SUMMARY
This paper outlines approaches to developing the International Society of Physical and Rehabilitation Medicine (ISPRM) and addresses many current challenges. Most importantly, these approaches provide the basis for ISPRM to develop its leadership role within the field of Physical and Rehabilitation Medicine (PRM) and in relation to the World Health Organization (WHO) and the United Nations (UN) system at large. They also address a number of specific critiques of the current situation. A positioning of ISPRM within the world architecture of the UN and WHO systems, as well as the consideration and fostering of respective emerging regional PRM societies, is central to establishing networking connections at different levels of the world society. Yearly congresses, possibly in co-operation with a regional society, based on a defined regional rotation, are suggested. Thus, frustration with the current bidding system for a biennial congress and an intermediate meeting could be overcome. Yearly congresses are also an important step towards increasing the organization’s funding base, and hence the possibility to expand the functions of ISPRM’s Central Office. ISPRM’s envisioned leadership role in the context of an international web of PRM journals complementing the formally defined official journal of ISPRM, regional societies, and so forth, is an inclusive rather than exclusive approach that contributes to the development of PRM journals worldwide. An important prerequisite for the further development of ISPRM is the expansion and bureaucratization of its Central Office, adding professionalism and systematic allocation of resources to the strengths of the voluntary engagement of individual PRM doctors.
Introduction
With its emergence as the pre-eminent scientific and educational international society for practitioners in the field of Physical and Rehabilitation Medicine (PRM) and its evolving role in collaboration with the World Health Organization (WHO) and the United Nations (UN) system, the International Society of Physical and Rehabilitation Medicine (ISPRM) is now facing a number of challenges. In the first chapter of this special issue, which aims to involve the constituency in the process of advancing ISPRM, we described the history and achievements of ISPRM since its foundation in 1999 and outlined the current challenges (1).
In order to address these challenges, ISPRM must now evolve into an organization that assumes a leadership role in the development of the field of PRM within the broader area of human functioning and rehabilitation. The objective of this second chapter is to outline approaches as to how ISPRM can achieve this goal. The specific aims of this chapter are: (i) to discuss ISPRM’s envisioned future role and position within the world of PRM; and (ii) to describe the development of the Central Office to meet the needs of ISPRM’s evolving role.
Role and Position of ISPRM within the World of Physical and Rehabilitation Medicine
ISPRM, as the pre-eminent international society in the field of PRM in official relation with the WHO, is in a unique position to lead and facilitate the worldwide collaboration of scientific organizations, conferences and journals in the field of PRM. Scientific societies, conferences and journals are involved in, sometimes fierce, international competition (2). However, they are also mutually dependent with respect to their common goal to advance their distinct scientific fields. While usually independent and in no formal relationship, scientific societies, journals and conferences should also have an inherent interest in collaborating as long as their specific interests coincide or are at least particularly considered, e.g. in a web of journals (3). In this paper we try to answer the question as to how ISPRM can enhance the current collaboration of PRM societies, conferences and journals.
World architecture of Physical and Rehabilitation Medicine societies
ISPRM is committed to the UN’s fundamental principle of universalism, according to which every individual has the human right to participate in and be a beneficiary of social progress and better standards of life (4). In order truly to embrace this world societal perspective, it is helpful to act on the assumption of a world architecture, comprising different levels of regional, sub-regional, national and local subunits. Communication and co-operation with the WHO and other institutions of the UN system is facilitated through the orientation of ISPRM towards their subdivision of world regions. Against this background, ISPRM also needs to develop an understanding of its position in the emerging world architecture of PRM societies as well as a vision for its future position. Only then will ISPRM be really capable of leading and facilitating PRM research and practice in collaboration with other PRM institutions worldwide. Table I and Fig. 1 show the current world architecture of PRM from a regional and international perspective in relation to the architecture of the WHO regions.
|
Table I. The world architecture of Physical and Rehabilitation Medicine from regional and international perspectives
|
|
WHO regions
|
Envisioned ISPRM large regions
|
Current ISPRM regions
|
Current regional societies
|
Envisioned regional societies
|
|
The Americas
|
The Americas (AM)
|
North America
|
na
|
tbd
|
|
Latin America
|
AMLAR
|
|
Western Pacific
|
Asia & Oceania (AO)
|
Asia & Oceania
|
AOSPRM
|
AOSPRM
|
|
Asia
|
|
The Eastern Mediterranean
|
Europe, Middle East, Africa (EMA)
|
Africa & Middle East
|
na
|
tbd
|
|
Africa
|
na
|
|
Europe
|
Europe
|
ESPRM
|
|
na: not applicable; tbd: to be defined; ISPRM: International Society of Physical and Rehabilitation Medicine; ESPRM: European Society of Physical and Rehabilitation Medicine; AMLAR: Latin American Society of Physical and Rehabilitation Medicine; AOSPRM: Asia-Oceanian Society of Physical and Rehabilitation Medicine; WHO: World Health Organization.
|
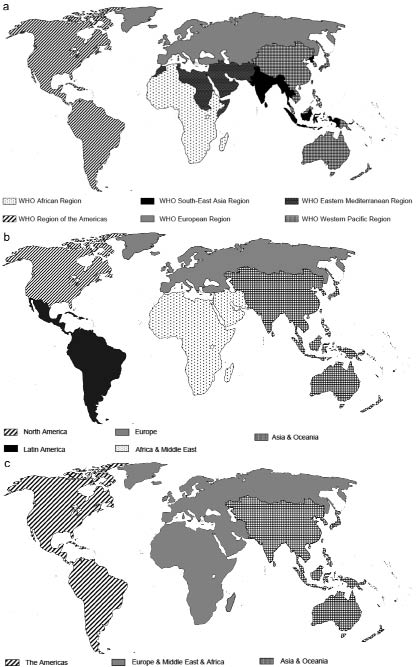
Fig. 1. World regions from the perspectives of: (a) World Health Organization (WHO); (b) International Society of Physical and Rehabilitation Medicine (ISPRM) at present and, (c) envisioned ISPRM large regions.
