Federico Posteraro, MD1, Stefano Mazzoleni, PhD2, Sara Aliboni, MD3, Benedetta Cesqui, MScME2,4, Alessandro Battaglia, MD3, Maria Chiara Carrozza, PhD2, Paolo Dario, PhD2 and Silvestro Micera, PhD2,5
From the 1Neurological Rehabilitation Unit, Auxilium Vitae Rehabilitation Center, Volterra, 2ARTS Lab, Scuola
Superiore Sant’Anna, Pontedera, 3Rehabilitation Medicine Unit, Versilia Hospital, Lido di Camaiore,
4IMT Institutions, Markets, Technologies Lucca Institute for Advanced Studies, Lucca, Italy and 5Automatic Control Laboratory, Swiss Federal Institute of Technology, Zurich, Switzerland
OBJECTIVE: To compare the effects on spasticity of 2 robot-mediated therapies in patients with chronic hemiparesis.
DESIGN: Groups comparison.
SUBJECTS: Thirty-four patients, divided into 2 homogeneous groups.
METHODS: Outcome measures were: motor status score, Modified Ashworth scale, and range of motion. A pattern of reaching exercises was implemented, in which the direction and length of the movements were modified with the aim of reducing activity of the flexor muscles and improving extension of the arm. A 3-month follow-up was performed.
RESULTS: Statistically significant improvements were found in both groups after treatment. Some differences were found in elbow motor improvement between the 2 groups.
CONCLUSION: Comparison between groups confirms that active movement training does not result in increased hypertonia, but results in spasticity reduction in antagonist muscles by activating the reciprocal inhibition mechanism. Furthermore, robot-mediated therapy contributes to a decrease in motor impairment of the upper limbs in subjects with chronic hemiparesis, resulting in a reduction in shoulder pain.
Key words: upper limb; robot-mediated therapy; rehabilitation.
J Rehabil Med 2010; 42: 279–281
Correspondence address: Federico Posteraro, Neurological Rehabilitation Unit, Auxilium Vitae Rehabilitation Center, Volterra Italy Borgo San Lazzero 5, IT-56048 Volterra, Pisa, Italy. E-mail: f.posteraro@riabilitazione-volterra.it
Submitted December 16, 2008; accepted October 26, 2009
INTRODUCTION
High-intensity and task-specific upper limb therapeutic interventions consisting of active, highly repetitive movements have led to significant improvements in cortical reorganization and motor function in disabled people more than one year after stroke onset (1).
Traditional methods of stroke rehabilitation have some drawbacks: manual intervention by physiotherapists is necessary; and treatments must be provided on a daily basis for several weeks, which makes delivery of a highly intensive treatment for each patient difficult and expensive. Several robotic devices for rehabilitation have been developed in an attempt to avoid these disadvantages (2).
Robot-mediated sensorimotor training and task-oriented repetitive movements can improve muscle strength and movement coordination in patients with neurological impairment (3). An obstacle to using this kind of robotic treatment is the fact that most traditional rehabilitative methodologies aim to reduce and limit spasticity and, in some cases, to delay the execution of active movements. According to these methodologies, active movements involving flexor muscles, such as shoulder adduction, shoulder intra-rotation and, particularly, elbow flexion, can induce an increase in muscle spasticity, resulting in worsening of upper limb motor impairment.
Our hypothesis was that an active-assisted robotic training that does not stimulate flexor patterns (shoulder adduction, shoulder intra-rotation and elbow flexion) and that increases elbow extension may induce different effects on muscle spasticity compared with a robotic training that involves both flexor and extensor upper limb patterns.
In order to examine this hypothesis and evaluate the risk-benefit ratio of stimulating flexor patterns, patients with hemiparesis received 2 different robotic treatments: the first, already used in previous studies (4), allows the use of both flexor and extensor patterns; the second, a new treatment designed and developed by the authors, primarily aims to avoid movements involving the flexor muscles, but to maintain and increase the motor actions involving extension of the arm, particularly at the elbow level.
METHODS
A total of 34 subjects with chronic hemiparesis were included in the study, having had an acute event at least one year previously (mean time from onset of damage 24 months). Inclusion criteria were: unilateral paresis; ability to understand and follow simple instructions; minimum ability to perform active movements, even through trunk compensation, using the shoulder and/or the elbow joints. Exclusion criteria were: flaccid hemiparesis (Chedoke–McMaster Stroke Assessment score = 1) (5, 6); bilateral impairment; severe sensory deficits in the paretic upper limb; cognitive impairment or behavioural dysfunction that would influence the ability to comprehend or participate in the treatment; inability to provide informed consent; and other current severe medical problems. Group A (17 subjects; age range 33–64 years, mean age 51.9 years (standard deviation (SD) 10.7); 7 right hemiparesis, 10 left hemiparesis) was recruited for the robotic therapy used in previous studies. Group B (17 subjects; age range 27–75 years, mean age 52.3 (SD 13.8) years; 6 right hemiparesis, 11 left hemiparesis) were recruited for the new robotic therapy. Robot-mediated therapy was delivered using the MIT-MANUS (Interactive Motion Technologies, Inc., Cambridge, MA, USA), a robot designed for clinical neurological application (4).
