OBJECTIVE: To examine the state of, and change in, biopsychosocial health and quality of life of patients after whiplash injury, before and after an inpatient interdisciplinary pain management programme.
METHODS: Observational, prospective cohort study (n = 103) using medical record data and standardized self-assessments to compare health state with general population norms and to determine effects by means of standardized effect sizes. The therapy programme consisted of drug adaptation, graded activity exercise, relaxation therapies, and behavioural therapy.
RESULTS: Compared with population norms, patients’ health was significantly deteriorated in all dimensions of the Short Form 36, depression and anxiety at all examined times. After rehabilitation, pain improved by effect sizes up to 0.65, function/role performance up to 0.87, vitality up to 0.67 and coping up to 0.41. At the 6-month follow-up, these effects remained, with effect sizes between 0.45 and 0.87. The median working capacity improved from 8 h per week at baseline to 21 h at follow-ups.
CONCLUSION: The rehabilitation programme showed moderate to large mid-term improvements in important health dimensions, medication reduction and working capacity. Further controlled studies are required to quantify and attribute these improvements more precisely.
Key words: whiplash injury; outcome; interdisciplinary; rehabilitation; instruments.
J Rehabil Med 2010; 42: 350–356
Correspondence address: Felix Angst, Schiedhaldenstrasse 1, CH-8700 Küsnacht, Switzerland. E-mail: fangst@vtxmail.ch
Submitted May 26, 2009; accepted December 16, 2009
Introduction
Chronic neck pain and associated symptoms after whiplash injury cause severe individual burdens of disease and high costs for the healthcare system of middle European countries, USA and Australia. Whiplash injury has been estimated to have a point prevalence of 2% in the Swedish general population (1). The annual incidence has been estimated at 300/100,000 in Sweden and Germany (2, 3). Approximately 50% of persons with whiplash injury report neck pain one year after the accident (3). Once whiplash is chronic, treatment effects and recovery rates are small, and high levels of disability and compensation are frequent consequences (2, 4, 5).
In Switzerland, 10,000 new cases of whiplash injuries due to car accidents are reported annually, corresponding to an annual incidence of 130/100,000 (6). Approximately 10% of affected people develop a chronic course (7). Cervical spine injuries have been reported for every third car accident, which has led to a case for third party insurance (7). Whiplash injuries demand 50% of the costs paid by third party injuries for car accidents, i.e. 300 million euro per year (6, 7).
Mental health and psychosocial abilities play an increasing role in the course of whiplash (2, 4, 8). Compared with passive treatment modalities, active management modalities, e.g. muscle training, educational advice and teaching and practising of adaptive pain coping strategies, are more effective, especially in multidisciplinary settings (9–14). The effectiveness of multidisciplinary rehabilitation for neck and shoulder pain was considered to be of little scientific evidence compared with other rehabilitation methods in a review of 1808 abstracts and 65 reviews; only 2 studies were selected (15).
However, an interdisciplinary programme for 2 whiplash injury cohorts, including ergonomics, physical therapy modalities and exercise therapy, education and psychotherapeutic modalities, showed only a few and small improvements (5). Another outpatient programme consisting mainly of physical training therapies suffered from a high drop-out rate (almost 50%), with only 26 participants remaining, resulting in data of questionable validity (16). Both studies were conducted in the late 1990s. The rationale for our study was to examine the effects observed after a modern intensive inpatient pain programme focusing on improvement in pain coping performance, with intention-to treat analysis, and holistic standardized outcome assessment.
This study aimed to describe and examine state (compared with normative population data) and change in biopsychosocial health, health-related quality of life and pain coping performance of patients after whiplash injury (with chronic neck pain) before and after an inpatient interdisciplinary pain management programme.
Material and methods
Patients
Patients were consecutively referred by general practitioners, rheumatologists, neurologists, case managers of accident insurance companies, and hospitals to a specific inpatient, interdisciplinary neck pain management programme called Zurzacher Interdisziplinäres HWS Konzept (ZIHKo). Comprehensive rating of the patients and their situation focused on the following characteristics, as described by the Swiss multidisciplinary consensus group (17): whether the condition did not improve or worsened under/despite therapy, whether anxiety, depression or maladaptive coping played an increasing role, and whether patients did not (partially) return to work.
