OBJECTIVE: The aim of this study was to assess the effectiveness of neuromuscular electrical stimulation in patients with dysphagia caused by stroke.
METHODS: Thirty-six subjects were randomized into experimental and control groups. The control group was given thermal-tactile stimulation treatment only, while in the experimental group neuromuscular electrical stimulation and thermal-tactile stimulation treatments were applied simultaneously. Swallowing function was assessed before and 4 weeks after treatment, and evaluated via the swallow function scoring system, penetration-aspiration scale, and pharyngeal transit time. In addition, the discomfort score during the treatments and the satisfaction score 4 weeks after the treatments were measured.
RESULTS: Twenty-eight persons with dysphagia completed the study, 16 in the experimental group and 12 in the control group. Both groups showed improvement, but the experimental group showed more significant improvement in the swallow function scoring system, penetration-aspiration scale and pharyngeal transit time than the control group. The patient’s discomfort score did not show statistically significant differences in either group, but the satisfactory score was higher in the experimental group.
CONCLUSION: The results suggest that neuromuscular electrical stimulation combined with thermal-tactile stimulation is a better treatment for patients with swallowing disorders after stroke than thermal-tactile stimulation alone.
Key words: swallowing, dysphagia, stroke, neuromuscular electrical stimulation.
J Rehabil Med 2009; 41: 174–178
Correspondence address: Kil-Byung Lim, Department of Rehabilitation Medicine, College of Medicine, Ilsan Paik Hospital, Inje University, 2240 Daehwa-dong, Ilsanseo-gu, 411-706 Goyang, Korea. E-mail: kblim@paik.ac.kr
Submitted April 2, 2008; accepted October 8, 2008
INTRODUCTION
Swallowing is initiated by the cerebral cortex and effected by the brainstem swallowing centre (1). Although not all brain injuries affect areas involved in steering the swallowing process, many brain injuries, such as from a stroke, disrupt the normal physiology of swallowing, leaving the airway vulnerable to the entry of food into the lungs (aspiration) (2). Dysphagia occurs in 45–65% of patients after acute stroke (3), it is the most significant risk factor for the development of pneumonia and can delay the patient’s functional recovery (4). Pneumonia accounts for approximately 34% of all stroke-related deaths and is the third-highest cause of death during the first month after stroke, although not all these pneumonias are caused by aspiration of food following attempted eating (4, 5). Therefore, detecting and managing dysphagia as early as possible is critical among patients after stroke.
Oropharyngeal motor dysfunction is an important cause of swallowing disorder after stroke (6). In addition, it has been claimed that pharyngeal sensory impairment is common after acute stroke and that such impairment is associated with an increased risk of aspiration and aspiration pneumonia (7). Recovery from dysphagia secondary to stroke is not guaranteed. As a result, a variety of treatments have been developed for improving stroke patient’s ability to swallow safely, and perhaps even sufficiently to allow a return to completely normal eating and drinking. A common method in clinical practice is thermal-tactile stimulation (TTS), which involves stroking or rubbing the anterior faucial pillars with a cold probe prior to having the patient swallow. It is hypothesized that the touch and cold stimulation increases “oral awareness” and provides “an alerting sensory stimulus to the cortex and brainstem, such that, when the patient initiates the oral stage of swallow, the pharyngeal swallow will trigger more rapidly” (8).
Electrical stimulation has been reported as a treatment for pharyngeal dysphagia in a few recent studies. Neuromuscular electrical stimulation (NMES) uses surface electrodes to deliver electrical stimulation to muscles causing muscle contractions by depolarization of nerve fibres within the region of application. Freed et al. (9) compared the effectiveness of NMES therapy with that of TTS therapy. Both groups made improvements in swallow function, but those in the NMES group reported greater and longer-lasting benefits. Leelamanit et al. (10) used NMES to stimulate the thyrohyoid muscle, with the goal of improving laryngeal elevation in 23 patients with reduced laryngeal elevation dysphagia, and patients showed improvement in the swallowing function after NMES therapy. However, Power et al. (11) assessed the effects of oral stimulation at the faucial pillar on measures of swallowing and aspiration in patients after stroke with dysphagia and reported no evidence for functional change in swallowing physiology after faucial pillar stimulation. As mentioned above, the efficacy of NMES in treating dysphagia is currently under debate. The aim of this study was to assess NMES stimulation in patients with dysphagia caused by stroke.