A number of aspects become obvious from this comparison. First, there are no regional societies in the ISPRM regions of the Middle East, Africa and Northern America. Secondly, there are 2 examples of large regions embracing southern, equatorial and northern parts of the world. The newly founded Asia-Oceanian Society of PRM (AOSPRM) is an example from the PRM perspective, while the Pan-American Health Organization (PAHO) is an example from the WHO perspective. AOSPRM can be considered a model for the development of large regional societies in the other parts of the world. In the future one may accordingly envision a world architecture of PRM with 3 large regions: Asia-Oceania (AO); Europe, Middle East and Africa (EMA); and the Americas (AM).
Three large regional societies working in close collaboration with ISPRM could importantly contribute to the strengthening of PRM from an international perspective. Recognizing also the potential advantages for ISPRM’s work, e.g. with respect to the organization of ISPRM congresses as outlined below, ISPRM may consider facilitating the creation of 3 large regional societies. More specifically, ISPRM may, in this respect, closely collaborate with the European Society of PRM (ESPRM) and the Latin American Society of PRM (AMLAR). Through its traditional links and collaboration with the Middle East and the Mediterranean Forum, ESPRM is in a unique position to lead the development towards a large region by reaching out from the northern to the southern hemisphere. AMLAR, a “tried and true” regional society seems ideally positioned to reach out to the northern American countries.
Since there is currently no regional society in the ISPRM region “Middle East and Africa”, the evolution of ESPRM into a tentative European, Middle East, and African Society of PRM (EMASPRM) seems a viable alternative to the creation of regional societies in the Middle East and Africa, which seems unlikely in the near future. Just as AOSPRM, this society may then create 2 committees matched with, and responsible for, the communication with the 2 regional WHO offices within the larger region. Also, many Mediterranean and Middle Eastern countries are already included in the Mediterranean Forum of PRM and are collaborating closely with ESPRM. The envisioned integration of ESPRM with the Middle Eastern and African region also offers the unique opportunity to support PRM physicians in the latter countries with regard to the development of the specialty. This could importantly contribute to overcoming the paradox that PRM is currently least present where it could contribute most. The collaboration of ISPRM and ESPRM in the development of PRM in Africa, the Mediterranean region and the Middle East would also be an important initiative to answer the call of the WHO resolution on disability and rehabilitation “stressing that 80% of people with disabilities, particularly in the child population, live in low income countries and that poverty further limits access to basic health services, including rehabilitation services” (5). Clearly, these regions are most in need of rehabilitation services because of “economic problems, poverty and ongoing social conflicts and wars related to disability” (5). It is also important to note that the integration of Europe with the Middle East and Africa has been a vision of our former president, the late Professor Haim Ring, who was the founder of the Mediterranean Forum. An according development in the spirit of true partnership needs to be fostered from the international level, i.e. ISPRM, in order to avoid any feelings of “being patronized” by the Europeans on the side of Africa and the Middle East.
Since it is unlikely that the USA, Canada and the English-speaking Caribbean countries will organize a regional Northern American society, an alternative would be that these countries join forces with AMLAR, which could evolve into a Pan- American society of PRM (tentatively named American Society of PRM, with the possible acronym AMSPRM). A Pan-American organization would be in line with WHO’s regional organization of PAHO and would follow the example of other medical organizations, such as the International Federation of Sports Medicine (FIMS). The integration of the Northern American countries with AMLAR would also be in line with the current paradigm shift in US policy towards increasing international consultation and collaboration on the global level, e.g. within the UN system (6), and the development of a new vision of shared continental interests in collaboration with Latin American countries (7). The integration of the Northern American region with AMLAR could importantly increase the involvement of one of the most active and powerful national PRM societies, the American Academy of PRM (AAPMR) in the regional and hence international arena. This would importantly strengthen the regional and international PRM perspective both within the Americas and globally.
The proposed naming and abbreviation of the envisioned large regional societies are oriented towards the model of AOSPRM, which includes AO as the initial letters, for the included regions Asia and Oceania, S for Society, and PRM for the scientific field. This is because the systematic use of this model would contribute to the development of a common identity for PRM worldwide and easy recognition by international institutions, including the WHO and other non-governmental organizations (NGO).
While ISPRM cannot implement the suggested developments towards 3 large regional societies, it can develop and share its vision of an international PRM architecture, which it considers most suitable for the development of the field. To facilitate such a development it could also redefine its regions, moving from currently 5 regions to 3 large regions. It could further develop formal ties with the large regional societies. In this context it could redefine its current concept of regional vice-presidents, e.g. by providing the large regional societies with the possibility to nominate candidates or even elect the regional ISPRM presidents from members of the regional boards. The idea that ISPRM’s vice-presidents should, at the same time, be members of the executive board of the respective regional society seems a preferred option in light of the fact that currently all regional vice-presidents from regions where a regional society exists are members of the respective regional board.
Whether or not ISPRM should develop formal relationships with regional societies is open to debate. A first step may be the development of working procedures for key common activities, such as the organization of joint congresses, as described in a following section.
Although ISPRM may implement its activities to facilitate 3 large international regions, it will need to be pragmatic in its relationships with national and regional societies in order to maintain a fully international presence. Co-operative relationships require that all parties see value in their participation. ISPRM cannot alienate significant national or regional organizations through imposing its vision on them without losing their representation. The ISPRM strategies will need to emphasize persuasion, inclusion and, in all likelihood, gradualism.