Patients were screened for admission to the programme in 3 steps: first, diagnostic screening was performed by the head of the programme (FG) or one of the other experienced neuropsychologists according to predefined conditions based on the admission report. These conditions based on consensus and described in the inclusion and exclusion criteria (see below) fulfilled the criteria of the Swiss multidisciplinary consensus group as stated above (17). The assessment of the inclusion and exclusion criteria was instructed for the members of the neuropsychologists’ team in order to be able to carry out the criteria by each neuropsychologist. Secondly, the neuropsychologist contacted potential candidates by telephone to evaluate the inclusion and exclusion criteria listed below. Thirdly, approximately 5% of the candidates interviewed by telephone visited the clinic for a 1 h consultation to clarify any uncertainties concerning the first or second screening steps.
Inclusion criteria for the study were: (i) chronic neck pain of minimum 3 months and maximum 5 years duration caused by whiplash injury (after 5 years many are jobless); (ii) first-time accident causing whiplash injury (re-injuries were excluded); (iii) history of failed or insufficient efficacy of outpatient treatment and/or signs of risk for chronic course post-injury; (iv) no inpatient rehabilitation for whiplash-associated disorders in the past; (v) age between 17 and 65 years; (vi) willingness to participate to the whole rehabilitation programme and the assessment by written informed consent; (vii) sufficient cognitive abilities and German language skills to understand the content of the interventions.
Exclusion criteria were: (i) severe somatic illness requiring specific treatment, such as cancer, inflammatory rheumatic disease, spinal fracture, neurological disease, and pain after a recent operation; (ii) manifest psychiatric disorder, such as severe depression, suicidality, psychosis, personality disorder, dementia; and (iii) failed inclusion criteria. “Severe” was defined as when the disorder prevented participation in the therapies. The study protocol was approved by the independent local ethics commission (Health Department in Aarau, Switzerland, EK AG 2008/026). Written, signed informed consent was obtained from all participants. From 2004 to 2008 (sampling period: 5 years), 252 consecutively admitted patients participated in the 4-week rehabilitation programme. The inclusion criteria were met by 185 persons (Fig. 1). All 67 excluded patients participated in the rehabilitation programme without any restriction. All patients had a Quebec Task Force grade II (neck pain and musculoskeletal findings) syndrome.
Fig. 1. Patient selection in the study.
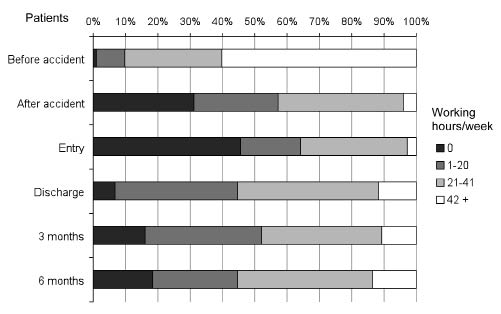
Fig. 2. Working status during the course of treatment.
Intervention
The present interdisciplinary therapy concept was based on experience with our parallel interdisciplinary management programme for chronic pain (8). The therapeutic modalities of our present programme for whiplash patients are listed in Table I. The clinic stay lasts 4 weeks and nursing service for the patients is available 24 h/day. The therapy programme is based on a biopsychosocial model, the concept of salutogenesis, and the integration of various psychotherapeutic concepts and methods (14).
