OBJECTIVE: To explore the main barriers to and facilitators of physical activity in young adults with childhood-onset physical disabilities.
DESIGN: Qualitative study using focus groups.
PARTICIPANTS: Sixteen persons (12 men and 4 women) aged 22.4 (standard deviation 3.4) years, of whom 50% were wheelchair-dependent, participated in the study. Eight were diagnosed with myelomeningocele, 4 with cerebral palsy, 2 with acquired brain injury and 2 with rheumatoid arthritis.
METHODS: Three focus group sessions of 1.5 h were conducted using a semi-structured question route to assess perceived barriers to and facilitators of physical activity. Tape recordings were transcribed verbatim and content analysed. According to the Physical Activity for People with a Physical Disability model, barriers and facilitators were subdivided into personal factors and environmental factors.
RESULTS: Participants reported several barriers related to attitude and motivation. In addition, lack of energy, existing injury or fear of developing injuries or complications, limited physical activity facilities, and lack of information and knowledge, appeared to be barriers to physical activity. Fun and social contacts were mentioned as facilitators of engaging in physical activity, as well as improved health and fitness.
CONCLUSION: Young adults with childhood-onset physical disabilities perceived various personal and environmental factors as barriers to or facilitators of physical activity. These should be taken into account when developing interventions to promote physical activity in this population.
Key words: disabled persons, young adult, motor activity, focus group, barriers and facilitators.
J Rehabil Med 2009; 41: 881–885
Correspondence address: Laurien M. Buffart, Erasmus MC, Department of Rehabilitation Medicine, PO Box 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: l.buffart@erasmusmc.nl
Submitted January 13, 2009; accepted May 14, 2009
INTRODUCTION
Due to advances in medical technology and care, the majority of children with physical disabilities such as myelomeningocele (MMC), cerebral palsy (CP) or brain injury (BI) survive into adulthood (1–3). As a consequence, healthcare is shifting from disability prevention towards health promotion, in order to prevent secondary conditions and to ensure a healthy adult life (4). Secondary conditions affecting people with physical disabilities include osteoporosis, decreased balance, reduced muscle strength and endurance, reduced aerobic fitness, increased spasticity, overweight, hypertension and depression. With increasing age, lifestyle-related diseases, such as diabetes mellitus and cardiovascular diseases, may also be of concern. Encouraging physical activity (PA) is important for health promotion, and is assumed to have positive effects on secondary conditions, and on functional independence, social integration, and life satisfaction (5, 6).
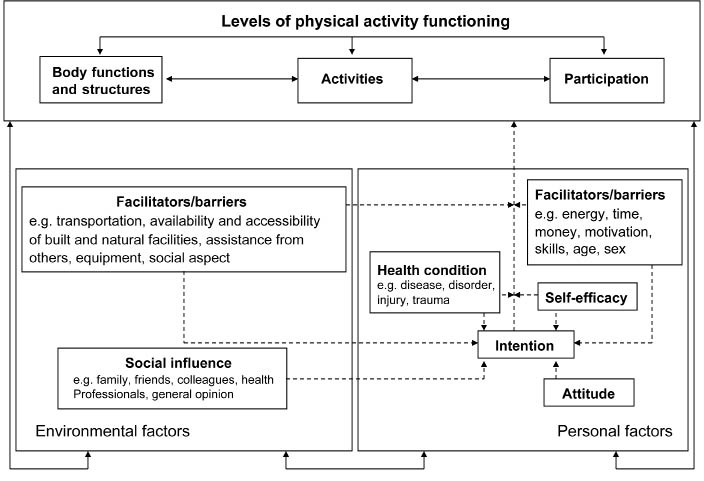
Previous studies in adolescents and young adults with MMC and CP showed low levels of PA and low aerobic fitness, compared with able-bodied people of the same age (7–9). In order to develop programmes to promote PA in people with childhood-onset physical disabilities, it is important to understand the factors that determine PA behaviour in this population (10, 11). To describe factors associated with PA in people with a physical disability, van der Ploeg et al. (12) proposed the Physical Activity for People with a Disability (PAD) model (Fig. 1). The model uses the International Classification of Functioning, Disability and Health (ICF) as its starting point. The ICF model describes the functioning of an individual in a specific domain as a dynamic interaction or complex relationship with environmental and personal factors, given a certain health condition (12). In the PAD model, PA behaviour and its correlates were integrated into the ICF model (13).
Fig. 1. Physical Activity for People with a Disability (PAD) model. Published with permission from the author H. P. van der Ploeg (12).