Subjects held the end-effector of the robot via a handle; they were seated so that the centre of the range of targets, lying approximately at the centre of their reachable workspace, was aligned with the shoulder in the proximal-distal direction (y-axis). During therapy the subject’s hemiparetic arm was placed in a customized arm support attached to the end-effector of the robot arm. All subjects were asked to perform goal-directed, planar reaching tasks that emphasized shoulder and elbow movements. As they attempted to move the robot’s handle toward designated targets, the robot was able to recognize the active component of movement and allow the patient to perform the movements without assistance. If the patient was unable to reach to the target, the robot supported the patient by driving the end-effector to the target. The computer screen in front of the patient provided visual feedback of the target location and the movement of the robot end-effector.
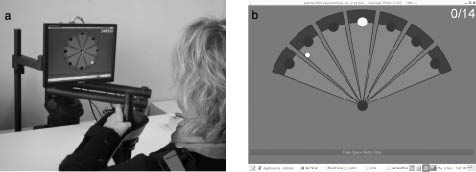
Subjects in group A were asked to perform goal-directed, planar reaching tasks that emphasized shoulder and elbow movements, moving from the central target to peripheral targets (“clock-like” robotic therapy) (Fig. 1a). Subjects in group B were asked to perform tasks using a new technique, named “fan-like” robotic therapy (Fig. 1b). This scenario was implemented in order to reduce stimulation of the flexor pattern, avoiding reinforcement of the pectoralis and biceps muscles. Compared with the “clock-like” therapy, the elbow joint range of motion (ROM) was reduced. Subjects in each group received 3 × 45-min sessions per week of robot-mediated therapy for 6 weeks. Each of the 2 robotic therapies was composed of 2 different kinds of exercises, unassisted (Record) and assisted movements (Adaptive).
Fig. 1. (a) Standard “clock-like” robotic rehabilitative therapy scenario. (b) Innovative “fan-like” robotic therapy rehabilitative scenario.
Each subject’s upper extremity impairment was rated using the Stage of Arm section of the Chedoke–McMaster Stroke Assessment Scale CM-SAS (7) and the Motor Status Scale section for shoulder and elbow (MSS-SE) (8). Spasticity and passive ROM were assessed using the Modified Ashworth Scale (MAS) (9). Elbow active extension was measured by specific Motor Status Scale items. A common condition in neurologically impaired patients is pain in the shoulder joint. The amount of pain in the affected arm was assessed using a 4-point verbal rating scale (0–3, where 0 represents no pain and 3 maximum pain) (10). In order to verify possible qualitative changes in each group (e.g. movement smoothness, impedance by co-activation of antagonist muscles (11)), the minimum jerk deviation, as its mean value for the 3 assisted repetitions, before and after the robotic treatment was determined. Due to the characteristics of the outcome scales (ordinal, but not equally ranged), a non-parametric statistical method, a Wilcoxon signed-rank test was used.
RESULTS
Before starting the therapies, groups A and B were homogeneous. No statistically significant differences were found in CM-SAS, MSS-SE, MAS or ROM. After therapy the results showed a significant decrease in motor impairment in the paretic upper limb in both groups. As shown in Table I, statistically significant improvements were found on the MSS-SE measured before and after robotic treatment in both groups (p < 0.005). The shoulder MAS score decreased significantly after therapy in both groups (p < 0.005). The change in the elbow MAS score after therapy was not statistically significant in either group (p > 0.05).
