OBJECTIVE: To test the impact of introducing a format based on the International Classification of Functioning Disability and Health, version for children and youth (ICF-CY) as a road-map for in-hospital paediatric neuro-rehabilitation on target definition, intra-team communication and workload as perceived by involved professionals.
DESIGN: Single-centre pilot testing with impact assessment.
Patients: Team members of a tertiary care paediatric neuro-rehabilitation unit included 15 consecutive patients with severe neurological conditions.
METHODS: An ICF-CY based format for rehabilitation projection and programming was constructed and tested for 12 months. The format comprises 3 sections: project, programme, and follow-up. Impact on the rehabilitation team was assessed with a questionnaire.
RESULTS: All cases were described according to their specific needs with appropriate ICF-CY codes, and the interventions were linked to needs and targets. ICF-CY was judged an efficient tool in providing a road-map for rehabilitation in this setting, although concern was voiced about timing and workload.
CONCLUSION: ICF-CY may work as a road-map for in-hospital paediatric neuro-rehabilitation. Its implementation results in perceived improvements in the process. Training requirements and accurate evaluation of timing, workload and organizational context are critical issues that should be addressed before results from the present experience are generalized.
Key words: rehabilitation; WHO; children disability; delivery of healthcare; patient care team.
J Rehabil Med 2010: 42: 49–55
Correspondence address: Andrea Martinuzzi, “E. Medea” Scientific Institute, Conegliano-Pieve di Soligo Research Centre, Via Costa Alta 37, IT-31015 Conegliano, Italy. E-mail: andrea.martinuzzi@cn.lnf.it
Submitted October 27, 2009; accepted August 25, 2009
INTRODUCTION
Interventions in health services are driven by the common goal of improving people’s health, where “health” is intended in its widest and most comprehensive definition, as given by the World Health Organization (WHO): as not only absence of disease, but also complete physical, psychological, and social well-being. The 2 parts of such a definition have their descriptors in the WHO’s International Classification of Diseases (ICD-10) (1), and the International Classification of Functioning, Disability and Health (ICF) (2), both of which are part of the WHO’s Family of International Classifications (WHO-FIC) (www.who.int/classifications). These complementary classifications have the aim of capturing and appropriately describing the health status at the individual and population levels: the first defines health and disease according to aetiology and nosology; the second describes human functioning in terms of body functions and structures, life activities, participation in society, and gives prominence to contextual factors.
In 2007, following a 5-year work by an ad-hoc international team, and after extensive review by the WHO-FIC collaborating centres, WHO presented an ICF adaptation specially designed for children and youth (ICF-CY) (3), acknowledging the peculiar and dynamic nature of many aspects of functioning in children and adolescents. The ICF-CY was then proposed as the common language to describe health and disability in the first two decades of life.
In rehabilitation the emphasis of intervention is rarely on the disease and its treatment, but is almost always on functioning and improvement in well-being. It is therefore understandable that ICF provides the most adequate framework to describe the condition of the persons towards whom rehabilitative efforts are concentrated. Rehabilitation, in the context of health strategy, is defined as a process whose primary goal is to restore functioning, or to optimize it to the highest possible level on the basis of a specific health condition (4). Such a process requires commonly agreed references to describe both the starting condition, with all its weaknesses and strengths, the objectives of the intervention, and the outcomes: outcome research is intended to understand the results of health interventions, in order to improve their utility for patients (5). Chosen references should be recognized and shared by all of the professionals collaborating in multidisciplinary teams, even though they belong to different fields and have different backgrounds, and should be comprehensible to patients and their families. Given these caveats, a framework, if accepted as a common reference, may strengthen the delineation of the rehabilitation process, acting as a road-map. In the rehabilitation process one may recognize the project, aiming at the expected level of functioning for that person foreseen in the long term, and the programme, which will describe the short-term goals, the methodology required to reach them, the timing, and the milestones identified along the process. Such a distinction is also recognized within the Italian laws (6).
ICF can provide the language for structuring both the rehabilitation project and programme, especially for professionals caring for health conditions characterized by problems in multiple areas, that affect persons’ functioning at multiple levels, and require interventions in many sectors, from purely medical to psycho-social, from education to housing.
