OBJECTIVE: To measure the effect of intensive therapy and the lasting effect of a standardized functional training programme with vs. without the addition of chemodernervation of the muscles of the forearm and hand.
Patients and methods: Twenty children with spastic hemiplegia, aged 4–16 years, were matched for baseline characteristics and randomized to standardized task-oriented therapy for 6 months with or without botulinum toxin injections. Dynamic kinematic outcome measures were: speed, accuracy, end-point spread and performance. Measurements of active and passive range of motion, stretch-restricted angle of the elbow and wrist, Ashworth scores and Melbourne Assessment of Unilateral Upper Limb Function were made. All measures were performed at baseline, 2 weeks after injection of botulinum toxin and after 6 months (at the end of therapy), and 3 months after end of the therapy.
RESULTS: Clinical measures showed improvement in both groups. However, no significant differences emerged between groups on functional measures. Directly after the botulinum toxin injection all kinematic outcome measures showed a decrease, but baseline values were re-established during the therapy period. After botulinum toxin injections a temporarily significant greater increase in speed and performance was found. These results illustrate the need for further quantitative research into the effects of botulinum toxin.
Key words: cerebral palsy; kinematic aiming tasks; spasticity; upper limb; task-oriented therapy; botulinum toxin-A; randomized clinical trial.
J Rehabil Med 2010; 42: 332–338
Correspondence address: Eugene Rameckers, Motor Control, KU Leuven, Strabeek 30, NL-6301 HS Valkenburg, The Netherlands. E-mail: eaa.rameckers@hetnet.nl
Submitted April 7, 2009; accepted November 30, 2009
INTRODUCTION
Children with spastic hemiplegia encounter many problems in performing manual tasks (1). Research in the last decade has lead to a better picture of the movement characteristics of the affected upper limb (2–5). Compared with typically developing children, children with spastic hemiplegia have slower upper limb movements, and an increased number of sub-movements, combined with excessive trunk movements (2–5). Furthermore, they also have decreased scores in manual performance tests, such as the Jebsen Taylor test (6), Melbourne Assessment of Unilateral Upper Limb (MA) (7) and Quality of Upper Extremity Skills Test (QUEST) (8, 9).
An important question arises; namely, what are the underlying causes of this deficit?
The primary motor cortex is crucially involved in execution of movement of the fingers and is often damaged in hemiparesis (10). This most often results in spasticity and pareses (11–14). If spasticity is the major factor eliciting such impairments then 2 questions are important; whether spasticity can be decreased by intervention and, if so, whether this will lead to positive changes in hand function.
A common intervention used to treat spasticity is injections with botulinum toxin-A (BoNT-A) (15). BoNT-A has a paralysing effect on the injected muscles and blocks the release of acetylcholine in the synapses of the motor units for the coordination of the muscles. BoNT-A decreases spasticity and muscle strength in the injected muscles and increases the active range of motion of the antagonists (15–17). Current evidence does not allow any conclusion to be drawn about the positive or negative effect of BoNT-A on manual function (18–21). This lack of consistency illustrates the need for more rigorous quantitative tasks (19–21).
Using isometric wrist flexor force tasks we have shown that the wrist flexor force decreased immediately after BoNT-A injection and increased slightly at the end of therapy (22).
It may be argued that some of these quantitative tests do not sufficiently represent activities of daily living (ADL). Therefore, in parallel, we used a kinematic aiming task (KAT) as a quantitative and reliable way to assess changes in arm movements. It was found that, directly after BoNT-A injection, the accuracy and speed of movements in such aiming tasks were reduced (16).
A first rationale for the current study was to expand these tasks so as to mimic more closely the activities normally performed by these children. Three different kinematic aiming tasks were developed; a discrete lift task, a discrete shift task and an alternating shift task. All 3 tasks represent different aspects of movements occurring in ADL, such as writing, lifting a small object and placing an object.