| Table I. Characteristics and therapy components of the interdisciplinary rehabilitation programme for patients with whiplash injury |
| Intervention | Duration: h/week |
| Physician: examination in first week examination in last week | 1 0.5 |
| Physician: visit | 0.75 |
| Information about pain (group) | 0.75 |
| Physiotherapy: individual (mainly exercise therapy) | 2.5 |
| Physiotherapy: group (strengthening and endurance training) | 3 |
| Strength and endurance training (non-supervised) | Optional |
| Aquatic exercise group | Optional |
| Physiotherapy: relaxation therapy | 3 |
| Occupational therapy: group individual | 3 2 |
| Tai chi/Qigong | 3 |
| Psychology: pain information and coping group | 2–3 |
| Psychology: cognitive behavioural therapy individual | 2–4 |
| Psychology: music therapy and painting therapy (group) | 2–3 |
| Interdisciplinary meetings for 5–6 patients | 1.5 |
It addresses the medical, personal and psychosocial complexity of patients with chronic pain disorders and has been adapted to chronic whiplash syndrome. The programme aims to stop the process of pain chronification, to increase resilience, to correct and improve maladaptive coping behaviour, and to improve health-related quality of life (14, 17). Psychosocial elements can amplify and aggravate benign somatic symptoms to produce a severe, disabling chronic syndrome, and a minor injury can be turned into a serious life event (8). The event of the accident has to be overcome, processed and coped with. The role of accident victim that leads to passive maladaptation must be turned into an active role of personal responsibility. This was performed by neuropsychological therapies and occupational therapies to assess and increase psycho-intellectual resilience.
Specific therapeutic strategies were mainly included in the pain management programme if their outcomes had been published in peer-reviewed journals, for example, graded activity exercises and cognitive behavioural therapy for chronic back and neck pain (8–12). Creative therapies are also, but somewhat less, examined (18). Every participant received all therapy modalities listed in Table I (standardized programme). Active therapies, i.e. exercise therapies, were individual strengthening exercises, mainly on exercise machines, and aerobic exercise on standing bike, treadmill, Nordic walking, and individually tailored home exercises (Table I). The only passive therapy was individual massage.
In the psychotherapy modules, patients relearned a structured time frame for the activities of daily routine and work. Balanced phases of activity and relaxation were taught. Patterns of thinking and behaving were revised and optimized. Psychosocial stress factors were identified and strategies developed to manage the stress factors. Psychosocial problems and psychiatric disorders were treated by individual psychotherapy and psychoactive drugs. In most cases, subsequent management programmes were organized for the period immediately after hospital dismissal, especially home exercise and advice about physiotherapy and psychotherapy in cooperation with the physician and the physiotherapists who continue the patient’s management.
The interdisciplinary pain management team consisted of specialists such as clinical neuropsychologists, physicians, physiotherapists, occupational therapists, Qi Gong instructors, creative therapists (painting therapy, music therapy). All the healthcare professionals involved were experienced in their speciality: the mean duration of working experience on-the-job (time after diploma for current profession) was 15 years and the mean time of participation in the rehabilitation programme was 5 years. Additionally, they had completed additional postgraduate standardized educational training in the theoretical, conceptual and therapeutic aspects of interdisciplinary pain management during employment in our clinic by repetitive, regular seminars and courses. The main aim was to qualify them successfully to treat chronic pain, concomitant vegetative symptoms, and maladaptive patterns of coping after accidents. Clinical supervision and, if necessary, case-specific instructions during the course of treatment were provided by an experienced neuropsychologist (FG).
Measures
Sociodemographic data were collected using the same standardized questionnaire as in several previous studies, including questions about working capacity before the accident and after returning home. Medical records provided additional information about physical and mental comorbidities (any comorbidities, no predefined list), medication, and working capacity. Specific observed comorbidities were anaemia, obesity, osteoarthritis, complications after various fractures, periarthropaties, fibromyalgia, low back pain, reflux disease, gastritis, cardiovascular diseases, hypertension, metabolic diseases (mainly diabetes mellitus and hypothyreosis), depression, anxiety, and allergies.
Biopsychosocial health and quality of life was assessed comprehensively by the Short Form 36 (SF-36), the most widely used self-administered generic health-related quality of life instrument. We administered the validated German version to ask about symptoms and functioning during the preceding 4 weeks (19, 20). The SF-36 has been implemented in numerous studies in over 50 languages worldwide and its clinimetric quality has been proven in various settings. Normative data that allow stratification by sex, age (5-year intervals) and comorbidity (none vs at least 1) were obtained from a German population survey (n = 6948) (21).