According to the PAD model, several personal and environmental factors may influence PA behaviour. While knowledge of the barriers to and facilitators of PA for the general adolescent and young adult population is increasing (14–16), such studies are scarce in young adults with childhood-onset physical disabilities. In adolescents and young adults with MMC and CP, ambulatory status, or gross motor function, was found to be associated with PA levels, whereas gender was not (8, 9). With regard to intervention development, identification of such non-modifiable factors is important for defining subgroups that are at increased risk of developing an inactive lifestyle, or subgroups that need a different approach to promote PA. However, to change PA behaviour, it is relevant to focus more on modifiable barriers and facilitators of PA, including psychological, physical and environmental factors. In adults with CP, the caregiver’s perceived benefits of exercise and the type of residence appeared to be determinants for exercise participation (17). Furthermore, a previous study in adolescents and young adults with MMC showed that sports participation was associated with higher self-efficacy, exercise enjoyment, physical appearance, and social support (18). However, sports participation is a planned and structured sub-category of PA (19), and results may not hold for daily PA in general. Using focus groups, Rimmer et al. (20) studied barriers to and facilitators of PA in adults (mean age 40.2 years) with various types of physical disabilities, including people with limited ability of using the upper or lower extremities, people with spinal cord injuries and people with back problems. However, somewhat different barriers to and facilitators of PA may play a role in young adults compared with older adults, and in people with childhood-onset physical disabilities compared with disabilities acquired during adulthood. This study therefore aimed to explore barriers to and facilitators of PA, as perceived by young adults with childhood-onset physical disabilities.
METHODS
Participants
Three focus group sessions were conducted with a convenience sample of young adults with childhood-onset physical disabilities. Participants were eligible for the study when they were between 16 and 30 years, they did not have learning disabilities and were known in the outpatient rehabilitation department of Erasmus Medical Center (MC) and Rijndam Rehabilitation Center, both in Rotterdam, and Sophia Rehabilitation Center in The Hague. Thirty-two young adults with MMC or CP who had been involved in previous studies were sent postal invitations, and 14 agreed to participate. Four of them were not available on the days of the interviews. Six additional participants were invited via their treating physical therapist in the young adult team. This resulted in the participation of 16 young adults (12 men and 4 women) aged 22.4 (standard deviation (SD) 3.4; range 18–30) years, of whom 50% were wheelchair-dependent. Eight participants were diagnosed with MMC, 4 with CP, 2 with acquired BI and 2 with rheumatoid arthritis (RA). The medical ethics committee of Erasmus MC approved this study. All participants gave written informed consent before the start of the focus group interviews.
Procedures
Focus group sessions were facilitated by 2 members of the research team (LB and TW). At the beginning of each focus group session, the purpose of the study was explained and written informed consent was obtained. A semi-structured question route was used during the focus group sessions (Appendix I). Participants were asked about factors influencing their PA behaviour, including daily PA and sports; assessing reasons for participation or non-participation. Furthermore, participants were asked about their preferences on how they felt that PA could be improved, which resulted in additional facilitators of PA. Groups ran for approximately 1.5 h.
Data analyses
Focus group sessions were audio-taped, and the tapes were transcribed verbatim to ensure systematic analyses of the interviews. Tape recordings of the sessions were content analysed by 2 members of the research team (LB and TW), which involved the systematic examination of the transcripts to identify major categories of barriers to and facilitators of PA. According to the PAD model, barriers and facilitators were subdivided into personal factors and environmental factors, including the social and physical environment.
RESULTS
Nearly all participants mentioned they had been involved in sports sometime during childhood. Some of them stopped sports participation during adolescence or young adulthood due to injuries or complications associated with their condition, or other priorities. Various personal and environmental factors that participants perceived as barriers to and facilitators of PA are presented in Tables I and II, respectively.