In the discrete lift and shift tasks the movements have to be made with start and stop signals for each movement. These tasks are chosen to test the ability to accelerate and slow down the object, guided by visual information, which is essential in order to carry out these tasks accurately (23). Compared with the shift tasks, the load on muscle strength in proximal arm muscles in the lift task is higher, because the whole arm has to be lifted from the surface. In the alternating task fast movements had to be made between 2 targets. Controlled activation and release of agonist and antagonist muscles are required to perform this task well (4, 5, 23).
For evaluation purposes it is obligatory that the data from kinematic recordings have small measurement error in order to be able to detect change over time (16). Such objective and clinical essential data are provided by parameters such as accuracy and movement speed. Both are important elements determining the performance in a goal-directed task. This speed accuracy trade-off is expressed in a mathematical relationship in Fitts Law (24). Importantly, Fitts Law can be used to equate the performance of the motor system by combining the speed and accuracy in a single outcome measure, the Index of Performance Effective (IP-E) (3).
The present study examined the effect of standardized therapy (PT/OT) and BoNT-A on the changes in accuracy and movement speed.
After BoNT-A injection, it is assumed that muscle tone and co-contraction decreased (15). If so, this may allow faster movement towards an object. This effect is predicted to be most obvious in the alternating aiming tasks, because such tasks have a robust advantage in speed accuracy trade-off over discrete tasks. Smits Engelsman et al. (3) found that movement speed was higher in cyclical alternating movements. This was based on incorporated stretch-shortening cycles. The muscles can generate more force after stretch and benefit from the energy stored in the elastic tissue, which is released during muscle shortening. This will enable movement with greater speed (3). In contrast, a discrete aiming task may have an advantage with respect to accuracy because attention can be focused on the homing-in phase, when the target is nearly reached. Hence, accuracy will be most important in the discrete aiming tasks and these are therefore likely to be performed at lower speed.
A second rationale for the present study was that there is a need to evaluate the long-term effects of BoNT-A. An earlier study showed that directly after BoNT-A the accuracy and speed of movements were reduced in KAT tasks (16), but it is not known what the long-term effects are on this type of tests. In the present study we are interested in the effect on speed and accuracy after a long period of PT/OT with (BTX+ group) or without (PT/OT group) additional BoNT-A. The present study took place over a period of 6 months therapy, with 3 months follow-up after the therapy period. A randomized design was used with 2 groups.
The aims of the study were: (i) to evaluate whether spasticity and range of motion correlate with movement time and accuracy at baseline; (ii) to evaluate the effect of intensive therapy on movement time and accuracy in aiming tasks compared with baseline; and (iii) to evaluate the additive effect of BoNT-A and intensive therapy on movement time and accuracy in aiming tasks.
METHODS
Participants
Twenty children with cerebral palsy (CP) participated in this study, age range 4–16 years, mean age 9.5 years. They were diagnosed with spastic hemiplegia according to the Hagberg classification (25) and were classified based on the severity of the hand function using the Zancolli classification (pattern of hand function impairment, pattern I, IIa, IIb) (26). Exclusion criteria were: children with a cognitive level below 3 years, with Zancolli III and movement limitation of wrist or elbow extension of more than 30º. An overview of the baseline and follow-up characteristics of the participants is given in Table I. A specific PT/OT programme adapted to each Zancolli level was developed. The current data were collected in conjunction with the study of Speth et al. (17). The parents gave informed consent and the study was approved by the medical ethics committee of the Rehabilitation Foundation Limburg.
