke – not to milestones in recovery”. However, the idea of re-definition and reconciliation in order to create a continuous or coherent sense of self also emerged from the themes and interpretations within the studies. For example, Becker (36) noted that “all respondents searched for anchors of predictability and sought to define and build links between the old self and new imperatives”. Participants in the study by Ellis-Hill et al. (41) were described as “working to get a sort of negotiated settlement – a realignment between body, self and society and create a coherent sense of self”, while Dowswell et al. (42) noted that “a small number of patients had arrived at a sort of truce with themselves”.
Discussion
Suffering a stroke challenges the assumptive identity, self-concept and role-capacity of the individual in the face of acquired deficits. Individuals with stroke are required to adjust to these challenges while adapting to functional disabilities. According to Glass & Maddox (44), the stroke experience can be viewed as a psychological transition, in that (i) it takes place in a short period of time and often strikes without warning; (ii) it alters the capacity for social role functioning; and (iii) the risk of loss of functional independence requires adjustment to a new definition of self. This perspective appears to be well supported by the themes identified from the qualitative research included in the present synthesis.
When the stroke experience is viewed in terms of a psychosocial transition, the role of social support in stroke rehabilitation gains importance. Results from quantitative studies indicate that the perceived effectiveness of social support networks have a positive influence on both physical recovery and quality of life post-stroke (45). However, the predominant theme identified here is one of social isolation or disconnection from others. Although relationships are perceived to be important, not only for comfort and support, but also for maintaining a sense of continuity, the majority of studies described loss of roles and relationships, decreased social interaction and increasing isolation (8, 36–38, 40–43).
While many of the participants in the qualitative studies included here spoke of change and loss, study data also reflected a shift toward adaptation and recovery for some informants. Doolittle (22) suggested that recovery from stroke is marked by what matters to the individual, and that this is to return to a life that is meaningful. Folden (23) undertook a qualitative study to examine the process of managing recovery from stroke. In that study, individuals who had gone through a period of transformation and adaptation that included identifying as a stroke survivor proceeded toward recovery. Forward progress was maintained through hope, preserving energy and increasing a sense of control over recovery, where recovery was defined in terms of the individual’s personal goals and values, not by the goals of the stroke rehabilitation team (23). In a study focusing on a comparison of the perceptions of patients with those of healthcare professionals regarding the implications of stroke, Bendz (27) reported that healthcare professionals tended to set very different sorts of goals from patients. Healthcare professionals focused on physical tasks or functional ability with concrete end-points. Patients, on the other hand, reported less concrete goals pertaining to personal identity, finding new roles or defining a new sense of normal. For them, the processes of adaptation and reconciliation, including the development of new ways to interact with the social world, may be the focus for recovery, rather than physical or functional ability alone (40).
Delivery of stroke services based on an understanding of the experiences of individuals with stroke shifts the focus from the service provider to the intervention recipient (38), whereas, approaches that are based solely on clinical interpretations of the recovery process may be of little relevance to the individual (27, 40, 46). Discrepancies between the goals of involved healthcare professionals and the subjective needs and desires of patients, particularly in areas such as interpersonal relationships, roles, mobility and leisure, may result in isolation and development of secondary handicaps (46, 47). Adaptation of rehabilitation practices to reflect the needs and concerns of the individual and reduce these discrepancies may require an investment in patient-centred practice that includes taking the time to discover the personal narratives and stories of patients and initiating regular discussions around individual preferences and concerns. For the individual with stroke, this approach may foster a greater sense of personal control in the recovery process, thereby increasing motivation and maintaining a sense of progress through the process of transformation and adaptation (23). For members of the interdisciplinary healthcare team, better knowledge of the patient’s life context and needs may assist in designing meaningful and effective rehabilitation strategies, improved co-ordination of appropriate services and recognition of existing service gaps (46–48).
Study limitations
At present, the process of qualitative meta-synthesis is not well defined. The role of quality assessment of studies to be included remains controversial. We chose to maintain broad inclusion criteria in order to prevent the exclusion of potentially valuable data, and provide additional information regarding the quality of those studies included in the synthesis process. In addition, although individuals who share the experiences in question may best assess the credibility of interpretations (19), we were unable to conduct a peer-review of the analysis as presented. It is also important to note that participants included in the synthesis studies were able to respond to open-ended questions in an interview setting and therefore, may represent a group of individuals with no significant cognitive or language impairments post-stroke.