Children and adolescents with neurological conditions, both acquired or congenital, typically experience problems in multiple functions and structures, are limited in a number of activities, and their participation in society is restricted at many levels Their functioning is heavily influenced by the positive or negative effect of the context, and they are typically in need of both medical and rehabilitation management (7). When dealing with these children any (re)habilitative intervention is naturally complex, articulated and multiprofessional. It must therefore take into consideration all the diverse aspects of functioning, and find a synthetic way in which all the problems are charted in a unified representation that will then serve as an appropriate road-map for action and for evaluating the efficacy of that action by the whole team.
In a tertiary care referral hospital for intensive (re)habilitation of children with complex and severe disabilities, we developed a novel paradigm for rehabilitative project and programme definition based on the ICF-CY, and tested its implementation for 12 months. The introduction of the ICF-CY-based paradigm was expected to act as a shared road-map in the rehabilitation process, providing better targeting and more efficient intervention, and improving information-sharing among team members. ICF would offer an easy to read depiction of the process, clearly linking needs, objectives, methods, and outcome assessment to a sound and scientifically based conceptual model. Worries were voiced about timing and workload, and thus we monitored these items along the test.
The aim of this paper is to present the results of this pilot study testing the impact of the new tool on the multidisciplinary team.
MATERIAL AND METHODS
Design
This is a pilot prospective study in a single centre: a tertiary care referral hospital for paediatric neuro-rehabilitation in the Veneto Region, Italy.
Participants
An ad-hoc work group was constituted within the rehabilitation team. Members of the work group were physicians (neurologist, child neurologist, physiatrist) and rehabilitation professionals (two physico-therapists (PT), one neuropsychologist, (NPS) one social worker, one speech therapist (ST), one occupational therapist (OT), one pedagogist) with a good knowledge of ICF and ICF-CY, having all participated to the basic and advanced training (8) and having acquired at least 3 years of experience in ICF’s clinical use (9). The study then involved all the professionals working with the patients on whom the format was consecutively tested, that is 4 MDs, 3 PTs, 3 NPSs, 2 STs, 2 OTs, 2 pedagogists and one social worker.
Cases
Patients aged 0–18 years consecutively admitted to the unit for severe and complex disabilities undergoing intensive rehabilitation in the period June 2007 to June 2008.
Procedure
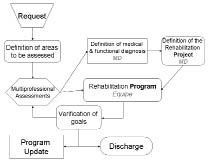
The work group, starting from the analysis of the process (Fig. 1), defined the steps in which ICF-CY structure or formal coding could be introduced and linked to specific steps in the rehabilitation work, and eventually elaborated a structured format in which the rehabilitation project and the rehabilitation programme could be transcribed.
Fig. 1. The process by which the novel project/programme format was introduced.
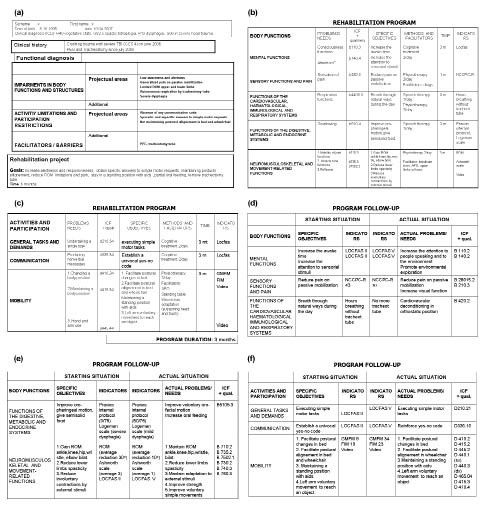
The section describing the project (Fig. 2a) comprised patient’s demographic data, the medical diagnosis according to the ICD (1), a brief anamnesis (open text), and the functional diagnosis, detailed as impairment in body functions and structures and activity limitations/participation restrictions. Functional problems were listed in 2 boxes: the first describing the problems that would be targeted in the rehabilitation work to be performed during the hospital stay; and the second detailing problems which, albeit present, would not be the focus of intervention during hospital admission. A specific box was added for description of facilitators and barriers present and active in the patient’s context. Finally, a box listing the medium-long term goals was included. This section was drafted mainly by the physician responsible for the case, bearing in mind the requests of the patient and his/her family. In this section the use of ICF-CY codes and qualifiers was not requested, but the listing was mapped to the ICF components and, within each component, to the various chapters. Social workers helped to collect information on the context, and involved professionals expressed their opinion. Once each member of the multidisciplinary team has agreed on the assessment and objectives, the rehabilitation project is shared with the patient (if appropriate) and his or her family. The time allotted for project definition was approximately 30 min.