| Table I. Changes in Angle of Catch, Active Range of Motion, and Passive Range of Motion of the wrist and elbow, and Melbourne Assessment (MA) scores over both groups during the period of therapy and follow-up |
| Clinical data | Both groups (n = 20) |
| Baseline Mean (SD) | Therapy period Mean (SD) | Follow-up MEan (SD) |
| Angle of Catch wrist (°) | 57.7 (21.1) | 69.9* (17.5) | 70.7 (15.6) |
| Angle of Catch elbow (°) | 136.7 (36) | 158.7* (29.8) | 167.5 (21.7) |
| Active dorsal flexion wrist (°) | –3.7 (37) | 22.7* (31) | 16.5 (34.1) |
| Active extension elbow (°) | 165.5 (15.5) | 172.5* (13.1) | 175 (8.5) |
| Passive dorsal flexion wrist (°) | 72.5 (12.4) | 74.7 (12.9) | 74.5 (14) |
| Passive extension elbow (°) | 176.2 (13.1) | 177.7 (7.8) | 178.7 (5.8) |
| Melbourne Assessment (%) | 64 (10) | 67 (9.9) | 66.6 (11.9) |
| p < 0.05. |
Design
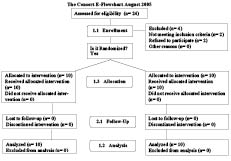
Ten pairs of children were formed after matching according to age and Zancolli level (I and II). A BTX+ group and PT/OT group were formed after random allocation within each pair. Randomization was performed by computer. Only one of the pairs had different Zancolli levels (I, II). Outcome measures were collected at baseline (2 weeks before BoNT-A), 2 weeks after BoNT-A, and at 3, 6 and 9 months after the start of therapy. The PT/OT group was tested in the same weeks as the BTX+ group. No children were lost to follow-up (Fig. 1).
Fig 1. The CONSORT flow-chart
Therapy programme and splinting
The specific therapy programme was standardized and task-oriented. Training of skills (27) and strength (28) was performed within task-specific activities, based on the individual demands and specific goals of each child. A thermoplastic night splint was used to improve passive range of motion (PROM) – the elbow extended, a neutral forearm, 20º extension of the wrist and thumb in abduction. For the participants graded Zancolli IIB a cock-up splint (wrist in 20º extension) was made, which they wore during the day. The duration of the therapy was 30 minutes of physical and occupational therapy each, 3 times a week, over a period of 6 months. The therapy was supervised by experienced therapists.
Injection technique and dosage
Botox® (Allergan, Irvine, USA) was used (dilution 5 U/0.1 ml). Dosage was 2–3 U/kg bodyweight in the upper arm, 1–2 U/kg bodyweight in the forearm, with a maximum of 50 units at any one site, with an overall maximum dose of 400 U/kg total bodyweight (17). Predominantly the m. adductor pollicis (10 U), the m. flexor carpi ulnaris (2 × 20–2 × 40 U) and the m. pronator teres (30–50 U) were injected and less frequent injections were given in the m. flexor carpi radialis (30–2 × 30 U), m. biceps brachialis (2 × 20–2 × 50 U), m. brachioradialis (40–2 × 40 U) and m. flexor pollicis brevis (5 U), as described in the study of Speth et al. (17). The number of units per total bodyweight ranged from 2.9 to 5.8 U.
Outcome measures
Experimental outcome measures. In the 3 KAT tasks, the children held a digital pen embedded in a custom-made puppet (length 7 cm, diameter 2.5 cm) in their affected hand. They could directly see their movements. Movements were made on a digitizer (Wacom, type Cintiq 18sx, sample rate 206 Hz, KIKO software, Doetinchem, The Netherlands). This digitizer was also a SXGA full 24-bit colour LCD monitor and was placed directly in front of the participant (Fig. 2). The glass surface of the monitor made the shifting movement easy.
Fig. 2. Experimental set-up with a digitizer as colour LCD monitor. The tablet is placed directly in front of the participant. The digital pen is embedded in a “puppet” of 2.5 × 7 cm.
Three tasks were performed, a discrete visually-guided tapping task (lift task), a discrete visually-guided shift task (shift task) and an alternating visually guided shift task (alternating task). Oasis software (KIKO software) was used to program the 3 tasks (29). Movements were made over a distance of 20 cm and to a target with the same diameter as the puppet (2.5 cm).
The goal for the children in these aiming tasks was to get the puppet in the target circle (2.5 cm diameter) while performing a substantial arm movement (20 cm). After putting the puppet on the digitizer in the starting circle on the left side the investigator pressed the start button. After a random period (between 0.5 and 1.5 s) a tone sounded and the other target appeared on the right side of the digitizer, 20 cm from the target on the left side. This was the “go” signal for the child, who was then required to move as fast and as accurately as possible to the target.