ISPRM congresses
ISPRM’s vision is to organize the leading international congress in PRM with respect to scientific quality and attendance. To achieve this goal, ISPRM must overcome the challenges outlined in the first chapter of this special issue (1) and must develop a loyal and engaging participant base through a sustained effort over time. This requires a number of changes in the organization of future ISPRM congresses. They include yearly instead of biennial congresses organized under the scientific and administrative leadership of ISPRM together with a host nation, and, possibly, in collaboration with a relevant regional society. Respective joint committees with representatives of ISPRM, the national host society and the regional society need to be established 2 years ahead of a congress.
Yearly meetings. ISPRM cannot develop a profile in each single member nation through congresses organized by a host nation. It could, however, develop a profile in its large regions. This would seem important, since many, if not most, individual members are more likely to attend a meeting within their region than an international meeting held in another, often distant, region, associated with high travel costs. This point has been clearly visible in the previous congresses, where the majority of attendants came from the host country and the respective region. In contrast, the international attendants came mainly from a relatively small group of internationally active members.
A prerequisite for the development of a profile in the regions is a regular presence of ISPRM in each region. Unfortunately, this is not possible with a biennial congress to be held in one out of 5 regions. Not considering variations resulting from the bidding process, ISPRM is currently present in each of its 5 regions only every tenth year.
To enhance ISPRM’s presence in the regions it seems preferable to hold an ISPRM congress every year and to rotate systematically within the 3, currently virtual, large ISPRM regions. This would allow individual members to attend an ISPRM congress in their region every third year and hence to develop a loyalty with the congress. As shown in Table III of the first chapter of this special issue (1), the switch to yearly ISPRM congresses would be possible from 2014 onward.
Joint meetings in collaboration with a regional society and a national society. A move of ISPRM towards yearly congresses to be held in the 3 large regions potentially intensifies the competition with international congresses organized by regional and sub-regional societies (1). It thus seems crucial to clarify the relationship of ISPRM with the relevant regional societies.
A most attractive solution would be yearly ISPRM congresses in collaboration with regional societies in a triennial rhythm. Since there is only one regional society in Asia-Oceania, the partner would be AOSPRM. In the large region of Europe, Africa and the Middle East, ESPRM, together with relevant national societies from the Middle East and Africa and sub-regional organizations, could serve as the host regional society for this large ISPRM region. In the large ISPRM region of the Americas, the regional society AMLAR could, together with the relevant national societies of the Northern American region, serve as collaboration partner for the triennial ISPRM meeting organized in the Americas. If, as envisioned and following the model of AOSPRM, 2 large regional societies would emerge for Europe, Middle East, Africa and the Americas, ISPRM could in the future collaborate with these societies in a triennial rhythm.
The main advantage of joint ISPRM-regional society meetings hosted by a national society is the strengthening of both the regional societies and ISPRM. The regional society benefits from a triennial international scientific exchange and international lecturers as well as a worldwide attendance. ISPRM benefits from a broad attendance of ISPRM individual members and non-member PRM physicians from the region who are loyal to their regional society meeting.
To strengthen both ISPRM and the regional societies, the regional societies might decide to move to yearly congresses as well. Besides the ISPRM world congress hosted together with a particular regional society according to the suggested rotation, ISPRM may be present at the 2 other regional congresses that year in a special ISPRM session.
The organization of ISPRM congresses in collaboration with regional societies and hosted by a national society is a major challenge. However, because of the new situation of having presidents who are not at the same time the organizers of ISPRM congresses, ISPRM is, in any case, faced with the challenge to develop suitable procedures with regard to communication and collaboration with the host nation. Therefore, it seems timely to develop a concept involving respective hybrid organizational structures and procedures. There are a number of principles that ISPRM must in the future consider in the organization of congresses in collaboration with a host nation and possibly a regional society.
Principles for ISPRM involvement in congress organization. ISPRM’s mission to organize the leading international congresses requires that ISPRM takes the lead in their scientific and administrative organization. Up till now the national host and not ISPRM carried the financial burden. ISPRM thus had to accept that it only had a consulting role with respect to the scientific programme and the financial and practical congress organization including the financially relevant registration procedures and industrial exhibition. In the future, ISPRM should consider taking primary responsibility for the scientific and administrative organization. When ISPRM will carry at least part of the financial risk it will have a say in the sharing of the gains.
With regard to the scientific organization, it is suggested that ISPRM in the future establishes joint scientific committees chaired by an ISPRM representative and involving in addition the same number of members representing ISPRM, the national society hosting the congress, and, if applicable, the collaborating regional society. The number of committee members designated by each partner should not exceed 15, and hence 46 members in total including the chairperson provided by ISPRM. Since the committee members designated by ISPRM are the holders of a “collective” or “social” memory (8, 9) and carry the experience from one congress to the next, it is important that ISPRM designates its scientific committee members for a period of several years in a “roll-over” procedure. ISPRM could, for example, elect 5 new members to its scientific committee every year in the case of a committee consisting of 15 members and a term of 3 years.
To ensure accountability with regard to the scientific content it is suggested that ISPRM develops and adopts a topic list that is altered only every few years to include emerging topics or exclude topics of decreasing importance or interest. The definition of a congress topic list contributes to a coherent definition of the field of competence as discussed in chapter 6 of this special issue (10). In light of the envisioned collaboration with the regional societies in the yearly congress, it should be developed in close collaboration with the regional societies AOSPRM, AMLAR and ESPRM. A first version of a topic list for the next ESPRM congress in 2010 in Venice, developed under the auspices of ESPRM (11), may serve as a starting point.