Fig. 2. An exemplificative set of Project and Programme forms. Forms substantiating (a) the project, (b–e) the programme, and (f) follow-up steps. In each form either the various domains of International Classification of Functioning Disability and Health (ICF), or the actual ICF version for children and youth (ICF-CY) codes are embedded and linked to critical steps of the rehabilitation process. FIM: functional independence measure; GMFM: Gross motor function measure; Locfas: level of cognitive functioning assessment; NCCPC: non communicating children’s pain checklist; ROM: range of motion.
The programme (Figs 2b–d) was usually drafted by the fifteenth day of hospital stay, following definition of the project and based upon the mainframe drafted by it. In the programme each professional identified the ICF-CY codes relevant to his or her work, both when they represent a problem (with the appropriate qualifier 1–4) and when they report information on good functioning (with the qualifier 0), set the target of his or her intervention, detailing the methods to be used and the facilitators to be employed and, finally, declared the timing for an assessment of intervention effectiveness. Each team member could use the codes at the definition level that he or she felt most appropriate to describe adequately and precisely the functional profile of the patient. Therefore, we did not limit coding to second-level categories, but first-level as well as fourth- or even fifth-level codes could be used. Linkages to appropriate indicators, possibly expressed through a validated assessment tool (e.g. spasticity b735/Ashworth scale), are required in a dedicated section, and standardized linking procedures were followed (10). The results of scales or assessment tools were operationalized into the generic ICF qualifiers following the indications provided by the American Psychological Association in its guidelines (11), adapting the choice to the type of score resulting from the specific tool. The programme was finalized and harmonized in a team conference (30 min) chaired by the physician responsible for that case, to which all professionals working with that patient participated.
The same format was used for sharing the major intervention goals with family members.
A follow-up form was introduced to be completed at the expiration of the programme time (Figs 2e–2f). The follow-up form is intended to recall the starting situation (containing agreed objectives and appropriate indicators) and to directly compare it with the current and actual situation. In the last columns the remaining problems, described with the appropriate ICF-CY codes and qualifiers, are listed: this opens the possibility of using such information for a new programme form, which would become the starting point of the new phase of rehabilitation.
The family members involved in the reported testing were informed of the ongoing test and gave their informed consent.
Data collection
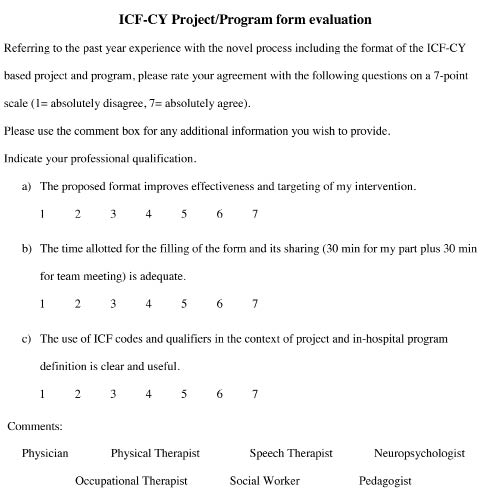
After 12 months of pilot testing, the work group re-evaluated all the completed project/programme forms, and distributed a questionnaire to all involved professionals to gather information on perceived difficulties and positive aspects (Fig. 3). The questionnaire investigated the following dimensions: (i) perceived efficacy and utility of the novel format; (ii) perceived workload in correlation with the time allotted (30 min for each professional involved for filling his portion, plus 20–30 min for the “in-team-meetings” synthesis); and (iii) perceived utility and clarity of the ICF-CY codes use. Responses were recorded on a 7-point scale (1 = absolutely disagree, 7 = absolutely agree). A blank box was left at the bottom of the questionnaire for participants to make relevant comments. The questionnaires were distributed and completed once at the end of the 12-month testing period.