In the lift task the puppet had to be lifted and land on the target that had appeared. In the shift task the puppet had to be shifted. If the puppet landed on the target and was kept stationary (if speed was below 0.2 cm/s) a new starting sound was given and the puppet had to be moved to the other side. The total number of movements was restricted to 10 per trial.
In the alternating task a start signal was given and over a period of 20 s the puppet had to be shifted between both targets as often as possible with the highest accuracy. After 20 seconds a stop signal was given.
The tasks were presented in the same order to all the children; namely, lift, shift, and alternating task. This was done because random order led to too many mistakes in performance. After a practice session for all tasks the experiment began.
Signal analysis. Spatial accuracy was calculated in 2 ways: first using the dichotomy between the correct and incorrect responses (Proportion Successful Movements; PSM); secondly, as the distance of the centre of the puppet to the centre of the target (End-point Spread; END, mm). Movement Time (MT, seconds) per segment was calculated as a temporal variable. The MT started when a puppet was lifted/shifted and ended when the speed of the puppet in the target dropped below 0.2 cm/s in the target. The IP-E (bits/s) was calculated, expressing the relationship between movement speed and accuracy in goal-directed movements (37). In formula format the definition is: IP-E = a + b*Log2 (2A/ ETW) /MT (where a and b are empirical constants, A = distance between targets, ETW = effective target width, and MT = movement time). The ETW is calculated as the distance between the centre of the target and the centre of the puppet.
Outcome measures for spasticity and mobility. Spasticity was measured with the Ashworth Scale (AS) and the Stretch-Restricted Angle (SRA) for the extension of the wrist and elbow (30–31). Spasticity was measured in the supine position. The SRA was assessed by moving the wrist and elbow as fast as possible (within 1 second) through the whole range of motion (31).
Mobility was registered by measuring the active and passive range of motion (AROM and PROM) of the wrist and elbow extension while the participant was in the sitting position. Standardized goniometry (MIE, Medical Research Ltd clinical goniometry) was used to measure SRA, AROM and PROM (32).
Manual ability of the affected hand was measured with the Melbourne Unilateral Upper Limb Assessment, because of the reliability and validity for unilateral upper limb function in children with spasticity in the studied age group (7). MA was scored from video recordings, after encoding and randomization (children and occasions of measurements). Trained movement scientists (double-blinded) scored the videos.
The clinical outcome measures have been reported earlier (22) and were used in the study to evaluate whether spasticity, and range of motion showed a correlation with movement time and accuracy at baseline and after the end of therapy.
Statistics
KAT task outcome measures. The dependent variables PSM, END, MT and IP-E were evaluated by means of the General Linear Model (Polynomial), Repeated Measures design, with group (2) and session (5) as between-subject variables, and task (3) as within-subject variable. Post-hoc analyses were used, if appropriate, to further analyse: (i) baseline and 6 months (to measure the effect of therapy); (ii) baseline and 9 months (to measure the long-term effect); and (iii) 6 vs. 9 months (to measure the lasting effect after the end of therapy).
Spearman’s rank correlation was calculated to examine whether the outcome measures, AROM, PROM, SRA and AS, correlated with MT, END, and IP-E at baseline and at the end of the therapy period. The alpha level was set at 0.05.
χ2 statistics were used to look for differences between groups at baseline.
RESULTS
All participants completed the therapy and the measurement programme. There was no loss to follow-up. There were no statistical differences between the groups at baseline.
Outcome measures for spasticity, mobility and manual ability
The results of the clinical tests after the intervention have been described in a previous publication on the same group of participants (22). Since these findings are essential to compare with the present experimental data the results are summarized briefly in Table I, showing the significant changes. In summary, measured over all children, AROM and SRA of the wrist increased and Ashworth scores decreased. For both groups combined, a significant increase in AROM and SRA of the wrist was found at the end of the therapy period. Furthermore, a significant decrease in Ashworth scores of the wrist and elbow were found at the end of the therapy period. The percentile scores of the MA did not show any significant improvement on any of the test occasions. Importantly, no significant differences were found between groups.