METHODS
Subjects
Thirty-six patients with a diagnosis of dysphagia after stroke, who were admitted to Ilsan Paik Hospital from February 2005 to July 2006 and who consented to participate, were enrolled in the study. Participant selection criteria included primary diagnosis of stroke with magnetic resonance imaging (MRI) or computerized tomography (CT) scans, confirmation of swallowing disorder by videofluoroscopy, a score of 21 or greater on the Mini-Mental State Examination (MMSE), and that they were medically stable at the time of the study.
Exclusion criteria included the inability to receive the treatment for 1 h, a neurological disease other than stroke, a combined behavioural disorder that interfered with administration of therapy, current illness or upper gastrointestinal disease, and an inability to give informed consent because of cognitive impairment or receptive aphasia. The subjects gave their informed consent to participation before starting the study.
Procedures
Subjects were divided into 2 groups according to the order of enrolment in the study following admission to the rehabilitation department. The subjects in the experimental group were given NMES and TTS treatment simultaneously, while those in the control group were treated with TTS alone.
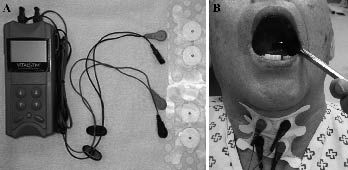
Electrical stimulation treatment. Electrical stimulation was applied by an occupational therapist, using a modified hand-held battery-powered electrical stimulator (VitalStim® Dual Channel Unit and electrodes, Chattanooga Group, Hixson, TN, USA). The skin of the anterior neck was prepared with 70% isopropyl alcohol cotton. Two sets of electrodes were used. The top set was placed in the submental region between the anterior belly of the digastric muscle and hyoid bone, and the hyoid bone and thyroid cartilage. The bottom set was placed on the skin between the thyroid cartilage and cricoid cartilage and below the cricoid cartilage (Fig. 1). Through this method, we could stimulate the muscles needed for swallowing, such as the digastric muscle, myohyoid muscle, and thyrohyoid muscle.
Fig. 1. (A) The VitalStim® equipment. (B) Both VitalStim® and thermal-tactile stimulation are applied to the stroke-related dysphagia patient.
NMES carries possible risks, including laryngospasm, arrhythmia, hypotension, glottic closure, and burns. We explained the possible adverse effects to the patients before treatment, and we closely observed and recorded every treatment session.
After familiarizing the participant with the device, we identified the sensory threshold as the lowest current level at which the participant reported a “tingling” sensation on the skin. The amplitude of the electrical current level was approximately 7 mA. The therapy sessions were for 1 h at a frequency of 5 per week. The VitalStim® device cycles automatically from “on” to “off” to “on” again for 1 sec every min. Because the change in stimulation is ramped, this cycling process takes up to 4 sec.
Thermal-tactile stimulation treatment. The TTS procedures were standardized and conducted by a co-operating occupational therapist (12). An occupational therapist used the standard method for TTS. A cold mirror (size 00) was used to stimulate the oral cavity and an ice stick was used to stimulate the side of the face. Rubbing was carried out firmly, but not so as to cause discomfort. The rubbing extended from as low on the faucial pillar as it was possible to reach, and as high as possible, with no effort made to avoid the tongue. Subjects were asked periodically if they could feel the cold and if it was uncomfortable. They were also instructed to report discomfort as soon as it occurred. Five trials were carried out per week. Therapy sessions for electrical stimulation treatment were the same.
Assessment. Each patient’s swallowing was assessed using 3 systems; the swallow function scoring system (9), Rosenbek penetration-aspiration scale (13), and pharyngeal transit time by videofluoroscopic imaging, at baseline and after the 4 weeks of treatment.
Discomfort during the treatments was measured using the discomfort score, which was assessed like pain scoring using a visual analogue scale. In addition, we measured the subjective satisfaction of the patients after the 4-week treatment session using the satisfactory score, which was assessed with 10-point scales from 1 to 10 point. A higher score indicates greater satisfaction. The tube-feeding ratio in the 2 groups was assessed before and after this study.
The swallow function scoring system was previously developed and validated as a 7-point scale that describes the severity of swallowing function (Appendix I). The penetration-aspiration scale is an 8-point scale that measures selected aspects of penetration and aspiration, conveying depth of airway invasion and whether material entering the airway is expelled (Appendix II). Standardized videofluoroscopic swallowing examinations using 10 ml semi-solid and liquid boluses were taken. Pharyngeal transit time (PTT) was defined as the interval (in sec) between the first frame showing the arrival of the bolus head at the trigger point and the last frame showing the tail of the bolus passing through the upper oesophageal sphincter, although the trigger point differs according to the type of bolus or age of the subject. To preserve patient safety, testing was discontinued if a subject aspirated a large amount of boluses without successfully clearing them from the airway.
