OBJECTIVE: To describe the course of social support in persons with recently acquired spinal cord injury, and to examine direct and indirect relationships between social support and life satisfaction over time.
DESIGN: A multi-centre prospective cohort study with measurements at the start of active rehabilitation, at discharge from inpatient rehabilitation and one year after discharge.
SUBJECTS: One hundred and ninety individuals with spinal cord injury from 8 Dutch rehabilitation centres.
METHODS: Social support was measured with the Social Support List-12. Life satisfaction was measured as the sum score of current life satisfaction and current life satisfaction compared with life satisfaction before spinal cord injury. Distress was operationalized as functional dependence and measured with the Functional Independence Measure. Random coefficient analysis was used for the analyses.
RESULTS: Everyday social support and support in problem situations decreased, and esteem support remained stable over time. Everyday support and support in problem situations were directly associated with life satisfaction over time. Significant interaction effects between social support and distress on life satisfaction were found.
CONCLUSION: Different types of social support showed different courses over time. Social support was associated with life satisfaction after spinal cord injury, in particular in persons with relatively high levels of distress.
Key words: spinal cord injury; rehabilitation; prospective study; social support; life satisfaction.
J Rehabil Med 2010; 42: 265–271
Correspondence address: Marcel Post, Rembrandtkade 10, NL-3583 TM Utrecht, The Netherlands. E-mail: m.post@dehoogstraat.nl
Submitted July 28, 2009; accepted October 26, 2009
INTRODUCTION
Adjusting to the devastating physical and psychosocial consequences of spinal cord injury (SCI) is one of the dominant challenges that persons with SCI are faced with (1, 2). Social support plays an important role in the adjustment process of persons with SCI (3–6). Several studies have reported that more social support is associated with greater life satisfaction (7– 9). Social support can influence life satisfaction in 2 different ways. The first is a direct effect, which is a general effect of social support on life satisfaction, irrespective of the level of distress that a person might experience. The second is an indirect effect, also called a buffer effect, which protects people from potential negative effects in stressful situations (10, 11). In other words, a buffer effect is found when the association between social support and life satisfaction is stronger in stressful circumstances than in less stressful circumstances.
Being dependent on help from other persons is a major stressor (10), especially early after SCI (12). Therefore, the assumption could be made that persons with SCI who are more functionally dependent perceive more distress than persons with SCI who are less functionally dependent (13). In other words, distress is operationalized in the present study as the level of functional dependence.
arlier studies on social support and life satisfaction in persons with SCI did not differentiate between direct and indirect effects of social support (7–9). Moreover, all previous studies had a cross-sectional design, hindering the analysis of the longitudinal relationship between social support and life satisfaction, and the course of social support. Furthermore, most of these studies were conducted several years after the occurrence of SCI (7–9). No studies were found on social support in the early period after SCI.
The first aim of the present study was to describe the course of social support in a cohort of Dutch persons with SCI during inpatient rehabilitation up to one year after discharge. The second aim was to examine direct and indirect relationships between social support and life satisfaction over time. With respect to the second aim, 2 hypotheses were formulated. The first hypothesis is that social support is significantly associated with life satisfaction in persons with SCI over time. The second (buffer) hypothesis is that the association between social support and life satisfaction is significantly stronger in functionally dependent persons with SCI, i.e. those persons who experience more distress, than in functionally independent persons with SCI.
METHODS
Participants
This study is part of the Dutch research programme “physical strain, work capacity, and mechanisms of restoration of mobility in the rehabilitation of persons with spinal cord injuries” (14). For this research programme, persons with a recent SCI who were admitted for initial inpatient rehabilitation were selected consecutively from 8 rehabilitation centres with specialized SCI units in the Netherlands between August 2000 and July 2003. Subjects were included if they fulfilled the following criteria: (i) a recently acquired SCI; (ii) age between 18 and 65 years; (iii) grade A, B, C, or D on the American Spinal Injury Association (ASIA) Impairment Scale (AIS); and (iv) expected permanent wheelchair dependency. In 7 of the 8 rehabilitation centres the reasons why 74 persons did not enrol into the study were specified: 22 persons were excluded because they had an SCI due to a malignant tumour or progressive disease, 16 persons had psychiatric problems, 10 persons had insufficient comprehension of the Dutch language to understand the goal of the study and test instructions, and 26 persons refused to collaborate.