Fig. 3. Text of the final questionnaire for all study participants at the end of the testing period (translation from the Italian original). ICF-CY: International Classification of Functioning Disability and Health version for children and youth.
To objectively track timing and workload, the coordinator of the rehabilitation team was asked to probe the time requested for completing the forms at the beginning of the study, after 6 months and after 12 months,. This was achieved by counting the delays accumulated by each professional in his or her working schedule with res pect to the set time for form filling and team-meetings discussion. The counts were provided by the internally developed institutional administrative software.
Data analysis
Scores of each of the 3 closed questions were averaged and are presented as mean (standard deviation (SD)), while the comments in the open box were analysed qualitatively. Data regarding timing and workload are presented synthetically as frequency of delays.
RESULTS
Fifteen new consecutive cases (7 males, 8 females, median age 9 years, age range 1–15 years) admitted for intensive rehabilitation for complex and severe acquired neurological disabilities were framed with the new format following the flow chart indicated in the diagram (Fig. 1). ICD 10 diagnosis was G80–82 for 10, G93.1 for 3, G04.8 and G05.2 for one each. An example of a completed project/programme/follow-up form (a 12-year-old boy with tetraplegia due to traumatic brain injury) is shown in Fig. 2.
Acceptance by the team members followed an adaptation curve: most of the difficulties and resistance were observed in the first cases, followed by growing confidence with the format and by a decrease in time required for completing all the forms. The first 5 projects/programmes (timing check at 6 months) required the professionals to use the whole allotted time. However, some areas were still not completed adequately, resulting in delays of 10 min or more for at least one team member, while the last 5 cases (timing check at 12 months) were completed and discussed by the whole team in the allotted time.
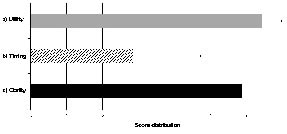
Seventeen questionnaires were returned, all reporting strongly positive judgements at points (i) and (iii), with few internal variability (6.43 (SD 0.53) and 5.86 (SD 1.06), respectively), while responses regarding time allotted and workload (item ii) were more varied (2.85 (SD 1.87)), with most responders reporting difficulties either in keeping up within the assigned time limits, or in accommodating the new assignment in their daily programme (Fig. 4). Analysis of the comment box indicated general appreciation of the opportunity for a stronger convergence on targets and goals, a better concordance with children’s families on the general project, and on the increased inter-professional interaction within a shared conceptual frame and a common language offered by the use of the ICF-CY.
Fig. 4. Distribution of the scores to the closed questions in the questionnaire (a) perceived efficacy and utility; (b) perceived workload in correlation with the time allotted; and (c) perceived utility and clarity of the International Classification of Functioning Disability and Health version for children and youth (ICF-CY) codes. Results are shown as mean (standard deviation) of 17 returned questionnaires.
DISCUSSION
This paper describes the first attempt to implement the new ICF-CY in a clinical setting. This experiment is important for 2 reasons: it represents the first direct clinical utilization of this new classification, testing its efficiency in describing children and adolescents with complex disabilities; and it demonstrates the feasibility of ICF in-hospital implementation, by embedding its conceptual framework in goal definition, process analysis, and outcome evaluation. The setting in which the study was held is a small (40-bed) neuro-rehabilitation unit specifically devoted to children and adolescents, where all professionals were already familiar with team-work, and this might have eased the experience. Nevertheless, the recognition of the added value brought by the implementation of the new ICF-CY-based format, which emerged from the questionnaires, accounts for some difficulties in communication and goal-setting, which the use of ICF-CY helped to overcome.
There have been reports of ICF implementation in clinical settings: the majority of them focussed on the selection of ICF-relevant categories for patients in rehabilitation settings or in acute hospitals (12–14) and on the application of the ICF in rehabilitation settings (15), as well as on the development of ICF Core Sets (16), and the development of ICF-based profiles (Rehabilitation Activity Profile) (17). Verhoef’s study described the effects on team members of the implementation of an ICF-based rehabilitation tool, demonstrating that it improved the perception of cohesion and satisfaction with team conferences.
In the field of developmental disabilities, some studies showed ICF’s utility in the evaluation and description of functional status (9, 18) and in the evaluation of intervention in terms of participation enhancement (19, 20): in the field of language disorders, several papers have been published on the application of the ICF in clinical settings, both in adults and in children (21–29).