In conclusion, meta-synthesis of qualitative research is needed to promote the inclusion of what we know about patient preferences and values in evidence-based practice (9, 49). At present, service provision is based on the “expert” medical interpretations of recovery; however, this may not be of relevance to the stroke survivor. Provision of services should reflect a more comprehensive understanding of the experience of living with stroke. Qualitative findings may be used in conjunction with quantitative research in the development of patient-centred, tailored interventions that are effective, feasible and meaningful.
The present analysis suggests that stroke represents a sudden, overwhelming and fundamental change for the survivor. Transition and transformation form a background for loss, uncertainty and social isolation. However, stroke survivors may move forward through adaptation and reconciliation of identity towards meaningful recovery. Rehabilitation professionals should actively cultivate an awareness of patient experiences, priorities and goals. This awareness could promote effective strategies for care focused on what is most relevant to the individual.
REFERENCES
1. Hafsteinsdottir TB, Grypdonck M. Being a stroke patient: a review of the literature. J Adv Nurs 1997; 26: 580–588.
2. Pound P, Gompertz P, Ebrahim S. A patient-centered study of the consequences of stroke. Clin Rehabil 1998; 12: 338–347.
3. Salter KL, Foley NC, Jutai JW, Teasell RW. Assessment of participation outcomes in randomized controlled trials of stroke rehabilitation interventions. Int J Rehabil Res 2007; 30: 339–342.
4. Bayley KB, London MR, Grunkemeier GL, Lansky DJ. Measuring the success of treatment in patient terms. Med Care 1995; 33 Suppl 4: AS226–AS235.
5. Clarke P. Towards a greater understanding of the experience of stroke: integrating quantiative and qualitative methods. J Aging Studies 2003; 17: 171–187.
6. Fuhrer MJ. Subjectifying quality of life as a medical rehabilitation outcome. Disabil Rehabil 2000; 22: 481–489.
7. McKevitt C, Redfern J, Mold F, Wolfe C. Qualitative studies of stroke. A systematic review. Stroke 2004; 35: 1499–1505.
8. O’Connell B, Hanna B, Penney W, Pearce J, Owen M, Warelow P. Recovery after stroke: a qualitative perspective. J Qual Clin Pract 2001; 21: 120–125.
9. Sandelowski M. Using qualitative research. Qual Health Res 2004; 14: 1366–1386.
10. Noblit GW, Hare RD, editors. Meta-ethnography: synthesizing qualitative studies. Newbury Park, CA: Sage Publications; 1988.
11. Jensen LA, Allen MN. Meta-synthesis of qualitative findings. Qual Health Res 1996; 6: 553–560.
12. Campbell R, Pound P, Pope C, Britten N, Pill R, Morgan M, et al. Evaluating meta-ethnography: a synthesis of qualitative research on lay experiences of diabetes and diabetes care. Soc Sci Med 2003; 56: 671–684.
13. Bondas T, Hall EO. Challenges in approaching metasynthesis research. Qual Health Res 2007; 17: 113–121.
14. Finfgeld DL. Metasynthesis: the state of the art – so far. Qual Health Res 2003; 13: 893–904.
15. Hammell KW. Quality of life after spinal cord injury: a meta-synthesis of qualitative findings. Spinal Cord 2007; 45: 124–139.
16. Reis S, Hermoni D, Van Raalte R, Dahan R, Borkan JM. Aggregation of qualitative studies – from theory to practice: patient priorities and family medicine/general practice evaluations. Patient Educ Couns 2007; 65: 214–222.
17. Sandelowski M, Docherty S, Emden C. Focus on qualitative methods. Qualitative metasynthesis: issues and techniques. Res Nurs Health 1997; 20: 365–371.
18. Letts L, Wilkins S, Law M, Stewart D, Bosch J, Westmorland M. Guidelines for critical review form: qualitative studies (version 2.0). Available from: http://www.fhs.mcmaster.ca/rehab/ebp/. 2007
19. Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P. Qualitative research methods in health technology assessment: a review of the literature. Health Technol Assess 1998; 2: 1–274.
20. Sandelowski M, Barroso J. Classifying the findings in qualitative studies. Qual Health Res 2003; 13: 905–923.
21. Mays N, Pope C. Qualitative research in health care. Assessing quality in qualitative research. BMJ 2000; 320: 50–52.