In addition to a congress topic list it would seem important to develop a common basic structure for international PRM congresses to ensure that both, clinically and research-oriented congress participants can count on an attractive programme covering all relevant areas over the years. Based on first suggestions (12), it would again seem useful to develop an internationally conforming basic structure in collaboration with the regional societies.
With regard to the administrative organization, it is suggested that ISPRM should in the future organize the abstract submission process and handle the registration of congress participants together with the national host and in collaboration with the regional partner society. This will ensure continuity with regard to the scientific evaluation of abstract submissions and the possibility of ISPRM’s Central Office communicating with its membership at the congress; its only possibility to interact face-to-face.
The handling of these functions will require ISPRM to develop its Central Office accordingly, as described below. Conversely, the organization of sessions, invitations and reimbursements of speakers and exhibitions in the future could also be the responsibility of the national host society. With regard to financial agreements, it is suggested that all partners, be it ISPRM and a host society or, ISPRM, a host society, and, possibly, a regional society receive a similar share from a defined part of the income generated through the congress.
As sponsorship of the congresses by industry is needed to break even, it is advised that a specific congress sponsorship committee should be set up for the recruitment of sponsors for the congress. With yearly congresses, it will become easier to convince sponsoring companies and to continue respective collaborations on a long-term basis. Presently each congress has to start from scratch again. ISPRM should have an important role in this sponsorship committee and provide its chair.
The evolution from the current decentralized model of congress sponsorship to partnerships will require that ISPRM has sufficient resources to accommodate to the risks of losses as well as congress operations. This may require an incremental strategy, perhaps first emphasizing the value of consistency of scientific content from congress to congress (11, 12).
ISPRM’s involvement in both the scientific and sponsorship committee would ensure the society’s scientific legitimacy by the means of consistency with the Policy and Procedures document (13) and organizational accountability in terms of funding, as outlined in an accompanying paper (14).
Journals
Web of Physical and Rehabilitation Medicine journals. Together with scientific societies and conferences, journals are instrumental in the development of scientific fields. Journals in particular have an important role in the dissemination of research. The publication and discussion of the results of scientific studies are essential in promoting the research process in the direction of a constant approximation of truth in the scientific community and the stimulation of new research questions. Through the breadth and depth of the publications, journals also importantly contribute to a common understanding of a scientific field or “field of competence”. In doing so, the visibility of the scientific field from outside is enhanced and identification from inside the field is facilitated (3, 15).
With respect to their common goal, to develop and maintain a distinct scientific field, societies, journals and conferences are mutually dependent. Therefore, a society must decide whether and how it will collaborate with journals of major relevance for its constituency. Beyond organizing “meet the editor” sessions at ISPRM congresses, ISPRM is challenged to define its role in the emerging collaboration of journals sharing its mission.
It is thus suggested that ISPRM considers taking the lead in the development of an international web of journals, building on an initiative by ESPRM for the European region. ESPRM has formalized its relationship with European journals which share its vision, to strengthen the field of PRM within Europe and internationally. ESPRM is envisioning a “web” of journals that collaborate in concert. Through its initiative, ESPRM by no means intends to interfere with the highly competitive scientific publication process of “original work”. Researchers will and should publish their research in the most suitable journal irrespective of a particular journal’s collaboration with scientific societies such as ESPRM or ISPRM. ESPRM does, however, hope that the envisioned web will contribute to the strengthening of the journals in such a way that they become scientifically more competitive and will attract an increasing number of the best papers in the future (3).
A web of journals can also facilitate the publication of papers that are considered not primarily “scientific”, but which are essential for the development of the field of competence. Papers of immediate relevance for the development of the field of competence include guidelines and standards as well as discussion and policy papers developed in collaboration with ISPRM, regional or national PRM societies (10, 16). The same holds true for educational articles, which must find an appropriate forum on the international, regional, language or sub-regional area or national level.
The envisioned web is also intended to facilitate the publication of articles that are of primary relevance internationally, for a specific region, language or sub-regional area, or country. Examples are papers on rehabilitation and health services provision, as well as case studies on rehabilitation care in the context of national or regional healthcare systems. Other examples are language validations of measurement instruments that are typically of interest and relevance to a national or language sub-regional area, but not necessarily to a regional or international readership.
Finally, ISPRM, together with the regional societies, can contribute to the scientific standards for journals by collaborating in the development of standards for the planning of studies and grants and the reporting of studies based on the ICF and the harmonization of author’s instructions, as described in more detail in this special issue (10).
There are numerous journals of potential relevance for the field of PRM. The reasons for this are the highly interdisciplinary orientation of rehabilitation and the broad field of functioning and rehabilitation research, ranging “from the cell to society” (17). While it would be possible to develop a far-reaching web of journals in the area of human functioning and rehabilitation (15), it seems preferable to adopt the approach by ESPRM and to develop a web of journals that are clearly dedicated to PRM. Table II shows the current list of journals collaborating in the European web of PRM journals. Tables III and IV show tentative lists of PRM journals in the Asia-Oceanian region and the American region.