Cervical spine-specific pain, function and neurogenic (neurological) symptoms were quantified using the North American Spine Society (NASS) cervical spine self-assessment instrument (22, 23). Neck pain is assessed by 2 items (suffering from pain, and disabled by pain), functional limitation due to neck pain by 8 items (dressing, lifting, walking, sitting, standing, sleeping, social life and leisure, and travelling), and neurogenic symptoms by 8 items suffering from: pain in the arm, numbness or tingling in the arm/hand, weakness in the arm/hand; disabled by: pain in the arm, numbness or tingling in the arm/hand, weakness in the arm/hand; when walking: stiffness in the legs, trembling in the legs The aggregate score of pain and function was determined in accordance with the original description of the instrument (24). Pain and function were also analysed on 2 separate subscales because of their very different constructs, which were empirically separated by factor analysis in chronic back pain (24). To our knowledge, population-based data are not available.
Affective health, specifically depression and anxiety were self-rated on the Hospital Anxiety and Depression Scale (HADS) (25, 26). The questionnaire was specifically designed for non-psychiatric settings and has been thoroughly tested in large populations and patient surveys (27). Sex- and age-specific (10-year intervals) norms are available from a German population survey (n = 2037) (27).
Cognitive and behavioural strategies to tolerate, manage and compensate for pain were quantified using the Coping Strategies Questionnaire (CSQ). We used an abbreviated version of the German CSQ consisting of the scales “increasing activity”, “praying and hoping” (only 3 items of hoping: “hoping”), “catastrophizing”, “ability to control pain”, and “ability to decrease pain” since these are the most responsive scales in chronic pain (28–30).
An overview of all scores is presented (see Table III) and some examples of the item contents of the scales are cited at the beginning of the discussion.
| Table III. Course of whiplash injury patients on self-assessments (n = 103) |
| | Norm Mean | Entry Mean (SD) | Discharge | 3 months | 6 months |
| Mean (SD) | ES | p | Mean (SD) | ES | p | Mean (SD) | ES | p |
| SF-36 | Physical functioning | 87.3 | 55.7 (18.3) | 68.3 (17.4) | 0.69 | < 0.001 | 69.2 (17.5) | 0.74 | < 0.001 | 70.5 (18.9) | 0.81 | < 0.001 |
| | Role physical | 81.8 | 5.8 (15.3) | 19.2 (26.0) | 0.87 | < 0.001 | 15.4 (27.7) | 0.63 | < 0.001 | 19.2 (32.1) | 0.87 | < 0.001 |
| | Bodily pain | 62.9 | 21.4 (14.3) | 30.7 (15.0) | 0.65 | < 0.001 | 29.9 (18.2) | 0.59 | < 0.001 | 30.4 (20.9) | 0.63 | < 0.001 |
| | General health | 66.5 | 49.4 (16.1) | 51.6 (16.8) | 0.14 | 0.134 | 49.7 (19.0) | 0.02 | 0.712 | 49.6 (18.5) | 0.01 | 0.939 |
| | Vitality | 56.3 | 27.3 (15.9) | 38.0 (17.1) | 0.67 | < 0.001 | 34.6 (19.0) | 0.46 | 0.001 | 35.7 (20.9) | 0.53 | < 0.001 |
| | Social functioning | 83.9 | 45.3 (25.8) | 49.9 (25.0) | 0.18 | 0.074 | 47.5 (26.6) | 0.09 | 0.592 | 50.7 (25.9) | 0.21 | 0.118 |
| | Role emotional | 86.6 | 44.0 (45.1) | 46.6 (43.2) | 0.06 | 0.520 | 49.3 (42.0) | 0.12 | 0.304 | 47.3 (45.6) | 0.07 | 0.421 |
| | Mental health | 69.2 | 52.5 (19.8) | 61.4 (17.0) | 0.45 | < 0.001 | 58.9 (21.2) | 0.32 | < 0.001 | 57.6 (20.9) | 0.26 | 0.006 |
| | PCS | 48.5 | 33.9 (6.3) | 37.8 (6.9) | 0.63 | < 0.001 | 37.4 (6.7) | 0.56 | < 0.001 | 38.3 (7.8) | 0.71 | < 0.001 |