| Table II. Environmental barriers to and facilitators of physical activity (PA) in adolescents and young adults with childhood-onset physical disabilities |
| Barriers | Facilitators |
| Social environment | Social environment |
| Lack of professional support | Social contacts |
| | Social support Parents Professionals Peers/friends Sports team School |
| Physical environment | Physical environment |
| Bad weather | Nice weather |
| Having a car (also use the car for short distances instead of active transportation, i.e. walking, (hand)cycling) | Having a car (it facilitates transportation to PA locations) |
| PA facilities Limited facilities, particularly for young people and in rural areas Distance to facilities Opening hours Crowdedness | Having a dog |
| Equipment Expensive Inappropriate (not adapted for people with physical disabilities) It takes a long time to acquire the equipment after purchasing it | |
| Lack of information/knowledge on Where to exercise How to exercise Physical and medical consequences | |
| Transportation problems Duration (waiting for taxi) Costs (public transport, taxi) Dependency upon others Carrying equipment in public transport | |
| Other | Other |
| Financial/costs Expensive equipment Expensive entrance of facilities Transportation to facilities | |
| Table II. Environmental barriers to and facilitators of physical activity (PA) in adolescents and young adults with childhood-onset physical disabilities |
| Barriers | Facilitators |
| Social environment | Social environment |
| Lack of professional support | Social contacts |
| | Social support Parents Professionals Peers/friends Sports team School |
| Physical environment | Physical environment |
| Bad weather | Nice weather |
| Having a car (also use the car for short distances instead of active transportation, i.e. walking, (hand)cycling) | Having a car (it facilitates transportation to PA locations) |
| PA facilities Limited facilities, particularly for young people and in rural areas Distance to facilities Opening hours Crowdedness | Having a dog |
| Equipment Expensive Inappropriate (not adapted for people with physical disabilities) It takes a long time to acquire the equipment after purchasing it | |
| Lack of information/knowledge on Where to exercise How to exercise Physical and medical consequences | |
| Transportation problems Duration (waiting for taxi) Costs (public transport, taxi) Dependency upon others Carrying equipment in public transport | |
| Other | Other |
| Financial/costs Expensive equipment Expensive entrance of facilities Transportation to facilities | |
Personal barriers and facilitators
Physical aspects that were mentioned as barriers to PA included having an injury or a complication associated with the condition, and lack of energy or being fatigued (Table I).
“When I’m tired or when my knee hurts, I’m not going cycling. But I think it is mainly fatigue, I don’t want to waste my last bit of energy on doing sports; I would rather do something else with the energy that I have left.”
Some participants mentioned that they did not exercise because they felt that it did not lead to any health benefits. For others, improved health was a reason to be physically active. Also maintenance of fitness, muscle strength, functional independence, and physical appearance were mentioned as reasons for engaging in PA.
“I started fitness because I know doing sports is healthy, and I want to keep in shape in its broadest sense, including the way I look.”
Psychological barriers that were mentioned in the focus groups included feeling uncomfortable or ashamed when engaging in PA, fear for complications or injuries, and several motivational barriers, such as lack of time (due to school or work), having other priorities, changing clothes being too much effort, or having to wake up early.
“I couldn’t combine wheelchair hockey with my study anymore, and I had to wake up early on Saturday morning, I had to travel far to go there, and my father had to take me there, because I couldn’t take my wheelchair on the bus. And I use public transport all the time, so I hardly use my bicycle to go anywhere.”
“When I was 13 years old, I started with wheelchair dancing via a friend. I danced for 11 years, but I had to stop that because it was too strenuous for my shoulders. It started with a bursitis, but became a chronic joint inflammation…. Now I am still searching for something else. I really would like to go swimming, but I have many doubts about that because I have had a pressure sore several times. So I am still searching for the right sport that gives the least damage to my body.”
Attitude (“If I want to be active, I will”) was a psychological facilitator of PA. Furthermore, wanting to win or achieve a goal, and clearing the mind, were mentioned as reasons for being physically active. In addition, several motivational facilitators were mentioned, including perceiving feelings of fulfilment and enjoyment, having a physical challenge, or being rewarded after exercise, for example by social events. Other reasons for being physically active were the use of active transportation, e.g. cycling to work or wheeling to the shops, and because it was a habit, since they had done so since childhood.
Environmental barriers and facilitators
Table II presents perceived barriers to and facilitators of the physical and social environment. Lack of professional support was mentioned as a PA barrier of the social environment, and social contacts as a facilitator.
“In my opinion, people always do sports for social contacts, unless people just need to lose weight or so.”
Furthermore, PA was often facilitated by others; family and friends had an important role in stimulating the young adult for being physically active, as well as facilitating transportation to facilities and having somebody to be active with.
“My parents stimulated me, well, they supported me. I didn’t have to, but if I wanted to exercise it, they helped me with it.”
“They stimulate me here at the rehabilitation centre. My physical therapist is an enormous support for me; he says it is good for me to exercise, so I do it.”
Aspects of the physical environment also appeared to influence PA. Bad weather was mentioned as a barrier to PA, whereas good weather was a facilitator. Having a car was a barrier to active transport (walking, (hand)cycling, wheelchair driving), but it appeared to facilitate the ability to go to sports and exercise facilities.
“Being able to drive my car gives me extra time and flexibility to go anywhere I like, also to go to my sports club. But it makes me lazier too. Since I have that car it is difficult not to also use it for travelling short distances.”
PA facilities (e.g. sports or exercise classes) also appeared to be limited, particularly in rural areas, or they were focused on the elderly population. Other barriers included expensive and inappropriate equipment, lack of information and knowledge on where and how to exercise and problems with transportation to exercise facilities.