|
Table II. European journals in Physical and Rehabilitation Medicine considered for the European Society of Physical and Rehabilitation Medicine (ESPRM) journal initiative in alphabetical order (3) †
|
|
Official name
|
English subtitle
|
Former name
|
Main language
|
Country of origin
|
Other languages
|
Abbreviation
|
Publisher
|
Owner
|
Societies*
|
URL (http://)
|
|
Annales de Réadaptation et de Médecine Physique
|
Intended
|
–
|
French
|
France
|
English
|
Ann Readapt Med Phys
|
Elsevier
|
SOFMER
|
SOFMER
|
www.elsevier.com/wps/find/journaldescription.cws_home/505808/description#description
|
|
Clinical Rehabilitation
|
–
|
–
|
English
|
UK
|
–
|
Clin Rehabil
|
SAGE Publications
|
SAGE Publications
|
BSRM VRA
|
cre.sagepub.com
|
|
European Journal of Physical and Rehabilitation Medicine
|
–
|
Europa Medicophysica
|
English
|
Italy
|
–
|
Eur J Phys Rehabil Med
|
Edizioni Minerva Medica
|
Edizioni Minerva Medica
and
Italian Society of Physical and Rehabilitation Medicine
|
ESPRM
SIMFER
MFPRM
EEFIAP
TSPRMS
|
www.minervamedica.it
www.ejprm.org
|
|
Fizikalna i Rehabilitacijska Medicina
|
Intended
|
–
|
Croatian
|
Croatia
|
English
|
Fiz Rehabil Med
|
CSPRM
|
CSPRM
|
CSPRM
|
|
|
Journal of Rehabilitation Medicine
|
–
|
Scandinavian Journal of Rehabilitation Medicine
|
English
|
Sweden
|
–
|
J Rehabil Med
|
Foundation of Rehabilitation Information
|
Foundation of Rehabilitation Information
|
ISPRM
|
www.medicaljournals.se/jrm
|
|
Medicina Física e Reabilitação
|
Intended
|
–
|
Portuguese
|
Portugal
|
English
French
Spanish
|
–
|
SPMFR
|
SPMFR
|
SPMFR
|
|
|
Physikalische Medizin, Rehabilitationsmedizin und Kurortmedizin
|
Journal of Physical and Rehabilitation Medicine
|
–
|
German
|
Germany
|
English
|
Phys Med Rehab Kuror
|
Thieme-Verlag
|
Thieme-Verlag
|
DGPMR
ÖGPMR
|
www.thieme.de/fz/physmed
www.thieme-connect.de/ejournals
|
|
Romanian Journal of Physical and Rehabilitation Medicine
|
–
|
Revista de Recuperare, Medicină Fizică şi balneologie
|
English
|
Romania
|
Romanian
|
Ro J Phys Rehabil Med
|
“Carol Davila” University Press. Bucharest
|
SRFMR
|
SRFMR
|
|
|
*Some journals may also have relationships with other organizations than shown in the table (e. g. Journal of Rehabilitation Medicine is also the official journal of the Physical and Rehabilitation Medicine Board of the European Union of Medical Specialists (UEMS) and the European Academy of Rehabilitation Medicine).
†Additional European journals, e. g. from Spain and Turkey, are currently also under consideration.
BSRM: British Society of Rehabilitation Medicine; CSPRM: Croatian Society of Physical and Rehabilitation Medicine; DGPMR: Deutsche Gesellschaft für Physikalische Medizin und Rehabilitation; EEFIAP: Hellenic Society of Physical and Rehabilitation Medicinen; ESPRM: European Society of Physical and Rehabilitation Medicine; ISPRM: International Society of Physical and Rehabilitation Medicine; MFPRM: Mediterranean Forum of Physical Medicine and Rehabilitation; SIMFER: Italian Society of Physical and Rehabilitation Medicine; SOFMER: Société Française de médecine physique et de réadaptation; SPMFR: Sociedade Portuguesa de Medicina Física e de Reabilitação; SRFMR: Societatea Medicină Fizică şi de Recuperare; VRA: Nederlandse Vereniging van Revalidatieartsen; TSPRMS: Turkish Society of Physical Medicine and Rehabilitation Specialists; ÖGPMR: Österreichische Gesellschaft für Physikalische Medizin und Rehabilitation.
|
|
Table III. Asia-Oceanian journals in Physical and Rehabilitation Medicine in alphabetical order
|
|
Official name
|
English subtitle
|
Former name
|
Main language
|
Country of origin
|
Other languages
|
Abbrevia–
tion
|
Publisher
|
Owner
|
Societies
|
URL (http://)
|
|
Asia Pacific Disability Rehabilitation Journal
|
–
|
–
|
English
|
India
|
–
|
–
|
National Printing Press
|
Sponsored by
Action for Disability Cordaid
|
Action for Disability Cordaid
|
www.aifo.it/english/resources/online/apdrj/journal.htm
|
|
Chinese Journal of Physical Medicine and Rehabilitation
|
–
|
Chinese Journal of Physical Medicine
|
Chinese
|
China
|
English abstract
|
–
|
Chinese Journal of Physical Medicine and Rehabilitation Editing Committee
|
Chinese Medical Association
Medical School of Hua Zhong Science & Technology University
|
CSPRM
|
www.cjpmr.cn/zhwl/WEB/InitialPage.aspx
|
|
Chinese Journal of Rehabilitation
|
–
|
–
|
Chinese
|
China
|
–
|
–
|
Chinese Electronic Periodical Services
|
China Disabled Persons Federation
Chinese Rehabilitation Society
Medical School of Hua Zhong Science & Technology
|
CARDP
|
www.zglckf.com/
|
|
Chinese Journal of Rehabilitation Medicine
|
–
|
–
|
Chinese
|
China
|
English abstract
|
–
|
Chinese Electronic Periodical Services
|
Ministry of Health, China
Chinese Rehabilitation Society
|
Chinese Association of Rehabilitation Medicine
|
www.rehabi.com.cn/ch/index.aspx
|
|
Chinese Journal of Rehabilitation Theory and Practice
|
–
|
–
|
Chinese
|
China
|
English abstract
|
–
|
Chinese Electronic Periodical Services
|
China Disabled Persons Federation
Chinese Rehabilitation Society
Chinese Doctors Society
Chinese Rehabilitation Research Center
|
CARDP
|
www.crrc.com.cn/trsweb/search.wct?channelid=8583
|
|
Clinical Rehabilitation Tissue Engineering Research
|
–
|
Chinese Clinical Rehabilitation
|
Chinese
|
China
|
English
|
–
|
Chinese Journal of Clinical Rehabilitation Press
|
Chinese Rehabilitation Medical Association
Ministry of Health, China
|
CARM
|
en.zglckf.com/sites/English/List_2025_9463.html
|
|
Japanese Journal of Rehabilitation Medicine
|
–
|
–
|
Japanese
|
Japan
|
English abstract
|
Jpn J Rehabil Med
|
JARM
|
JARM
|
JARM
|
wwwsoc.nii.ac.jp/jarm/
|
|
Journal of Thai Rehabilitation Medicine
|
–
|
–
|
Thai
|
Thailand
|
English
|
J Thai Rehabil Med
|
Suthin Publisher, Chiangmai
|
The Royal College of Physiatrists of Thailand
|
TRMA
|
www.rehabmed.or.th
|
|
The Journal of Korean Academy of Rehabilitation Medicine
|
–
|
–
|
Korean
|
Korea
|
English abstract
|
J Korean Acad Rehabil Med
|
KARM
|
KARM
|
KARM
|
www.karm.or.kr
|
|
CARDP: China Association of Rehabilitation of Disabled Persons; CARM: Chinese Association of Rehabilitation Medicine; CJRTP: Chinese Journal of Rehabilitation Theory and Practice; CJPMR: Chinese Journal of Physical Medicine and Rehabilitation; CSPRM: Chinese Society of Physical Medicine and Rehabilitation; JARM: Japanese Association of Rehabilitation Medicine; KARM: Korean Academy of Rehabilitation Medicine; TRMA: Thai Rehabilitation Medicine Association.