22. Doolittle ND. Clinical ethnography of lacunar stroke: implications for acute care. J Neurosci Nurs 1991; 23: 235–240.
23. Folden SL. Managing the effects of a stroke: the first months. Rehabil Nursing Res 1994; Fall: 79–85.
24. Nilsson I, Jansson L, Norberg A. To meet with a stroke: patients’ experiences and aspects seen through a screen of crises. J Adv Nurs 1997; 25: 953–963.
25. Wyller TB, Kirkevold M. How does a cerebral stroke affect quality of life? Towards a theoretical account. Disabil Rehabil 2003; 21: 152–161.
26. Eaves YD. ”What happened to me”: rural African American elders’ experiences of stroke. J Neurosci Nurs 2000; 32: 37–48.
27. Bendz M. The first year of rehabilitation after a stroke – from two perspectives. Scand J Caring Sci 2003; 17: 215–222.
28. Gillen G. Positive consequences of surviving a stroke. Am J Occup Ther 2005; 59: 346–350.
29. Clarke P, Black SE. Quality of life following stroke: negotiating disability, identity and resources. J Appl Gerontol 2005; 24: 319–336.
30. Tariah HA, Hersch G, Oswald SK. Factors associated with quality of life: perspectives of stroke survivors. Phys Occup Ther Geriatr 2006; 25: 33–50.
31. Hartke RJ, King RB, Denby F. The use of writing groups to facilitate adaptation after stroke. Top Stroke Rehabil 2007; 14: 26–37.
32. Mumma CM. Perceived losses following stroke. Rehabil Nurs 1986; 11: 19–24.
33. Clark MS. Patient and spouse perceptions of stroke and its rehabilitation. Int J Rehabil Res 2000; 23: 19–29.
34. Hilton EL. The meaning of stroke in elderly women: a phenomenological investigation. J Gerontol Nurs 2002; 28: 19–26.
35. Rochette A, Tribble DS, Desrosiers J, Bravo G, Bourget A. Adaptation and coping following a first stroke: a qualitative analysis of a phenomenological orientation. Int J Rehabil Res 2006; 29: 247–249.
36. Becker G. Continuity after a stroke: implications of life-course disruption in old age. Gerontologist 1993; 33: 148–158.
37. Häggström T, Axelsson K, Norberg A. The experience of living with stroke sequelae illuminated by means of stories and metaphors. Qual Health Res 1994; 4: 321–337.
38. Secrest JA, Thomas SP. Continuity and discontinuity: the quality of life following stroke. Rehabil Nurs 1999; 24: 240–246.
39. Pilkington B. A qualitative study of life after stroke. J Neurosci Nurs 1999; 31: 336–347.
40. Burton CR. Living with stroke: a phenomenological study. J Adv Nurs 2000; 32: 301–309.
41. Ellis-Hill CS, Payne S, Ward C. Self-body split: issues of identity in physical recovery following a stroke. Disabil Rehabil 2000; 22: 725–733.
42. Dowswell G, Lawler J, Dowswell T, Young J, Forster A, Hearn J. Investigating recovery from stroke: a qualitative study. J Clin Nurs 2000; 9: 507–515.
43. Murray CD, Harrison B. The meaning and experience of being a stroke survivor: an interpretative phenomenological analysis. Disabil Rehabil 2004; 26: 808–816.
44. Glass TA, Maddox GL. The quality and quantity of social support: stroke recovery as psycho-social transition. Soc Sci Med 1992; 34: 1249–1261.
45. Teasell R, Foley N, Salter K, Bhogal SK, Jutai J, Speechley M. Evidence-based review of stroke rehabilitation. 10th web edn. London: Ontario; 2007, September 5. Available from: www.ebrsr.com
46. Liu KP, Chan CC, Chan F. Would discussion on patients’ needs add value to the rehabilitation process? Int J Rehabil Res 2005; 28: 1–7.
47. Vincent C, Deaudelin I, Robichaud L, Rousseau J, Viscogliosi C, Talbot LR, et al. Rehabilitation needs for older adults with stroke living at home: perceptions of four populations. BMC Geriatr 2007; 7: 20.
48. Blickem C, Priyadharshini E. Patient narratives: the potential for «patient-centred» interprofessional learning? J Interprof Care 2007; 21: 619–632.
49. McCormick J, Rodney P, Varcoe C. Reinterpretations across studies: an approach to meta-analysis. Qual Health Res 2003; 13: 933–944.