Approval of the research protocol was obtained by the medical ethics committee of the SRL/iRv Hoensbroeck. All subjects gave written informed consent.
Procedure
Three measurements from the research programme were relevant for the present study. The first was at the start of active rehabilitation (defined as the moment that a person could sit for 3–4 h) (T1), the second at discharge from inpatient rehabilitation (T2), and the third one year after discharge (T3). The measurements comprised, among others, a medical anamnesis, an oral interview with a trained research assistant and a self-report questionnaire. Questions about social support and life satisfaction were part of the oral interview.
Instruments
Social support was operationalized as the subjective appraisal of received social support by the recipients themselves and was measured with the Social Support List (SSL-12). This is a reliable and valid short version of the Social Support List–Interactions, assessing the extent of perceived received social support by means of social interactions with members of the primary social network (15). The SSL-12 consists of 12 items on 3 scales, with possible item scores ranging from 1 (seldom or never) to 4 (very often). The 3 scales are “everyday social support” (referring to social companionship and daily emotional support), “support in problem situations” (referring to instrumental, informational support, and emotional support in times of trouble), and “esteem support” (referring to support resulting in self-esteem and approval).
Life satisfaction was measured with 2 questions. The first question was: people can be more or less satisfied with their life as a whole, their so-called “quality of life”. What is your quality of life at the moment? This question was scored on a 6-point scale: very unsatisfying (1) up to very satisfying (6). The second question was: if you compare your life now with your life shortly before the SCI, is your quality of life at the moment worse, equal or better than before the SCI? Possible response scores were: much worse (1) up to much better (7). Supported by strong correlations (0.5–0.6) between both questions at each measurement, a total life satisfaction score was computed by summing the 2 individual scores on both questions, leading to a total score of between 2 and 13. This total score was normally distributed (Skewness 0.0–0.5) at each measurement (16).
Level of functional dependence was the proxy measure of distress and was measured with the motor score of the Functional Independence Measure (FIMTM) (17). The motor score of the FIMTM consists of 13 items about self-care, mobility, transfers, and toileting and has a total score of between 13 and 91. A low FIM motor score indicates functional dependence and a high level of distress.
Demographic characteristics taken into account were age, gender, educational level (higher education vs high school or less), marital status (married or living at parental home vs living alone), and whether the participant had children.
Lesion characteristics were assessed according to the International Standards for Neurological Classification of Spinal Cord (18). Neurological lesion level was defined as the highest motor level. Neurological levels below T1 were defined as paraplegia, neurological levels at or above T1 were defined as tetraplegia. AIS grades A and B were considered motor complete, and grades C and D were considered motor incomplete.
Statistical analyses
Only persons who completed at least 2 measurements were included in the analyses.
Descriptive statistics of participants’ characteristics, functional dependence, social support, and life satisfaction were calculated for each measurement. Demographic and lesion characteristics of persons who completed all 3 measurements were compared with persons who only completed 2 measurements, using χ2 tests. Spearman correlations were used to investigate correlations between life satisfaction, functional dependence, and social support at each measurement time-point.
To study the course of social support up to one year after inpatient rehabilitation, random coefficient analysis (multi-level analysis) was used. The advantage of random coefficient analysis in longitudinal studies is that the number of observations per person and the temporal spacing of these observations can be varied. Furthermore, this method considers dependency of repeated measures within the same person by using random intercepts and, in this study, corrects for possible differences between rehabilitation centres and persons by allowing random slopes in regression coefficients (19). The course of social support was studied with time as the only determinant, entered in the model as a set of 2 dummy variables with discharge from inpatient rehabilitation (T2) as reference. Four different models were calculated to study the course of social support: 1 model with total social support as the dependent variable and 3 models with each a single subscale of social support as the dependent variable.
The relationships between social support and life satisfaction were analysed with 4 different multi-level linear regression models, one model for each type of social support and total support, with in the basic model life satisfaction (T1, T2, and T3) as the dependent variable, and the social support variable (also T1, T2, and T3) as the independent variable (to analyse the direct relationship). To analyse the indirect relationship between social support and life satisfaction, the FIMTM score, and the interaction term between the social support variable and the FIMTM score were added to the basic model. The demographic and lesion characteristics were added one by one to the model to test whether they were confounders. The characteristics were considered confounders if the Beta values of the above independent variables or interactions changed more than 10% after adding them to the model.