|
|
Table IV. American journals in Physical and Rehabilitation Medicine in alphabetical order
|
|
Official name
|
English subtitle
|
Former name
|
Main language
|
Country of origin
|
Other languages
|
Abbreviation
|
Publisher
|
Owner
|
Societies
|
URL (http://)
|
|
Acta Fisiátrica
|
–
|
–
|
Portuguese
|
Brazil
|
English abstracts
|
Acta Fisiatr
|
Divisão de Medicina de Reabilitação Hospital das Clínicas, University of São Paulo School of Medicine
|
Divisão de Medicina de Reabilitação Hospital das Clínicas, University of São Paulo School of Medicine
|
–
|
www.actafisiatrica.org.br
|
|
American Journal of Physical Medicine & Rehabilitation
|
–
|
–
|
English
|
USA
|
–
|
Am J Phys Med Rehabil
|
Lippincott Williams & Wilkins
|
AAP
|
AAP
|
www.amjphysmedrehab.com/
|
|
Archives of Physical Medicine and Rehabilitation
|
–
|
–
|
English
|
USA
|
–
|
Arch Phys Med Rehabil
|
Thomson Reuters
|
Elsevier
|
ACRM
|
www.archives-pmr.org/
|
|
Boletín de Rehabilitación Médica
|
–
|
–
|
Spanish
|
Venezuela
|
–
|
Bol Rehabil Méd
|
Ministerio de Sanidad y Asistencia Social, Departamento de Rehabilitación Médica
|
–
|
–
|
–
|
|
Jornal do Fisiatra
|
–
|
–
|
Portuguese
|
Brazil
|
–
|
–
|
ABMFR
|
ABMFR
|
ABMFR
|
www.fisiatria.org.br/
|
|
Medicina de Reabilitação
|
–
|
–
|
Portuguese
|
Brazil
|
English abstracts
|
Med Reabil
|
ABMFR
|
Centro de Estudos e Pesquisa Medicina de Reabilitação
|
AMLAR
ABMFR
SPMFR
ASCEP
|
–
|
|
PM&R
|
–
|
–
|
English
|
USA
|
–
|
PM&R
|
Elsevier
|
AAPM&R
|
AAPM&R
|
www.pmrjournal.org/
|
|
Reabilitar
|
–
|
–
|
Portuguese
|
Brazil
|
–
|
–
|
–
|
–
|
–
|
–
|
|
Rehabilitación: enfoque integral de la discpacidad
|
–
|
–
|
Spanish
|
Argentina
|
–
|
–
|
–
|
–
|
–
|
–
|
|
Revista Argentina de Rehabilitación
|
–
|
–
|
Spanish
|
Argentina
|
English abstract
|
–
|
SAMFYR
|
SAMFYR
|
SAMFYR
|
www.samfyr.org/revista_argentina2.php?id=12
|
|
Revista Colombiana de Medicina Física y Rehabilitacion
|
–
|
–
|
Spanish
|
Colombia
|
English abstract
|
–
|
ASCMF&R
|
ASCMF&R
|
ASCMF&R
|
ascmfr.homestead.com/publicaciones.html#anchor_15
|
|
Revista Medicina Física e Reabilitação
|
–
|
–
|
Portuguese
|
Brazil
|
–
|
–
|
SPFMR
|
SPFMR
|
SPFMR
|
www.spmfr.org.br/revista.asp
|
|
Revista Mexicana de Medicina Física y Rehabilitación
|
–
|
–
|
Spanish
|
Mexico
|
English
|
Rev Mex Med Fis Rehab
|
SMMFR
|
SMMFR
|
SMMFR
|
www.medigraphic.com/espanol/e-htms/e-fisica/em-mf.htm
|
|
AAP: Association of Academic Physiatrists; AAPM&R: American Academy of Physical Medicine and Rehabilitation; ABMFR: Associação Brasileira de Medicina Física e Reabilitação; ACRM: American Congress of Rehabilitation Medicine; AMLAR: Latin American Society of Physical and Rehabilitation Medicine; ASCEP: Associçäo de serviço à criança Excepcional; ASCMF&R: Asociación Colombiana de Medicina Física y Rehabilitación; SAMFYR: Sociedad Argentina de Medicina Física y Rehabilitación; SMMFR: Sociedad Mexicana de Medicina Física y Rehabilitación ; SPFMR: Sociedade Paulista de Medicina Física e Reabilitação; SPMFR; Sociedade Brasileira de Medicina Física e Reabilitaçäo.