| Table I. Outcome measures comparison at admission and discharge in groups A and B |
| Evaluation | Stage | Group A | Group B |
| Median | 25% | 75% | p-value | Median | 25% | 75% | p-value |
| MSS-SE | Admission | 12.8 | 10.3 | 14.8 | < 0.001 | 14.6 | 9.8 | 21.0 | < 0.005 |
| | Discharge | 14.2 | 11.9 | 16.6 | | 16.2 | 10.9 | 21.5 | |
| MAS shoulder | Admission | 8.0 | 4.7 | 11.2 | < 0.001 | 5.0 | 1.0 | 7.6 | < 0.005 |
| | Discharge | 4.0 | 2.7 | 6.6 | | 3.0 | 0.7 | 5.6 | |
| MAS elbow | Admission | 1.5 | 0.7 | 2.0 | ns | 1.0 | 0.0 | 1.5 | ns |
| | Discharge | 1.0 | 0.0 | 1.5 | | 0.0 | 0.0 | 1.62 | |
| ROM shoulder | Admission | 440.0 | 408.7 | 566.2 | < 0.001 | 595.0 | 525.0 | 658.7 | < 0.005 |
| | Discharge | 550.0 | 477.5 | 647.5 | | 655.0 | 562.5 | 692.5 | |
| Passive ROM elbow | Admission | 440.0 | 417.5 | 460.0 | < 0.005 | 460.0 | 437.5 | 460.0 | ns |
| | Discharge | 460.0 | 450.0 | 460.0 | | 460.0 | 4475 | 460.0 | |
| Active elbow extension | Admission | 0.8 | 0.6 | 0.8 | ns | 0.8 | 0.0 | 1.1 | <0.005 |
| | Discharge | 0.8 | 0.8 | 1.1 | | 1.0 | 0.6 | 1.8 | |
| ∆MAS elbow group A/group B | Admission | 0.5 | 0.0 | 1.0 | ns | | | | |
| | Discharge | 0.0 | 0.0 | 0.2 | | | | | |
| MAS: Modified Ashworth scale; MSS-SE: Motor Status Scale section for shoulder and elbow; ns: not significant; ROM: range of motion. |
To confirm the absence of differences in the elbow extension MAS score in both groups, changes between groups A and B (∆) were also measured, resulting in no statistically significant differences (∆group A/group B: p > 0.05).
Passive ROM in the shoulder also increased in both groups. For the shoulder, a statistically significant improvement was measured (group A: p < 0.001; group B: p < 0.005). For the elbow, passive ROM and active extension, measured by specific MSS items, were assessed. There was a statistically significant improvement in elbow passive ROM in group A (p < 0.005), but not in group B (p > 0.05).
In contrast, there was no statistically significant improvement in active elbow extension in group A (p > 0.05), whereas in group B active elbow extension showed a statistically significant improvement (p < 0.005).
At admission to the clinical trial, 5 subjects in group A and 8 in group B had shoulder pain. At the end of the robotic therapy, 10 of these had a reduced pain score. No patients reported an increase in pain score. The smoothness of elbow extension movements was measured in both groups through computation of a minimum jerk deviation, as a parameter for stretch reflex evaluation.
No statistically significant difference in the minimum jerk deviation between admission and discharge was found in either group (p > 0.05). No adverse events occurred during the period of study and no patients withdrew from the study. Patients informally reported better use of the impaired upper limb and some also reported an improvement in locomotion.
DISCUSSION
Shoulder MAS and ROM decreased in groups A and B. Elbow MAS did not increase in group A, whose therapy required a major effort of the flexor muscles (biceps) compared with the extensor muscles (triceps), or in group B, whose subjects received reinforcement in the extensor muscles. These results represent a confutation of the hypothesis that the active motor action of spastic muscles might be responsible for increasing the muscular tone (12, 13).
Furthermore, only in subjects from group A, whose therapy was responsible for an increase in elbow joint range, did the passive elbow ROM increase. On the other hand, the active elbow extension movement increased only in subjects from group B, who performed active movements requiring a specific stimulation of the elbow extension muscle.
There are two possible explanations for the above results: (i) the increase in active elbow movement is related only to an increase in muscular strength in the triceps, (ii) the increased activity of the triceps is responsible for a reduction in biceps hypertonia, due to activation of a reciprocal inhibition mechanism. The minimum jerk deviation, which represents a parameter measuring the stretch reflex activation, did not increase in subjects from group B at the end of the robot-mediated therapy. This finding supports the hypothesis that the improvement in active elbow extension involves not only a triceps reinforcement, but also the physiological reciprocal inhibition mechanism, which is responsible for a reduction in biceps spasticity.
In conclusion, active movements are not responsible for an increase in spasticity, at least in chronic patients, but they can contribute to reduced hypertonia in antagonist muscles through activation of a reciprocal inhibition mechanism. Furthermore, taking into account the limitations due to the study design not being a randomized clinical trial, the group outcomes confirm that robot-mediated rehabilitation treatment is able to reduce motor impairment in patients with chronic hemiparesis, and support the hypothesis that the improvement in motor abilities can continue more than one year after the acute event. A reduction in shoulder pain was an additional advantage of the robot-mediated therapy.
ACknowledgements
The present work was partly funded by Fondazione Cassa di Risparmio di Volterra Italy.
REFERENCES