A well-trained physiatrist was blinded during this study period by the way of not being informed about this study and grouping of the patients. He performed the videofluoroscopic examination and measured the PTT as well as the swallow function scoring system and Rosenbek penetration-aspiration scale.
Data analysis
The Mann-Whitney U test was used to compare variables between experimental and control groups and the Wilcoxon signed-rank test was used to compare variables before and after treatment in the same group. Analyses were performed using SPSS 10.0 version software and statistical significance was set at p < 0.05.
RESULTS
Subjects
Thirty-six patients with post-stroke dysphagia were enrolled in this study over the 2-year study period, but only 28 patients completed the study (16 in the experimental group and 12 in the control group). The main cause of not completing the study was early transfer to other hospital.
The mean age of the experimental group was 67.8 years, with 14 men and 2 women. The mean age of the control group was 60.8 years, with 10 men and 2 women. The experimental group was thus older than the control group; however, gender distribution, affected hemisphere, stroke type, location of lesion, months to study from onset, and previous treatment history of aspiration pneumonia were similar in the 2 groups (Table I).
| Table I. General characteristics of the subjects |
| Characteristics | Experimental group (n = 16) | Control group (n = 12) |
| Age, years, mean (SD) | 67.8 (8.1) | 60.8 (12.3) |
| Gender, men/women, n | 14/2 | 10/2 |
| Aetiology, n |
| Cerebral infarction | 10 | 8 |
| Cerebral haemorrhage | 6 | 3 |
| Subarachnoid haemorrhage | 0 | 1 |
| Location of lesion, n |
| Basal ganglia or thalamus | 12 | 8 |
| MCA territories | 2 | 2 |
| Brainstem | 2 | 2 |
| Side of lesion, n |
| Right | 8 | 6 |
| Left | 7 | 5 |
| Both | 1 | 1 |
| Months from onset, n |
| < 6 months | 13 | 9 |
| > 6 months | 3 | 3 |
| Previous treatment history of aspiration pneumonia, present/absent | 10/6 | 9/3 |
| SD: standard deviation; MCA: middle cerebral artery. |
During both treatments, the patient’s discomfort score did not show any statistically significant difference. However, the satisfactory score was significantly higher in the experimental group (Table II).
Swallowing measures
In the assessment of swallow function scores, there was no difference between the 2 groups at initial evaluation. After each treatment was applied, the median values of swallow function score changed significantly; from 2 to 4, in the experimental group (p < 0.05), and from 3 to 4 in the control group (not significant). Regarding the difference between the initial and final swallow function score, patients in the experimental group had significantly higher score changes than those in the control group (Table II).
| Table II. Median discomfort scores, satisfactory scores and swallow function scores on treatment |
| | Experimental group | Control group |
| Discomfort and satisfactory scores |
| Discomfort scores | 2 | 1 |
| Satisfactory scores | 7* | 3 |
| Swallow scores |
| Initial swallow scores | 2 | 3 |
| Final swallow scores | 4† | 4 |
| Difference in scores after the treatment | 2* | 0 |
| †p < 0.05 by Wilcoxon signed-rank test between initial and final scores in the same group. *p < 0.05 by Mann-Whitney U test between experimental and control groups. |
The penetration-aspiration scale improved significantly in the experimental group after treatment; from 5.5 to 2.5 in the test for semi-solids (p < 0.05), and from 7 to 5 for liquids (p < 0.05). In the control group a slight improvement was shown in both test materials, but not to any significant degree. Regarding the difference between the initial and final penetration-aspiration scales, patients in the experimental group had significantly higher scores; 2 in semi-solid (p < 0.05) and 2.5 in liquid (p < 0.05) than those in the control group (Table III).
| Table III. Penetration-aspiration scale (PAS) scores before and after the treatment given as median values |
| | Experimental group | Control group |
| Semi-solid | Liquid | Semi-solid | Liquid |
| Initial PAS scores | 5.5 | 7 | 3.5 | 7 |
| Final PAS scores | 2.5† | 5*† | 4 | 6.5 |
| Difference after the treatment | 2* | 2.5* | 0 | 0 |
| †p < 0.05 by Wilcoxon signed-rank test between initial score and the final in the same group. *p < 0.05 by Mann-Whitney U test between the experimental and control groups. |
The overall PTT was significantly lower; 0.86 sec in semi-solid (p < 0.05) and 0.86 sec in liquid (p < 0.05), and the change in time was significantly greater after treatment in the experimental group; 0.11 in semi-solid (p < 0.05) and 0.10 than in the control group (p < 0.05) (Table IV).