| | MCS | 48.9 | 37.9 (12.2) | 40.4 (11.3) | 0.20 | 0.023 | 39.5 (12.5) | 0.13 | 0.277 | 39.3 (12.6) | 0.11 | 0.495 |
| NASS | Pain | – | 17.7 (19.1) | 29.6 (22.4) | 0.62 | < 0.001 | 27.6 (21.3) | 0.52 | < 0.001 | 26.3 (21.2) | 0.45 | 0.001 |
| | Function | – | 59.8 (15.3) | 64.1 (15.7) | 0.28 | 0.001 | 65.0 (16.2) | 0.34 | < 0.001 | 66.1 (18.5) | 0.41 | < 0.001 |
| | Pain & function | – | 51.4 (14.2) | 57.1 (15.5) | 0.40 | < 0.001 | 57.6 (16.2) | 0.44 | < 0.001 | 58.1 (17.9) | 0.48 | < 0.001 |
| | Neurogenic symptoms | – | 68.1 (20.4) | 71.5 (19.8) | 0.17 | 0.040 | 70.7 (21.1) | 0.13 | 0.075 | 69.2 (22.4) | 0.05 | 0.578 |
| HADS | Depression | 81.6 | 63.8 (20.4) | 69.3 (19.6) | 0.27 | < 0.001 | 66.9 (23.0) | 0.15 | 0.083 | 66.5 (22.1) | 0.13 | 0.134 |
| | Anxiety | 77.8 | 63.3 (19.1) | 65.1 (18.9) | 0.09 | 0.211 | 64.8 (20.3) | 0.08 | 0.248 | 66.2 (21.0) | 0.15 | 0.094 |
| CSQ | Hoping | – | 36.3 (18.5) | 42.9 (21.3) | 0.35 | < 0.001 | 48.6 (23.7) | 0.66 | < 0.001 | 45.1 (23.0) | 0.47 | < 0.001 |
| | Catastrophizing | – | 60.1 (19.2) | 68.1 (19.5) | 0.41 | < 0.001 | 66.6 (22.9) | 0.34 | 0.001 | 66.4 (22.5) | 0.33 | 0.001 |
| | Activity level | – | 64.6 (14.6) | 66.0 (13.4) | 0.10 | 0.205 | 65.7 (14.9) | 0.08 | 0.410 | 66.4 (14.7) | 0.12 | 0.254 |
| | Control pain | – | 45.0 (19.6) | 48.7 (19.6) | 0.19 | 0.064 | 51.2 (23.3) | 0.32 | 0.008 | 50.5 (20.5) | 0.28 | 0.044 |
| | Decrease pain | – | 43.2 (18.1) | 48.1 (20.0) | 0.27 | 0.035 | 47.5 (21.6) | 0.24 | 0.062 | 46.0 (19.2) | 0.15 | 0.180 |
| SF-36: Short Form 36. NASS: North American Spine Society cervical spine self-assessment instrument. HADS: Hospital Anxiety and Depression Scale. CSQ: Coping Strategies Questionnaire. PCS: physical component summary. MCS: mental component summary. Norm: population-based normative values. m: arithmetic mean. s: standard deviation. ES: effect size. p: probability of type I error. |
Analysis
Assessments were performed on admission to the clinic (baseline), on discharge from the clinic (1 month follow-up), 3 months after baseline, and 6 months after baseline. This study describes the findings for the patients who completed all 4 assessments. However, all patients were treated whether or not data assessment was successful, in order to maintain the principles of an intention-to-treat analysis. The non-completers were characterized in a post-hoc analysis to assess selection bias. All analyses were performed using the statistical software package SPSS 17.0 for Windows® (SPSS Inc., Chicago, IL, USA). Significance tests were performed by the non-parametric Wilcoxon test for continuous data, since most of the characteristics and scores were not normally distributed, and by the χ2 test for frequency data.
Descriptive statistics for all instrument scores were scaled from 0 = worst to 100 = best health/function in accordance with the original scoring of the SF-36, and to ease comparison with scores obtained from other instruments (8). To be determinable, the specific “missing rules” of the instruments had to be fulfilled. This means that at least 50% of the items had to be completed for each of the SF-36 scales, 2/2 for the NASS pain scale, and 5/8 for each of the function and neurogenic symptom scales, 6/7 for each of the HADS scales, and 2/3 of the items for each CSQ scale (19, 23, 25, 29). The scores of the SF-36 and the HADS were compared with population normative data using the Wilcoxon test.