|
Formal relationships. If ISPRM decides to follow the model of ESPRM it would need to formalize relationships with individual journals, taking into account the varying scope of each journal and the current level of international competitiveness. ISPRM would accordingly opt for the re-designation of its official journal, the Journal of Rehabilitation Medicine (JRM) for administrative and organizational issues, and the fostering of a truly international highly competitive journal. It would then formalize its relationship with journals that publish articles both in English and national languages under consideration of their international scientific competitiveness. All journals that aim to establish official relations with ISPRM would need to fulfil the first 4 out of the 6 criteria shown in Table V. Journals fulfilling all 6 criteria would be “published in association with ISPRM”, while journals fulfilling at least 4 criteria would be “endorsed by ISPRM”. Editorial boards are selected by the journals on pure scientific grounds and the members do not represent any organization. An appropriate arrangement of the contacts between the organizations and the journal would therefore be to have special contact persons with the specific role of discussing principles for the collaboration between the journal and the organization, including publication of statement papers and educational reviews.
|
Table V. Criteria for the collaborations of journals in Physical and Rehabilitation Medicine with the International Society of Physical and Rehabilitation Medicine (ISPRM) (3). Fulfilment of all 6 criteria qualifies for “publication in association with ISPRM”, fulfilment of the first 4 criteria qualifies for “endorsed by ISPRM”
|
|
Criteria
|
Description
|
|
I
|
Publications in English
(It is possible to publish articles in other languages if an English abstract is provided)
|
|
II
|
English title or subtitle referring to the medical specialty Physical and Rehabilitation Medicine (It is possible to carry a title or subtitle in another language)
|
|
III
|
Involvement in the editorial board of at least 2 ISPRM scientists named by the journal in consultation with ISPRM
|
|
IV
|
Provision of space for ISPRM relevant information
|
|
V
|
Impact Factor should exist
|
|
VI
|
Citation in relevant databases such as Medline
|
Official journal. ISPRM is in the unique position that, since 2006, it has relied on the well-established JRM as its official journal. While the JRM is not owned by ISPRM, it is run by an independent non-profit foundation and published independently of a commercial editor. JRM would welcome a representative of ISPRM as an observer in meetings of its foundation. It sees itself as an international journal based in Sweden covering all aspects of PRM. While already highly international with respect to its editorial board, JRM is committed ultimately to involve scientists on parity from all 3 large ISPRM regions.
Based on its positive experience with the publication of the abstracts from the first AOSPRM congress in 2009 and the ESPRM congress in 2009, JRM is committed to publishing the abstracts from ISPRM or joint ISPRM/regional societies hosted by an ISPRM member country in the future. JRM is also committed to publishing a reasonable number of discussion and policy papers concerning ISPRM’s internal and external policy process, as described in accompanying chapters of this special issue (10, 16). These papers would be reviewed in order to meet the scientific standards of the journal.
The JRM is currently not an open access journal. However, it provides free access to its articles after one year. In addition, it provides open access to selected reviews, special reports and educational articles. More importantly, all individual members of ISPRM have immediate access to the electronic version of the journal. To benefit as many individual members as possible worldwide, it is therefore important to encourage national societies to negotiate a flat fee for all its individual members.
Development of the Central Office
One of the most important organizational challenges to ISPRM is to further develop its Central Office. In order to meet the challenges set out in the first chapter of this special issue, it is suggested that ISPRM strengthens its Central Office in order to make it an even more important and supportive part of ISPRM’s development efforts and goal attainment (1).
General principle
The general principle behind this development is the change from voluntary engagement of charismatic persons to bureaucratic authority (14, 18). Clearly, this pre-supposes higher financial investment.
Additional professional staff. Ideally, in the future the manager or central executive officer (CEO) of ISPRM who should have experience in PRM as well as in professional management is supported by additional staff. This should be, on one hand, vertically integrated middle management and assistants to whom specific fields such as public relations and tasks in relation to ISPRM’s strategic plan (16, 19) may be delegated, and horizontally integrated consultants with expertise in specific areas of PRM.
Financing change – a first step. A first step towards financing such a bureaucratic expansion of the Central Office might be, as mentioned above, to place the organization of ISPRM congresses and the administration of subsequent fees into ISPRM’s, i.e. the Central Office’s, hands. Also, ISPRM membership of national societies might in the future be limited to combined membership, so that all national societies would have to pay a lump sum for their individual members (1). In addition to the financial advantages, this would spread the ISPRM mission within a large number of individual members, e.g. through open access to ISPRM’s official journal.
Key duties of the Central Office
In addition to the envisioned involvement of the congress organization, a set of key duties of the enhanced Central Office would exist. These would be centred on membership management and liaison and fundraising activities.
Membership management and liaison duties. A key duty would be to enhance membership management, including the collection of membership fees and the recruitment of national and individual members worldwide.
Additionally, the Central Office would foster liaison with other PRM societies, other professional organizations in official relation with the WHO, such as the World Federation for Occupational Therapy (WFOT), as well as government representatives. This would link the development of ISPRM’s activities directly to the agendas of other key players (20).
Public relations and fundraising. Another key duty would be the representation and presentation of ISPRM and its activities to international media, thus communicating the society’s visions and goals to a global audience (21).
Finally, and elementary in bolstering the growth of ISPRM’s influence in the future, the Central Office would – in close collaboration with the board, ISPRM’s sponsorship committee, and its educational and development fund envision, compile, and manage the strategic plan, including fundraising activities, in particular the creation of new funding streams.