The only experience, to our knowledge, describing the ICF application to the whole process of rehabilitation, is the study by Rentsch et al. (30) at Lucerne’s Kantonsspital, in which the ICF was applied for setting rehabilitation goals and for interdisciplinary communication, on the basis of pre-defined selection of ICF categories. This application proved that ICF introduction contributed to an improved quality of interdisciplinary work processes and to a more systematic approach to rehabilitation tasks by team members.
In contrast to the study by Rentsch et al. (30), in which a definite checklist of second- to third-level items was developed starting from basic rasters, recognizing that a fixed list of codes could have resulted in loss of specificity and potential difficulties by the coders, we decided not to limit the number and level of ICF-CY codes. Each professional had the possibility of using the most appropriate set of items to describe the problems in patients’ functioning. This choice encouraged clinicians to enhance the precision of their definitions. This experience demonstrates that the simplification provided by the core-sets or checklists for clinical use, may result in overlooking significant, albeit not necessarily typical, aspects of functioning for that given health condition, and in missing areas of functioning that might be relevant for the single case.
Positive aspects related to this experience emerged from analysis of the questionnaires, and, among them, the strengthening of team cohesion is surely very important. Other aspects relate to improvement in target definition, process ordering for outcome evaluation following a shared conceptual framework. The ability synthetically and neatly to survey changes in patients’ functional profile, and to connect them with treatments, is an important issue, not only to justify the intervention, but also to better orient resources and efforts, especially at the present time, when health professionals are increasingly held accountable for the use of limited resources.
A core element is the possibility of linking the set of assessment tools used by each professional to ICF-CY codes. The rules for such link have been clearly stated and were followed in this study (10). This process launched a revision of the assessment protocols used in our setting in order to optimize the covering of all functional domains, avoiding overlapping and repetitions. In this ongoing activity, the reference to the logical framework of the ICF-CY is of great importance.
Communication across professional jargons is another very critical point achieved through the adoption of the standardized language provided by ICF-CY. This was particularly manifest in those cases requiring the extensive presence of social workers, in particular when communication with teachers is a central issue. The ability readily to recognize terms and definitions eased inter-professional exchanges, effectively reducing the time and effort required. The verification of the inter-rater reliability of concept mapping onto ICF codes by the various team members was not an aim of this study, but considering similar experiences reported by others within much more homogeneous teams (31), this issue deserves future consideration. Our means of implementing the ICF in a rehabilitation setting clearly distinguishes between problems, goals and methods to reach them. A full implementation of such a methodology will define a standardized way to link each aspect to ICF categories. At the same time, the ICF’s descriptive power enables users to find alternative procedures to reach the highest individual level of ability in a specific area: in our opinion, this flexibility is the most immediate positive effect of implementing ICF-based tools in clinical practice.
Finally, the systematic inclusion of environmental factors, both at the project level, where they are listed as acting facilitators or barriers in modulating the person functioning, and at the programme level, where they appear to be linked to the specific domain on which they act as part of the methodology adopted to reach an identified objective, represent an explicit recognition of the importance of context in defining functioning, and of the ecological approach that should characterize any rehabilitative work.
Problems encountered in this study can be categorized as related to training, time and transmission. The experiment was preceded by an extensive training on ICF and ICF-CY following an established format (8), as explained in the methods section. Structured and complete training is a prerequisite for implementing such a kind of ICF-based methodology: in fact clinicians can choose the most adequate set if ICF items only if they have acquired a wide expertise in ICF utilization. All involved professionals attended ICF training, and at least one person for each professional group (physicians, social workers, therapists, teachers, etc.) achieved sufficient proficiency in ICF ad ICF-CY utilization to be appointed as a tutor.
As shown by the results of the questionnaires, time constraint was the main problem recognized by most participants. The most frequent complaint was the lack of time allotted to each professional for completing research forms. However, it should be noted that none of forms arrived at the final team meeting with blank sections. The time allotted was certainly limited, and perhaps more time would have resulted in more accurate and thought-through records; however, we believe that the chosen timing represented a fair balance.
