Vocational rehabilitation
Vocational rehabilitation
Vocational rehabilitation (VR) has attracted increasing interest in recent years. We envisage 3 probable reasons for this phenomenon. One is the societal problem that occurs when too many people are on sick leave, either on sickness allowance or disability pension, causing too high or increasing costs for the national insurance system; examples are Norway, the Netherlands and Sweden. A second reason may be that the proportion of people who are retired due to age is increasing in relation to the proportion of people of working age, resulting in everyone of working ability being needed for the functioning of our societies (1). A third reason is the well-known fact that people without employment have an increased risk of disease, including an increased risk of suicide.
What is meant by VR? In Professor Anne Chamberlains (University of Leeds, UK) “Olle Höök lecture” on “Rehabilitation to work – some European perspectives”, at the yearly meeting of the Swedish Medical Association in Gothenburg, Sweden, in November 2008, she used the definition proposed by the British Society of Rehabilitation Medicine: “A process whereby those disadvantaged by illness or disability can be enabled to access, maintain or return to employment or other useful occupation”. A similar definition is used in a PhD thesis from the Karolinska Institutet (2): “Vocational rehabilitation is defined as medical, psychological, social and occupational activities aiming to re-establish among sick or injured people with previous work history their working capacity and prerequisites for returning to the labour-market, i.e. to a job or availability for a job”. This definition is also presented in a recent book on VR (3). However, the terms are sometimes used differently, e.g. that medical rehabilitation is one thing and that only the non-medical parts are called VR. Therefore some use the term “rehabilitation to work” to avoid indistinctness. The term “work-oriented medical rehabilitation” is also used. The process of an individual journey towards return to work or disability pension is illustrated in Fig. 1. Medical and non-medical rehabilitation actors are involved more or less in parallel during the process. In fact, it deals with rehabilitation at the International Classification of Functioning, Disability and Health (ICF) level of participation.
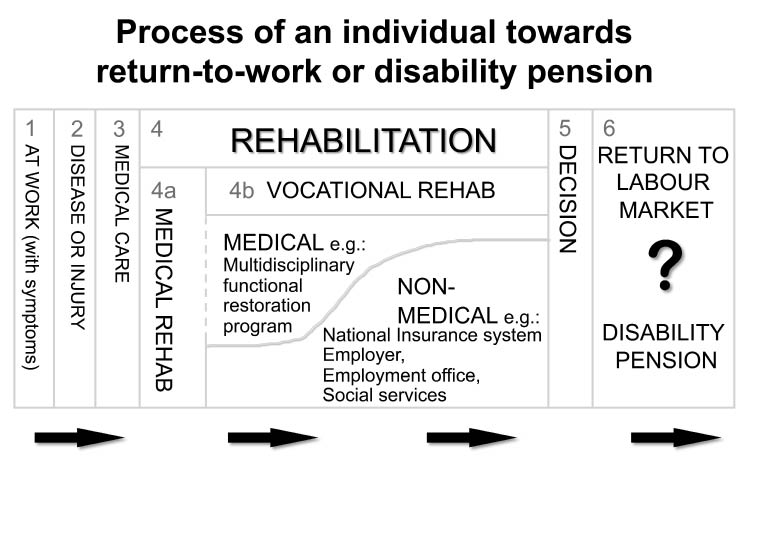
Fig. 1. The rehabilitation process towards a return to the labour market or to a disability pension (Source: modified after Ekholm J, et al., Report to Ministry of Social Welfare, Mid Sweden University, Östersund, CSF Reports No 2003:1).
An example of the current interest in the domain is the whole-day pre-congress symposium on VR held in June 2008, integrated with the 16th European Congress of Physical and Rehabilitation Medicine in Brügge, Belgium (4). After a comprehensive introduction, workshops were organized on, for example, “Pros and cons of different social security systems related to vocational rehabilitation” and “Successful projects in vocational rehabilitation leading to return to work”.
A systematic review was published in the November 2008 issue of Journal of Rehabilitation Medicine (5). Following a systematic analysis of the literature on rehabilitation and work ability it concluded that any type of rehabilitation may have an effect at an early stage of decreased work ability, being ineffective later on if applied as the only mode of rehabilitation (5). Where chronic disability is already present, multimodal medical rehabilitation needs to be combined with VR in order to reduce sick leave and disability pensions. The patients in the 45 studies included in the review had musculoskeletal pain conditions, cardiac infarction or other medical conditions.
Another review on return to work is published in the present issue of Journal of Rehabilitation Medicine (6). In this systematic review of 7 articles, including a meta-analysis, on the efficacy of multidisciplinary rehabilitation for patients on sick leave due to low back pain, evidence is shown for clinically relevant effects on work resumption in comparison with conservative treatment. The effect was better for patients with 5–11 weeks of sick leave before start of intervention than for those with more than 12 weeks.
The economic benefits of rehabilitation to work have been studied. In a study of the economic consequences of an 8-week multi-professional programme it was found that the total cost of the programme, including the cost for patients remaining on sick leave, had been recovered when the successfully rehabilitated patients had worked for 9–17 months. Any additional work after that yielded net economic benefits at the societal level (7).
In a 6-year follow-up of VR with systematic co-operation between employer, occupational health service and social insurance office, it was found that the study group had on average 5.7 fewer days on sick leave per month and person. The estimated average economic benefit, at the societal level, of the intervention was €36,600 per person, over the 6-year period (8).
An educational review on VR will be published in a forthcoming issue of Journal of Rehabilitation Medicine (9). This will focus on what trainees in rehabilitation medicine need to know about VR. Several aspects will be covered, e.g. the relationship of VR to rehabilitation medicine, legal frameworks, the most common patient groups involved, epidemiology, risk factors, models of VR, co-operation between authorities, effects of VR on return to work and sick leave.
In conclusion, research activities in the scientific domain of vocational rehabilitation are increasing; both outcome studies and process studies have been presented and more are expected. The societal relevance of the studies is high.
REFERENCES
Jan Ekholm MD, PhD, FRCP (Lond.)1, 3* and Kristina Schüldt Ekholm MD, PhD2, 3
From the 1Division of Rehabilitation Medicine, Department of Clinical Sciences, Danderyd Hospital, Karolinska Institutet, Stockholm, 2Department of Rehabilitation Science, Mid Sweden University, Campus Östersund, 3Stockholm Rehabilitation Medicine University Clinic, Danderyd Hospital, Stockholm, Sweden. *E-mail: jan.ekholm@ki.se