Experimental outcome measures
Overall. A significant main effect of task was found for all the outcome measures (MT F(2,36) = 8.07, p = 0.001; PSM F(2,36) = 2.6, p = 0.008; IP-E F(2,36) = 8.55, p = 0.001), indicating that the 3 tasks tested different elements of the aiming task. No main effect was found for session. However, a significant interaction effect of task and session was shown for each outcome measure (MT F(8,144) = 14.47, p < 0.001; PSM F(8,144) = 23.28, p < 0.001; END F(8,144) = 6.25, p < 0.001; IP-E F(8,144) = 18.65, p < 0.001), indicating that session resulted in different effects on the underlying mechanisms measured with the tasks. Only significant interactions of task, session and group were found for MT (F(8,144) = 4.21, p = 0.04) and for IP-E (F(4,188) = 5.34, p = 0.03), indicating that the groups performed differently over time on the tasks related to MT and IP-E (Figs 3–6).
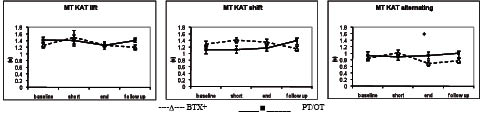
Movement time. As seen in Fig. 3 the PT/OT group showed very similar performance at the end of the therapy in the shift task (from 1.1 (0.07) to 1.2 s (0.09)), and in the alternating task (from 0.9 (0.12) to 0.95 s (0.1)). On the other hand, a minor decrease in MT was found in the lift task from 1.4 (0.09) to 1.2 s (0.06), meaning that they moved slightly faster. The BTX+ group showed a small decrease both in the lift task (from 1.4 (0.09) to 1.2 s (0.07)), and in the shift task (from 1.4 (0.1) to 1.3 s (0.1)), whereas a clear decrease in MT was found in the alternating task (from 1 (0.08) to 0.7 s (0.07)), indicating a positive influence of the added BoNT-A in fast alternating movement tasks. Post-hoc analysis of the period baseline and the end of the therapy showed a significant interaction of tasks by session by groups (F (2,36) = 3.76, p = 0.03). This is caused mainly by the larger difference in MT between both groups in the alternating task at the end of therapy. This effect was diminished 3 months after the end of therapy.
Fig. 3. Movement Time in all 3 kinematic aiming tasks (KAT). Measurement at baseline, after 2 weeks (short), at the end of the therapy period (end) and 3 months after the end of therapy (follow-up). Error bars are ± 1 standard error of mean. *Significant at post-hoc testing. BTX: intervention group with botulinum toxin, PT/ OT; intervention group without botulinum toxin.
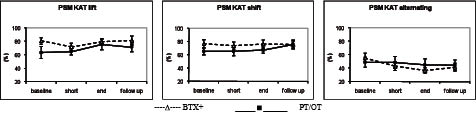
Accuracy (percentage successful movements (PSM) and end-point spread (END)). Both PSM as END did not show effects of group, and there were no interactions with task or session. In Fig. 4 it is shown that at the end of therapy in the lift task both groups improved their PSM. In contrast, in the shift task they did not improve. In the alternating task both groups showed a decrease in PSM, indicating that in these fast movements the accuracy was not improved in either group.
Fig. 4. Proportion Successful Movements in all 3 kinematic aiming tasks (KAT). Measurement at baseline, after 2 weeks (short), at the end of the therapy period (end) and 3 months after the end of therapy (follow-up). Error bars are ± 1 standard error of mean. BTX: intervention group with botulinum toxin, PT/ OT; intervention group without botulinum toxin.
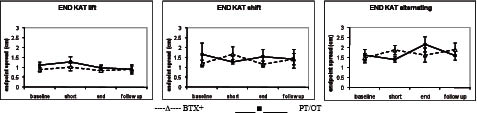
END. As illustrated in Fig. 5, the spread of end-points showed a non-significant small decrease in the lift and shift tasks for both groups at the end of therapy. In the alternating task both groups showed a non-significant small increase in END, indicating that neither group could improve their accuracy if speed is involved, despite intensive intervention.
Fig. 5. Endpoint Spread in all 3 kinematic aiming tasks (KAT). Measurement at baseline, after 2 weeks (short), at the end of the therapy period (end) and 3 months after the end of therapy (follow-up). Error bars are ± 1 standard error of mean. BTX: intervention group with botulinum toxin, PT/ OT; intervention group without botulinum toxin.