The time required to complete the common parts of the protocol decreased steadily during the experiment, probably due to a learning effect. Ongoing utilization is expected to reduce the time needed and the problems perceived in completing the task. The problem with time, however, also translates into another entity, cost, and, in turn, sustainability. When speaking about cost, all costs, direct and indirect, should be evaluated, which is presently beyond the scope of this work. The total cost of a fully completed form (which may vary according to the number of professionals involved and the complexity of the case) is adequately sustainable, considering the per-diem method of payment adopted by the regional authority. The ratio of the time dedicated to the direct intervention compared with the time dedicated to project/programme definition is more than 10, which is the threshold defined by local authorities. For some paradigmatic cases we calculated a ratio of between 25 and 50, with higher ratios for the more intensive and longer programmes. The amount of time dedicated to programme planning, therefore, is fully sustainable, at least in the present setting. A longitudinal follow-up is now ongoing to monitor workload and resource use, since it may be expected that a more rational programme planning might lead to saving more time and manpower towards similarly satisfactory outcomes. In the study by Rentsch et al. (30), as in ours, time consumption was reported as a problematic issue, but the amount of time required to complete the forms decreased as staff members became familiar with the proposed methodology. The issue of time, however, is always reported when a new procedure is introduced in a team, even when, as in our experience and that of Verhoef et al.‘s (17), several positive effects are also reported.
Data transmission was slow and most of the time restriction was due to Microsoft Word-based tables accessible via protected but shared folders. This not only resulted in a cumbersome data access, but also prevented rapid and filtered data analysis. We are now planning a fully web-based platform linked to the intranet health data system to speed up data transmission procedures. The work completed up to the present will serve as process analysis to implement such an advanced e-tool, which, when fully implemented, should also reduce time consumption.
We recognize that our study has some limitations, mostly linked to the small sample size and to the specificity of the setting in which the experiment took place. While the routine application of the tested procedure is likely to result in a confirmation of the learning curve in the application of the format, and thus in a further reduction in the time required for its compilation, we still cannot draw any definite conclusions about the impact that this new approach will have on children with various diagnosis. Our initial sample is heavily unbalanced towards neuromotor impairments, although some children do have cognitive problems, but none of our patients presented with severe behavioural or psychiatric manifestations. We believe that the inclusion and evaluation of more cases, with different clinical and functional features, will allow the proposed model to be strengthened.
The second critical point refers to the peculiarity of our setting, in which many different professionals are customarily brought to approach the young patients with a common team philosophy, and in which the time and energies needed to implement a new model of work organization is granted within the institutional research activity. An important critique attached to this point can be raised for not including in the experiment the nurses working in the unit. Indeed, while acknowledging the absolute relevance of the area of rehabilitative nursing in the rehabilitation process of our patients, the difficulties at the organizational level related to the identification of a single reference-nurse for each case, pushed us to ask the physician responsible for the case to complete most of the items related to nursing after he had retrieved the information from the nurses. Such a solution, however, will be only transitory, and we foresee as one of the next steps the inclusion of a referent nurse in the programme framing.
The extension of our proposed model will require radical modifications according to the setting to which the experience would be transferred, keeping in mind both the starting conditions of work organization and the setting’s institutional characteristics. It should therefore be underlined that our contribution is, at this stage, more a proof of principle with a practical pilot test than a formalized model ready for direct transferral. While encouraging the test of our proposed model in other settings, we caution that such application should be preceded by an accurate analysis of current institutional processes, in order to provide all required adaptations. The comparison among experiences in different settings will then provide a wide background for a complete and informed discussion on ICF-CY application in the paediatric rehabilitation hospital.
Planned future development of this project comprises 3 major aspects: (i) the establishment of an extended link for the evaluation of protocols in all sectors; (ii) the development of an ICF-CY-based discharge chart (which will allow simplification of transmission of information and improve connections with and between primary healthcare/territorial services); and (iii) the development of an intranet software for easier handling of the whole process.
ACKNOWLEDGEMENTS
We thank the children and their families for participating in this testing, and all the team members for their input. The contribution of Mariamalia Battaglia, MD, in the initial construction of the format prototype is gratefully acknowledged.
The work was funded by Institutional Resources of the Conegliano-Pieve di Soligo Research Centre of the “E. Medea” Research Institute.
REFERENCES