SPSS statistical program for Windows (version 16.0) and the MLwiN program of the Centre for Multi-level Modelling of the Institute of Education in London (version 1.1) were used for the analyses. Significance was set at a p-value less than 0.05.
RESULTS
Respondent characteristics
At the start of active rehabilitation (T1) 225 persons with SCI were included in the study, 198 participated at discharge from inpatient rehabilitation (T2), and 156 performed the tests one year after discharge (T3). A total of 190 persons completed at least 2 measurements on social support and life satisfaction and were included in the analyses. Reasons for drop-out over time varied: death (11), regained ability to walk longer distances (12), refusal to collaborate (24), unreachable (5), removal (5), organizational problems (9), and serious psychological problems (3). A comparison between participants and non-participants at the T3 measurement showed no differences regarding demographic characteristics and completeness of injury. However, more non-participants than participants had a tetraplegia.
The mean age of the participants at the start of active rehabilitation was 40.6 years (standard deviation (SD) 14.1), and the median time between injury and start of active rehabilitation was 75 days (range 7–371 days). There were more male than female participants, and the majority had a traumatic injury, a complete paraplegia, a spouse and children (Table I).
| Table I. Characteristics of respondents (n = 190 at start of active rehabilitation) |
| Characteristics | n (%) |
| Gender | |
| Male | 142 (74.7) |
| Female | 48 (25.3) |
| Cause of injury | |
| Traumatic | 143 (75.3) |
| Non-traumatic | 47 (24.7) |
| Type of injury | |
| Incomplete paraplegia | 35 (18.4) |
| Complete paraplegia | 85 (44.7) |
| Incomplete tetraplegia | 22 (11.6) |
| Complete tetraplegia | 47 (24.7) |
| Unknown | 1 (0.5) |
| Marital status | |
| Living with a spouse | 107 (56.3) |
| Living at parental home | 36 (18.9) |
| Living alone | 47 (24.7) |
| Children | |
| Yes | 96 (50.5) |
| No | 94 (49.5) |
| Education | |
| Higher education | 87 (45.8) |
| High school or less | 102 (53.7) |
| Unknown | 1 (0.5) |
| Age, years | |
| 18–34 | 75 (39.5) |
| 35–49 | 58 (30.5) |
| 50–65 | 56 (29.5) |
| Unknown | 1 (0.5) |
Descriptives and correlations between life satisfaction, social support, and functional dependence
Table II shows descriptives of total social support, the 3 subscales of social support, life satisfaction, and functional dependence at each measurement time-point.
| Table II. Descriptives of social support, life satisfaction and the functional independence measure score at each measurement (median, interquartile range) |
| Domain | Maximum range | Actual range | Admission (n = 190) | Discharge (n = 187) | After 1 year (n = 147) |
| Total support | 12–48 | 14–48 | 36.0 (31–40) | 34.0 (31–38) | 33.0 (28–36) |
| Everyday social support | 4–16 | 4–16 | 12.0 (11–14) | 12.0 (11–14) | 12.0 (11–13) |
| Support in problem situations | 4–16 | 4–16 | 12.0 (10–14) | 11.0 (9–13) | 10.0 (8–12) |
| Esteem support | 4–16 | 4–16 | 11.0 (9–13) | 11.0 (9–13) | 11.0 (9–12) |
| Life satisfaction | 2–13 | 2–13 | 5.0 (3–7) | 7.0 (5–8) | 7.0 (5–8) |
| Functional dependence | 13–91 | 13–90 | 36.0 (28–51) | 74.0 (47–79) | 74.0 (43–80) |
There were significant Spearman correlations (range 0.34–0.64; p < 0.01) among the 3 subscales of social support at each measurement. Furthermore, significant correlations existed between life satisfaction and functional independence at each of the 3 measurements (0.36, 0.31 and 0.32; p < 0.01). There were no significant correlations between the 3 subscales of social support and total social support on the one hand, and life satisfaction and functional independence on the other hand. The only exception was a weak but significant correlation between esteem support and life satisfaction at T1 (0.15; p = 0.04).