These new funding streams into ISPRM from private or public sources would, on one hand, be used to finance ISPRM’s internal organizational tasks and activities. On the other hand, these new streams would be redirected to support projects in possible global public private partnerships (GPPP) with the goal of delivering rehabilitation services in developing countries (22). ISPRM may, in the future, facilitate such projects by offering consulting with regard to their implementation, supervision and monitoring of standards (10).
Preliminary objectives and first tasks of the enhanced Central Office
In order to build and maintain such a pivotal organizational structure 2 preliminary objectives are at hand: firstly, to employ additional management and public relations experts via professional recruitment; secondly, to create new and readjust current funding streams to establish a sufficient Central Office budget for the challenges ahead. Then, a sequence of important tasks can be managed.
Central contact database. The first task of the Central Office management would be to set up a central database of all existing and new PRM relevant networking contacts, including regional and international, individual and institutional contacts in the private and public realm.
These include: all national and regional PRM societies, other international, regional and national NGOs relevant to PRM including other health professional societies (20) and disability advocacy organizations, governments, government ministries and institutions, health experts from different political parties, private companies, existing GPPPs (22, 23), social movements postulating the establishment of rehabilitation services, interest groups, and the mass media.
Public relations network. Secondly, a public relations network would be set up (24). To this end, a set of appropriate networking tools would be defined. Among these are face-to-face contacts, telephone calls to private and public contacts, e-mail, posters and presentations, speeches, specially organized ISPRM venues (congresses, meetings, lunches, dinner speeches, open-spaces, fundraising venues), sponsorship, etc. Since different communication tools involve different levels of media richness, i.e. types of information (e.g. emotions, content, pictures) which can be exchanged, each tool or combination of tools may be used for specific communication goals (25, 26).
Management of ISPRM presence at relevant venues. Thirdly, according to the ISPRM strategic plan, the Central Office would review relevant venues worldwide where ISPRM should be present. Public relations activities (27) are to raise awareness within the world society and nation states necessary for the acquisition of new funding streams (28).
Relevant venues may include PRM congresses and scientific meetings, international and national trade fairs, exhibitions, public and closed government sessions and consultations at the international, regional, sub-regional, national, and local level, as well as private venues sponsored by companies relevant to PRM.
ISPRM’s Central Office would also organize new kinds of venues to present ISPRM’s activities and discuss these with different groups. Discussion forums (open spaces) and expert meetings with representatives from media, politics, the private sector and other interest groups such as disabled persons organizations (DPOs), development projects, capacity building initiatives, and so forth, would be held.
At all of the above-mentioned venues members of the Central Office’s public relations team and ISPRM regional representatives would make direct face to face contact and create new networking links and concrete agreement on new partnerships towards a boundary-less enterprise (29). These joint partnerships may be contracted sponsorship agreements, joint programme agreements, joint public relations initiative agreements and many more. At the centre of these networking initiatives would, of course, be the planned yearly congresses organized by ISPRM itself.
Conclusion
The outlined approaches for developing ISPRM address many challenges. They provide the basis for a respective decision process within the responsible bodies of ISPRM (Table VI).
|
Table VI. Summary of issues and decision points on “developing International Society of Physical and Rehabilitation Medicine (ISPRM)”
|
|
Issues
|
Decision points
|
|
Enhancing the ISPRM policy process and agenda
|
Establishing a systematic internal policy process in relation to the PRM constituency
|
|
Establishing an external policy process in relation to WHO, other professional organizations and NGOs
|
|
Systematic development of quadrennial policy agendas for the internal and external policy process
|
|
Systematic development of the networking in relation to the external policy process through participation and initiation of relevant meetings
|
|
Professionalization of the Central Office
|
Organization of the ISPRM congress through the ISPRM Central Office
|
|
Generation of the funding necessary for the professionalization and expansion of the Central Office through the income generated by the organization of yearly ISPRM congresses and development of a sponsor network
|
|
Co-ordination of the internal and external policy process and planning of the policy agenda through the Central Office staff
|
|
Participation and initiation of relevant meetings in relation to the external policy process through the Central Office staff in collaboration with ISPRM officials
|
|
Enhancing ISPRM congresses
|
Move to yearly ISPRM congresses (earliest possibility, 2014)
|
|
Systematic rotation of the congress location in the 3 large regions Asia/Oceania, Europe/Middle East/Africa, Americas
|
|
Organization of the ISPRM congresses by its Central Office
|
|
Co-operation in the ISPRM congresses with the regional societies AOSPRM, ESPRM and AMLAR
|
|
Enhancing PRM journals
|
Nomination of JRM as ISPRM’s only official journal
Observer role of ISPRM‘s Central Office in the non-profit foundation running JRM
Publication of articles relevant for the internal and external policy process in ISPRM‘s official journal (JRM)
|
|
Fostering of PRM journals worldwide through the facilitation and collaboration with webs of journals in the 3 large regions
|
|
Establishing collaborations with the regional societies
|
Co-operation with the regional societies AOSPRM, ESPRM and AMLAR in the yearly ISPRM congress
|
|
Facilitation of the evolution of current regional societies towards large regional societies in Europe/the Middle East/Africa and the Americas
|
|
Nomination of the regional ISPRM vice presidents by the regional societies AOSPRM, ESPRM and AMLAR
|
|
PRM: Physical and Rehabilitation Medicine; JRM: Journal of Rehabilitation Medicine; NGO: non-governmental organization; ISPRM: International Society of PRM; ESPRM: European Society of PRM; AMLAR: Latin American Society of PRM; AOSPRM: Asia-Oceanian Society of PRM; WHO: World Health Organization.
|
References