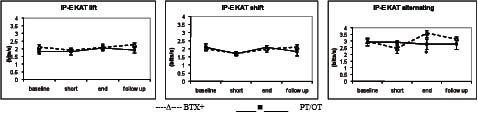
Index of Performance Effective. Both MT and END are essential elements of performance in the aiming tasks, and influence each other negatively. We therefore used the IP-E as a measure capturing the 2 elements and correcting for the speed accuracy trade-off (24). Analysis of the period baseline and the end of therapy showed a significant interaction of tasks by session by groups (F (2,36) = 2.85, p = 0.01). This is caused mainly by the difference in performance in the alternating task. As illustrated in Fig. 6 for the alternating task, a clear increase was found in IP-E for the BTX+ group, from 2.9 (0.2) to 3.6 bits/s (0.4) and a small increase was found for the PT/OT group at the end of the therapy, from 2.9 (0.2) to 3.1 bits/s (0.3). In the lift task only a slight improvement in IP-E was seen for the PT/OT group at the end of therapy, from 1.8 (0.1) to 2.1 bits/s (0.1), whereas the BTX+ group showed no differences (from 2.1 (0.1) to 2.1 bits/s (0.1)). In the shift task the PT/OT and BTX+ groups performed comparably and showed equal scores at baseline and at the end of therapy.
Fig. 6. Index of Performance Effective (IP-E) in all 3 kinematic aiming tasks (KAT). Measurement at baseline, after 2 weeks (short), at the end of the therapy period (end) and 3 months after the end of therapy (follow-up). Error bars are ± 1 standard error of mean. *Significant at post-hoc testing. BTX: intervention group with botulinum toxin, PT/ OT; intervention group without botulinum toxin.
Hence the only gain was seen in the alternating task and this gain was more beneficial for the BTX+ group. IP-E decreased after the end of therapy in the alternating task in both groups (to 3.1 bits/s (0.2) in the BTX+ group and to 2.8 bits/s (0.2) in the PT/OT group), indicating that 3 months after the end of therapy the gain in therapy was diminished.
Correlation between clinical and experimental outcome variables
As seen in Table II a significant correlation at baseline was present for AROM of the wrist with IP-E in the lift task (rho 0.67) (p = 0.001). In all tasks AROM of the wrist had a significant negative correlation with the accuracy parameter END, most probably indicating that active wrist mobility is important for accurate task performance. At baseline there was a significant positive correlation of Ashworth score of the wrist with MT in the lift task (rho 0.49) (p = 0.02) and a negative correlation of Ashworth score with IP-E (rho –0.52) (p = 0.02) in the alternating task, indicating that if high flexor tone of the wrist is present, movements are slow and IP-E will be low in an accuracy task if either speed or lifting an object is important.
| Table II. Correlation of Movement Time (MT), Proportion Successful Movements (PSM), Endpoint Spread (END) and Index of Performance Effective (IP-E) with the clinical measures (AOC, Active Range of Motion, Passive Range of Motion, Ashworth Score (AS) and Melbourne Assessment) at baseline. Only significant correlations are presented. (Alpha was set at 0.05) |
| | MT | PSM | END | IP-E |
| Lift task | | | | |
| Active dorsal flexion wrist (°) | –0.46 (0.02) | | –0.89 (0.00) | 0.67 (0.001) |
| Ashworth score wrist | 0.49 (0.02) | | | –0.52 (0.02) |
| Melbourne Assessment (%) | | | | 0.53 (0.01) |
| Shift task | |
| Active dorsal flexion wrist (°) | | | –0.68 (0.00) | |
| Ashworth score elbow | | 0.51 (0.01) | | |
| Melbourne Assessment (%) | | | –0.63 (0.00) | |
| Alternating task | |
| Active dorsal flexion wrist (°) | | | –0.81 (0.000) | |
| Ashworth score wrist | 0.58 (0.007) | | | –0.58 (0.006) |
| Melbourne Assessment (%) | | | –0.65 (0.00) | |
A significant negative correlation was found for MA with END in the shift task (rho –0.63) (p < 0.01) and with END in the alternating task (rho –0.65) (p < 0.001) and a significant positive correlation with IP-E in the lift task (rho 0.53) (p = 0.01), indicating that if the ability to perform movements accurately is high, MA scores will also be high.