Course of social support
Random coefficient analysis showed that total social support and everyday social support remained stable during inpatient rehabilitation, but decreased after discharge from inpatient rehabilitation (Table III). Support in problem situations decreased during and after inpatient rehabilitation, and esteem support remained stable during and after inpatient rehabilitation.
| Table III. Multi-level linear regression models for the course of social support during initial inpatient rehabilitation up to one year after discharge (n = 190) |
| Variables | Model for
total social support | Model for
everyday social support | Model for support
in problem situations | Model for
esteem support |
| Beta | SE | p | Beta | SE | p | Beta | SE | p | Beta | SE | p |
| Constant | 34.690 | 0.436 | | 12.346 | 0.149 | | 11.209 | 0.196 | | 11.128 | 0.179 | |
| Time (T2–T1) | 0.755 | 0.420 | 0.072 | –0.029 | 0.141 | 0.837 | 0.820 | 0.203 | 0.000* | –0.031 | 0.175 | 0.859 |
| Time (T3–T2) | –1.955 | 0.459 | 0.000* | –0.447 | 0.179 | 0.013* | –1.149 | 0.221 | 0.000* | –0.356 | 0.191 | 0.062 |
| *Statistically significant at p < 0.05. Note 1: Beta stands for a non-standardized regression coefficient in multi-level analyses. Note 2: All 4 models had random intercepts. Note 3: All time-dependent covariates had a fixed slope, except for Time (T3–T2) in the model for everyday social support, which had a random slope. T1: start of active rehabilitation; T2: discharge from inpatient rehabilitation; T3: 1 year after discharge from inpatient rehabilitation; SE: standard error. |
Direct and indirect relationships between social support and life satisfaction
Table IV shows that total social support and esteem support were not directly related to life satisfaction over time. Everyday social support and support in problem situations, on the other hand, were directly related to life satisfaction over time. Everyday social support was positively associated with life satisfaction, and support in problem situations was negatively associated with life satisfaction.
| Table IV. Multi-level linear regression models for the direct relationship between different types of social support and life satisfaction (n = 190) |
| Variables | Model for
total social support | Model for
everyday social support | Model for support
in problem situations | Model for
esteem support |
| Beta | SE | p | Beta | SE | p | Beta | SE | p | Beta | SE | p |
| Constant | 6.367 | 0.916 | | 5.224 | 0.833 | | 7.170 | 0.413 | | 5.709 | 0.723 | |
| Soc S. variable | 0.005 | 0.018 | 0.781 | 0.108 | 0.050 | 0.031* | –0.091 | 0.035 | 0.009* | 0.080 | 0.044 | 0.069 |
| Confounders |
| Age | –0.012 | 0.011 | 0.275 | –0.491 | 0.243 | 0.043* | n.e. | n.e. | n.e. | –0.003 | 0.011 | 0.785 |
| Completeness | –0.493 | 0.244 | 0.043* | –0.002 | 0.011 | 0.856 | n.e. | n.e. | n.e. | –0.476 | 0.243 | 0.050 |
| Lesion | 0.964 | 0.272 | 0.000* | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. |
| Cause of injury | –0.299 | 0.364 | 0.411 | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. |
| *Statistically significant at p < 0.05. Note 1: Beta stands for a non-standardized regression co-efficient in multi-level analyses. Note 2: All 4 models had random intercepts. Note 3: All time-dependent covariates had a fixed slope. n.e.: not entered; SE: standard error; Soc. S. variable: social support variable. |
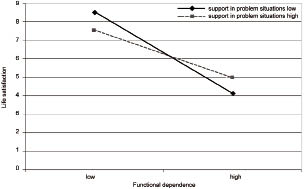
Table V shows that no significant interaction effects occurred between total social support and functional dependence, and between everyday social support and functional dependence. There was, however, a significant interaction effect between support in problem situations and functional dependence. Fig. 1 shows that the difference in life satisfaction between functionally dependent and functionally independent persons with SCI was larger for the group who experienced low levels of support in problem situations than for the group who experienced high levels of support in problem situations.