“In fitness centres there is a lack of knowledge on what is possible for people with disabilities, they don’t have time to support you and keep an eye on you.”
Furthermore, people were restrained from purchasing expensive equipment unless they were very sure that it was worth the investment, and second-hand assistive devices and equipment are scarce. In addition, it takes a long time to get the equipment after ordering it. This keeps people from being physically active.
“Purchasing a wheelchair for sports is expensive, and second-hand equipment is scarce. If you think you like a sport, but can’t have a try, or if you can’t pay for expensive equipment, this raises the threshold to even start. Then you really need to be sure you want to do that particular sport, because otherwise it is not worth the investment.”
DISCUSSION
This qualitative study showed that various personal and environmental factors can be a barrier or facilitator to engage in PA for young adults with childhood-onset physical disabilities. PA barriers and facilitators related to attitude and motivation appeared to play a role, which is comparable to the general population (14, 16). Also in adults with other types of physical disabilities, perceiving lower motivational barriers seemed to be important for exercise maintenance, as well as self-efficacy (21). In addition, fatigue, or lack of energy, having injuries or complications associated with the condition, as well as fear of injuries or complications were identified as PA barriers. Lack of information and professional support were also perceived barriers to PA. A study in adults with various types of disabilities also reported lack of information and barriers related to professional knowledge, education and training issues (20).
Rehabilitation professionals can have an important role in promoting PA in people with physical disabilities and in assisting them to overcome the barriers to PA. They can inform patients about the important health benefits of an active lifestyle and on where and how to exercise, and they can facilitate finding the equipment and programmes. They can supervise and assist during exercise and guide patients in finding the right balance between exercise and rest in order to reduce fatigue and prevent injuries. A previous study of van der Ploeg et al. (22, 23) in the Netherlands, showed that a rehabilitation intervention, providing both tailored sports advice and personalized tailored PA counselling, can successfully improve levels of PA of people with acquired physical disabilities in the short- and long-term. However, future studies are warranted to obtain insight into whether such intervention also improves PA levels of young adults with childhood-onset physical disabilities.
Fun or enjoyment was mentioned as a facilitator of PA. Personalized tailored PA counselling offers the opportunity for each person to be supported in finding the type of activity, he or she enjoys, allowing accommodation to the time and finances they have available. In addition to enjoyment, the social environment can also be a facilitator of PA; social contact and social support were mentioned during the focus group sessions. In line with these findings, social support was found to be related to sports participation in adolescents and young adults with MMC (18). For some people, combining social contacts with exercise may therefore be a way to overcome a PA barrier.
Study strengths and limitations
This is the first study reporting on barriers to and facilitators of PA as perceived by young adults with childhood-onset physical disabilities. However, some limitations of the study should be noted. The results are based on a small sample size, which may hamper their generalisability. However, 3 or 4 focus group sessions including 4–12 people are generally considered to be sufficient (24). The third focus group session did not result in much additional information, indicating that the 3 sessions covered the most relevant barriers to and facilitators of PA for young adults with childhood-onset physical disabilities without learning disabilities. Nevertheless, there may have been a selection bias, in that people who are more interested in physical activity and sports, were more likely to participate in the study. This may have resulted in the higher proportion of participating males compared with females. A previous study in adolescents and young adults with MMC showed that males were more likely to participate in sports than females (18).
The advantage of qualitative studies, such as focus groups, is that they are useful to examine the reasons and motives behind people’s behaviours, allowing large amounts of data to be collected in a short period of time (25). However, the methodology did not allow us to determine how many participants perceived a certain barrier or facilitator, or whether there were differences between males and females or other subgroups. Therefore, we cannot draw conclusions on which barriers and facilitators have the largest impact. Nevertheless, the results provide an overview of the main barriers to and facilitators of PA, as perceived by young adults with childhood-onset physical disabilities. Future quantitative studies with simultaneous assessment of PA and personal and environmental factors are warranted to differentiate between the importance of several PA determinants in this population.
In conclusion, young adults with childhood-onset physical disabilities perceived several barriers related to attitude and motivation. In addition, lack of energy, existing injury or fear for developing injuries or complications, limited PA facilities, and lack of information and knowledge appeared to be barriers to PA. Fun, social contacts, social support, and improved health and fitness were mentioned as facilitators. Future interventions to promote PA should take these barriers and facilitators into account.
ACKNOWLEDGEMENTS
This study was supported by Johanna Children’s Fund and Child Fund Adriaanstichting (Arnhem, the Netherlands, grant number 2006/0010 – 063). We thank all participating adolescents and young adults. In addition, we thank Arthur de Grund and Bertran Verweij for their contribution in preparing the focus groups.
REFERENCES