| Table IV. Mean pharyngeal transit time (PTT) before and after treatment given as mean with standard deviation |
| | Experimental group | Control group |
| Semi-solid | Liquid | Semi-solid | Liquid |
| Initial PTT | 0.97 (0.18) | 0.96 (0.19) | 0.97 (0.19) | 0.99 (0.23) |
| Final PTT | 0.86 (0.18)† | 0.86 (0.19)† | 0.96 (0.19) | 0.97 (0.22)† |
| Difference after the treatment | 0.11* | 0.10* | 0.01 | 0.02 |
| †p < 0.05 by Wilcoxon signed-rank test between initial and final in the same group. *p < 0.05 by Mann-Whitney U test between experimental and control groups. |
The tube-feeding cases were 12 out of 16 patients in the experimental group, 7 out of 12 patients in the control group before the experiment. There were 6 patients who progressed to oral feeding out of the 12 tube-fed patients in the experimental group, while only one of the 7 tube-fed patients in the control group did so.
NMES carries possible risks, including laryngospasm, arrhythmia, hypotension, glottic closure, and burns. However, no adverse effects were observed during the study period using NMES.
DISCUSSION
The aim of this study was to assess the NMES treatment and compare this with TTS treatment alone. The use of electrical stimulation in treating dysphagia was first reported by Park et al. (14). They used oral electrical stimulation to enhance the afferent arm of the swallow reflex in patients after stroke with dysphagia associated with delayed initiation of swallowing. On the other hand, Freed et al. (9) used the VitalStim® method specifically to increase muscular contractile forces. However, they did not provide any experimental control and this research has been criticized accordingly. Although the method used in our study, in which electrical stimulation was used to stimulate the contraction of swallowing-associated muscles, is similar to that in the study by Freed et al. (9), our study includes experimental control. Our results show that the NMES treatment with TTS has a better effect on improving swallowing or aspiration severity than does TTS alone. In addition, the electrical stimulation showed better satisfaction than TTS, as well as no significant discomfort.
The swallowing process involves a complex pattern of sequential motor contractions modulated by afferent stimuli to the brainstem swallowing centre. In detail, the swallowing centre is located within the brainstem, and the cortex has a role in modulating the reflex on a bolus to bolus basis. In addition, swallowing is a sequential, semi-automatic contraction and relaxation of the 55 muscles of the oropharyngeal, laryngeal and oesophageal regions, 6 cranial nerves, and 2 cervical nerve roots, which are unique and specific for each individual. The swallow is primarily controlled in the brainstem, but sensory input from the mouth (faces, tonsils, soft palate, and tongue base) and pharynx (posterior pharyngeal wall) heavily moderates and modulates the swallow. Many small muscles in the head and neck participate in the oropharyngeal phase of swallowing. The motor units within each of the laryngeal muscles tend to fire asynchronously during normal swallowing. Thus, they may be highly susceptible to failure of normal firing during swallowing (15). Also, disuse of a striated muscle leads to atrophy of the muscle. Electrical stimulation may enhance tone and strength, or help activation of the muscle.
Although patients with dysphagia after a stoke can recover their swallow function spontaneously, a mean of tube-feeding was needed for 15–60 weeks, and 30% of all patients continued on total tube-feeding for one year after their stroke (16). In our study, 19 of the total of 26 patients (65%) had required tube-feeding after their stroke. However, the tube-feeding ratio was decreased to 46% after the study. On the other hand, we found that 6 out of 12 patients in the experimental group who had had tube-feeding were able to progress to oral feeding, while only one out of 7 patients in the control group was able to progress to oral feeding. These findings also showed that neuromuscular electrical stimulation combined with TTS can help the recovery of dysphagia more effectively than TTS alone.
The main limitations of this study were the relatively small numbers of subjects participating in both groups, and the short follow-up period. Further research is therefore required with a larger group of patients with dysphagia and a long-term follow-up period. In addition, the effects on swallowing physiology of changing variables of electrical stimulation, such as frequency and amplitude, have not yet been established, and these could be an interesting area for future research.
In conclusion, the results of this study suggest that NMES combined with TTS is a better treatment for patients with swallowing disorders after stroke than conventional TTS alone.