| Table V. Multi-level linear regression models for the indirect relationship between different types of social support and life satisfaction (n = 190) |
| Variables | Model for
total social support | Model for
everyday social support | Model for support
in problem situations | Model for
esteem support |
| Beta | SE | p | Beta | SE | p | Beta | SE | p | Beta | SE | p |
| Constant | 2.045 | 1.344 | | 3.276 | 1.420 | | 3.140 | 1.044 | | 1.851 | 1.114 | |
| Soc S. variable | 0.062 | 0.035 | 0.076 | 0.073 | 0.107 | 0.495 | 0.096 | 0.076 | 0.207 | 0.212 | 0.089 | 0.017* |
| FIMTM | 0.074 | 0.020 | 0.000* | 0.041 | 0.022 | 0.062 | 0.065 | 0.015 | 0.000* | 0.072 | 0.017 | 0.000* |
| Soc S. × FIMTM | –0.001 | 0.001 | 0.317 | 0.000 | 0.002 | 1 | –0.002 | 0.001 | 0.046* | –0.003 | 0.001 | 0.003* |
| Confounders |
| Age | –0.004 | 0.010 | 0.689 | –0.003 | 0.010 | 0.764 | –0.006 | 0.010 | 0.549 | –0.003 | 0.010 | 0.764 |
| Completeness | –0.071 | 0.228 | 0.755 | –0.074 | 0.228 | 0.797 | –0.079 | 0.230 | 0.731 | –0.098 | 0.227 | 0.666 |
| Lesion | n.e. | n.e. | n.e. | n.e. | n.e. | n.e. | 0.181 | 0.276 | 0.512 | n.e. | n.e. | n.e. |
| *Statistically significant at p < 0.05. Note 1: Beta stands for a non-standardized regression co-efficient in multi-level analyses. Note 2: All 4 models had random intercepts. Note 3: All time-dependent covariates had a fixed slope. FIM: Functional Independence Measure; n.e.: not entered; SE: standard error; Soc. S. variable: social support variable. |
Fig. 1. Indirect (buffer) relationship between support in problem situations and life satisfaction over time. Low and high are the extremes of the actual range on the Functional Independence Measure (FIMTM) score and the support in problem situations scale: Low functional dependence = a score of 90 on the FIMTM. High functional dependence = a score of 13 on the FIMTM; Low support in problem situations = a score of 4 on the support in problem situations scale; High support in problem situations = a score of 16 on the support in problem situations scale; For the confounders 40.6 was filled in for age (mean age), one for completeness (complete lesion), and one for lesion (paraplegia).
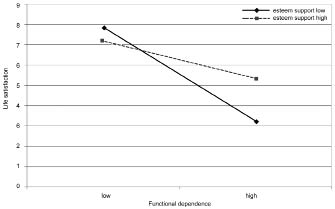
Furthermore, there was a significant interaction effect between esteem support and functional dependence. Fig. 2 shows that the difference in life satisfaction between functionally dependent and functionally independent persons with SCI was larger for the group who experienced low levels of esteem support than for the group who experienced high levels of esteem support.
Fig. 2. Indirect (buffer) relationship between esteem support and life satisfaction over time. Low and high are the extremes of the actual range on the Functional Independence Measure (FIMTM) score and the esteem support scale. Low functional dependence = a score of 90 on the FIMTM; High functional dependence = a score of 13 on the FIMTM; Low esteem support = a score of 4 on the esteem support scale; High esteem support = a score of 16 on the esteem support scale; For the confounders 40.6 was filled in for age (mean age), one for completeness (complete lesion), and one for lesion (paraplegia).
DISCUSSION
This is the first reported study to describe the course of social support and the direct and indirect relationships between social support and life satisfaction early after SCI. A decrease in social support during inpatient rehabilitation and in the first year after discharge from inpatient rehabilitation was found. The 2 hypotheses about the relationships between social support and life satisfaction were partly confirmed: everyday social support and support in problem situations were directly associated with life satisfaction over time, and the associations between support in problem situations and, respectively, esteem support and life satisfaction were stronger in functionally dependent persons with SCI than in functionally independent persons with SCI.
The 3 different types of social support followed a different course early after SCI. Everyday social support and support in problem situations were both high at the start of active rehabilitation, but decreased over time, with a steeper decrease for problem support than for everyday social support. Esteem support remained high during and after inpatient rehabilitation. These results correspond to the study of McColl et al. (20), who stated that in the first stage of a stressful event, emphasis was placed on emotional and problem-oriented support, but that over time, stronger emphasis was placed on emotional support than on problem-oriented support.
The decrease in social support can be considered negative, based on findings from other studies that more social support is related to better outcomes (7–9). However, it is also possible that a decrease in social support over time reflects the adjustment process in persons with SCI. One year after discharge from inpatient rehabilitation, social support levels in the present study were still higher than support levels in the general (elderly) population (15). This finding contrasts with earlier studies, which demonstrated that support levels in people with SCI approximate support levels in the general population over time (20). At present, data are collected 5 years after discharge from inpatient rehabilitation in the same cohort of persons with SCI. These data will make it possible to examine whether social support levels in persons with chronic SCI in the long run indeed approximate support levels in the general population.