DISCUSSION
Standardized therapy was performed in this randomized controlled study (RCT) over a 6-month period. The standardized therapy was based on task-oriented training, strength training and the use of splints. Half of the group received additional BoNT-A. For both the PT/OT and BTX+ groups this resulted in a clinically relevant increase in AROM of the wrist and elbow. In addition the scores on the Ashworth Scale decreased. The decrease in spasticity and increase in AROM are mentioned in most of the studies in the 3 week period after BoNT-A, indicating a tone-reducing effect of BoNT-A (17–22).
The crucial question is how these changes affect functional manual ability and whether it is possible to identify tasks in which such ability is improved. The present study shows that even when global assessments of manual ability fail to show improvement one can quantify improvement in very specific subtasks.
For the global assessment the MA test was used. Both groups showed a small non-significant increase in MA scores of 3 percentiles, which is less than the smallest detectable difference (8.9 percentile for the Melbourne Assessment) (33). This is in coherence with all review studies on BoNT-A and treatment of the upper limb, also showing no clear improvement in functional clinical measures (19–21). Furthermore in a prospective longitudinal study of 2 years duration, Satila et al. (34) concluded that the reduction in muscle tone after BoNT-A treatment did not translate into better gripping or quality of fine motor functions (Melbourne Assessment) of the affected hand.
The MA assesses many aspects of motor control, however, and it is possible that more detailed analysis is needed to reveal functionally important changes in manual ability. To identify such subtle changes a battery of 3 simple tests was used and performance was evaluated in terms of parameters of speed (MT), accuracy (PSM and END) and their combination (IP-E). In the alternating task the IP-E of the PT/OT group showed a small increase at the end of the therapy period and the BTX+ group improved significantly more. This increase was related to a significant decrease in MT while accuracy measures were unchanged (or even showed a non-significant decrease). Hence the PT/OT group moved more slowly and somewhat more accurately. This resulted in a benefit to the BTX+ group regarding IP-E. In the alternating task a fast alternating contraction and release of forearm muscles (wrist and elbow) is needed to perform this task adequately (35). The children have to master the degrees of freedom of the musculoskeletal system to control these fast alternating goal-directed movements (36–37). The tone-reducing effect of BoNT-A seems to facilitate the programming and execution of these movements with higher speed, resulting in improved IP-E for the BTX+ group.
While the changes in the alternating task were the only significant ones between groups, it is worthwhile considering some smaller tendencies seen in the other tasks. In this study we found the greatest increase in accuracy (expressed in PSM and END) in the lift task for both groups and a very small increase in the shift task when performance at end therapy was compared with baseline. There are several possible explanations for these positive findings. First, in the task-oriented therapy, mainly grip and lift tasks are practised, so they improved on what was trained (lift). Secondly, the selective improvement in the lift task may be related to the lift task being easier than the shift phase because homing-in is easier. In the shift task, the homing-in has to be controlled by slowing down gradually while this is not the case for the lift task where deceleration is relatively easy because of the impact on the surface at landing (acting to break the movement).
Study limitations
The study did not include either a control group without intensive therapy or a placebo group, thus we have to be cautious when generalizing our conclusions with regard to usual or no care.
Conclusion
We can conclude that intensive functional therapy with and without BoNT-A decreased spasticity and increased AROM of the wrist for both groups, with a slight non-significant benefit for the BTX+ group. Kinematic outcome measures show a larger and significant benefit for the BTX+ group for speed and performance in the alternating tasks. This increase is based on the gain in movement speed but relative loss of accuracy. In contrast, performance in the alternating task for the PT/OT group did not show this benefit. More generally, it can be concluded that adequate AROM of the wrist is required successfully to perform discrete movement tasks, while a decrease in spasticity is needed to perform fast alternating tasks.
REFERENCES