REFERENCES
1. Doty RW. Neural organization of deglutition. Handb Physiol 1968; 4: 1861–1902.
2. Mann G. Review of reports on relative prevalence of swallowing disorders after acute stroke. Dysphagia 2002; 17: 81–82.
3. Daniels SK, Brailey K, Priestly DH, Herrington LR, Weisberg LA, Foundas AL. Aspiration in patients with acute stroke. Arch Phys Med Rehabil 1998; 79: 14–19.
4. Roth EJ. Medical complications encountered in stroke rehabilitation. Phys Med Rehabil Clin North Am 1991; 2: 563–578.
5. Horner J, Massey EW. Silent aspiration following stroke. Neurology 1988; 38: 317–319.
6. Daniels SK, Brailey DH, Priestly LR, Herrington LA, Weisberg LA, Foundas AL. Aspiration in patients with acute stroke. Arch Phys Med Rehabil 1998; 79: 14–19.
7. Kidd D, Lawson J, Nesbitt R, MacMahon J. Aspiration in acute stroke: a clinical study with videofluoroscopy. Q J Med 1993; 86: 825–829.
8. Logemann JA. The dysphagia diagnostic procedure as a treatment efficacy trial. Clin Commun Disord 1993; 3: 1–10.
9. Freed ML, Freed L, Chatburn RL, Christian M. Electrical stimulation for swallowing disorders caused by stroke. Respir Care 2001; 46: 466–474.
10. Leelamanit V, Limsakul C, Geater A. Synchronized electrical stimulation in treating pharyngeal dysphagia. Laryngoscope 2002; 112: 2204–2210.
11. Power ML, Fraser CH, Hobson A, Singh S, Tyrrell P, Nicholson DA, et al. Evaluating oral stimulation as a treatment for dysphagia after stroke. Dysphagia 2006; 21: 1–7.
12. Noll SF, Bender CE. Rehabilitation of patients with swallowing disorders. In: Braddom RL, Buschbacher RM, Dumitru D, Johnson EW, Matthews DJ, Sinaki MS, editors. Physical medicine and rehabilitation. 2nd edn. Philadelphia: WB Saunders; 2000, p. 553–555.
13. Rosenbek JC, Robbins J, Roecker EB, Coyle JL, Wood JL. A penetration-aspiration scale. Dysphagia 1996; 11: 93–98.
14. Park CL, O’Neill PA, Martin DF. A pilot exploratory study of oral electrical stimulation on swallow function following stroke: an innovative technique. Dysphagia 1997; 12: 161–166.
15. West JB, editor. Best and Taylor’s physiological basis of medical practice, 12th edn. Baltimore: William & Wilkins; 1991.
16. Howard L, Ament M, Fleming CR, Shike M, Steiger E. Current use and clinical outcome of home parßenteral and enteral nutrition therapies in the United States. Gastroenterology 1995; 109: 355–365.
| Appendix II. The penetration-aspiration Scale |
| Category | Score | Descriptions |
| No penetration or aspiration | 1 | Material does not enter airway. |
| Penetration | 2 | Material enters the airway, remains above the vocal folds, and is ejected from the airway. |
| 3 | Material enters the airway, remains above the vocal folds, and is not ejected from the airway. |
| 4 | Material enters the airway, contacts the vocal folds, and is ejected from the airway. |
| 5 | Material enters the airway, contacts the vocal folds, and is not ejected from the airway. |
| Aspiration | 6 | Material enters the airway, passes below the vocal folds, and is ejected into the larynx or out of the airway. |
| 7 | Material enters the airway, passes below the vocal folds, and is not ejected from the trachea despite effort. |
| 8 | Material enters the airway, passes below the vocal folds, and no effort is made to eject. |
| Appendix I. The swallow function scoring system* |
| Swallow function score | Safe liquid consistency | Clinical implication | Level of swallow deficit |
| 0 | Nothing safe (aspirates saliva) | No solid or liquid is safe | Profound |
| 1 | Saliva | Same as above (candidate for PEG) | Profound |
| 2 | Pudding, paste, ice slush | – | Substantial |
| 3 | Honey consistency (liquid with thickener or premixed product like resource brand liquid nourishment) | – | Moderate |
| 4 | Nectar consistency (pureed fruit juice such as apricot, peach, pear) | – | Mild |
| 5 | Thin liquids (e.g. cream soups, orange juice, carbonated beverage) | No coffee, tea, thin juice (e.g. apple juice), or water | Minimal |
| 6 | Water | All liquids tolerated | Normal |
| PEG: percutaneous endoscopic gastronomy. *This system identifies the consistency of liquid the patient can swallow without aspiration. |