In the literature on social support, there is no consensus between authors about the existence of a buffer effect of social support (10, 11). We found evidence for both a general (direct) effect and a buffer (indirect) effect of social support on life satisfaction. Everyday social support and support in problem situations showed a direct association with life satisfaction over time. Everyday social support was positively associated with life satisfaction, and support in problem situations was negatively associated with life satisfaction. Other studies also found a positive association between emotion-oriented support and life satisfaction, and a negative association between problem-oriented support and life satisfaction (8, 21). A possible explanation for the negative association between problem-oriented support and life satisfaction is that problem-oriented support can be regarded as unwanted advice, or as a confront persons with SCI with the fact that they are dependent on others (20, 21).
However, a buffer effect was also found, as support in problem situations and esteem support were more strongly associated with life satisfaction in functionally dependent persons with SCI than in functionally independent persons with SCI. Many researchers believe that emotional support is the strongest stress buffer, although this is not investigated thoroughly (21). We showed that, next to emotional support, problem-oriented support also moderated the impact of distress on life satisfaction in persons with SCI.
In the present study, functionally dependent persons with SCI were compared with functionally independent persons with SCI, and it was assumed that low levels of functional dependence reflected low levels of distress. The significant buffer effects that were found illustrate the relevance of this approach. It is possible that even stronger direct or buffer effects would have been present if levels of distress of persons with SCI were compared with a control group without disabilities, but further study is needed to examine this hypothesis.
By focusing on the perceived received social support and making a distinction between 3 types of social support, it was clearly defined what was measured with respect to social support in this study. Often a clear definition of social support is lacking in studies on social support (22). Moreover, the longitudinal design with a time-span starting at active inpatient rehabilitation up to one year after discharge from inpatient rehabilitation made it possible to study the relationships between social support and life satisfaction during and after inpatient rehabilitation. Furthermore, the methodology that was chosen was powerful for finding a possible buffer effect. We tried to overcome problems in methodology and conceptualization described by Cohen (10) and Thoits (11) by using a large sample, a longitudinal design and instruments with acceptable psychometric characteristics. Also, a clear conceptualization of social support was given, and it was examined whether there was a significant relation between distress and life satisfaction, and no or little correlation between the social support and distress measures.
The somewhat larger drop-out of persons with tetraplegia may have resulted in an overestimation of life satisfaction after SCI and may have influenced the relationship between social support and life satisfaction (23). Furthermore, in the results, we did not make a distinction between patients with a traumatic and a non-traumatic lesion because we focused on the whole SCI population instead of focusing on subgroups within the SCI population. Earlier publications based on our cohort showed that cause of injury (traumatic/non-traumatic) was not a predictor for life satisfaction (16). Another limitation was that the level of distress was only measured as functional dependence. A recommendation for future research would be also to focus on other sources of distress in persons with SCI. For example, distress as a result of bodily functions such as pain and other secondary complications, or as a result of social conditions such as being unemployed. Furthermore, although psychometric properties of the SSL-12 were satisfactory (15), no earlier studies were executed that used the SSL-12 in persons with SCI. This made a comparison between the present study and other studies on social support and SCI somewhat more difficult. Moreover, the SSL-12 measures perceived received support, which is only one of the main constructs of social support, next to social networks and supportive behaviour (24). A final limitation of the present study was that the questions only covered support received from friends or family. Support from professionals was not taken into consideration.
The present study has shown that social support is important for life satisfaction of persons with SCI in the early phase of the injury. Sufficient attention must be paid to different types of social support during and after inpatient rehabilitation. Professionals should pay extra attention to functionally dependent persons with SCI who receive little social support. These persons might be at risk for poor adjustment.
ACKNOWLEDGEMENTS
The authors would like to thank the participating Dutch rehabilitation centres, and the research assistants in these centres who collected all data: Rehabilitation Centre De Hoogstraat (Utrecht), Rehabilitation Centre Amsterdam, Rehabilitation Centre Het Roessingh (Enschede), Rehabilitation Centre Hoensbroeck (Adelante), Rehabilitation Centre Sint Maartenskliniek (Nijmegen), Rehabilitation Centre Beatrixoord (Haren), Rehabilitation Centre Heliomare (Wijk aan Zee), and Rehabilitation Centre Rijndam (Rotterdam).
REFERENCES