The effects were quantified by “effect size” (ES), which is the score difference between the baseline and follow-up divided by the sample’s standard deviation at baseline, i.e. the unit-free change in number of baseline standard deviations (31). This description of changes in closed scaled scores has several numeric and statistical advantages; in particular, it permits comparison of the effects obtained for different scales. Positive ES reflects improvement or reduction of deterioration. An ES of 0.20–0.49 is considered a small effect, 0.50–0.79 a moderate effect, and 0.80 or more a large effect (31). An ES ≥ 0.40 is considered to be higher than the minimal clinically important difference (MCID), the effect which patients can subjectively perceive (32). To be also statistically significant, a sample size of n ≥ 100 is required for ES ≥ 0.40 when using a type I error of 0.05 and a power of 0.80 (32). Instead of the t-test used in (33), the more conservative, non-parametric Wilcoxon test was applied. In multiple testing, the probability that one test reveals significant increases with the number of tests (k) and the level of the type I error should be reduced to p = 0.05/k = 0.0023 when k = 21 scores are tested (see Table III). This is the Bonferroni correction, the most conservative approach to solve this issue (34).
Results
Patients
Of the 185 included patients, 10 dropped out between entry and discharge (Fig. 1). Of these, 4 did not complete the therapy programme (premature discharge): 1 had conflicts with the other patients in the therapy group, 1 left the hospital without indicating a reason, 1 had to go back to work after 3 weeks because she was on the staff of a large company, and the fourth returned home because her dog had to have an operation. Of the 175 patients, who completed the inpatient rehabilitation, 72 (41%) were lost to the 6-month follow-up, whereby 66 (38%) did not return the questionnaires after returning home even after reminder letter. As an exception to the inclusion criteria, 1 patient was admitted only 2.4 months (i.e. < 3 months) after the accident due to reasons of time management and because signs of risk for chronification were observed (Table II).
| Table II. Sociodemographic and disease-relevant data at baseline (n = 103) |
| Characteristics | % |
| Sex, female | 79.6 |
| Education Basic school (8–9 years) Vocational training College/high school/university | 2.9 19.4 77.7 |
| Living, with partner/spouse | 64.1 |
| Smoking, yes | 34.0 |
| Sports > 2 hweek > 0–2 h/week None | 25.3 44.7 30.0 |
| Comorbidities (n) None 1 2 3 4 or more | 16.5 34.0 26.2 14.6 8.7 |
| Type of accident Car Motorbike Bicycle At work At sports/leisure | 77.7 2.9 3.9 3.9 11.7 |
| Therapy interventions in the last 3 months before the pain programme Physician consultation Psychiatrist consultation Psychologist consultation Physiotherapy: exercises Physiotherapy: passive | 90.9 3.9 17.5 59.2 83.5 |
| Work or employment status Employed Self-employed Jobless In education 100% compensation | 65.0 14.6 13.6 5.8 1.0 |
| Age (years) mean (standard deviation) Minimum–maximum | 37.9 (11.9) 17.5 – 63.5 |
| Body mass index (BMI) (kg/m2) Minimum–maximum | 24.4 (4.9) 16.3 – 38.9 |
| Time since whiplash injury (months) Minimum–maximum | 13.3 (10.1) 2.4 – 56.8 |
The socio-demographic and disease-relevant data of the 103 study completers at baseline are listed in Table II. The characteristics of the patients were predominantly: young, female, well-educated, slim, sporty, and (surprisingly for their young age) highly comorbid. Passive physiotherapies, such as massage, reflex zone massage of the foot, electro-therapy, and ultrasound therapy, were more frequently undergone than active physiotherapy, such as active individual physiotherapy or medical training therapy before the clinic stay.
There were complete score data for all self-assessment instruments according to the missing rules at baseline. At the 6-month follow-up, data were complete for all scores, except for SF-36 physical functioning and CSQ praying (one missing, respectively).
Health and quality of life (primary outcomes)
At baseline and all follow-ups, all observed SF-36 and HADS scores were significantly worse than expected from the general population norm (all p < 0.001, Wilcoxon test’s z-values 4.7–8.8) (Table III; z and p data not shown in detail). Patients suffered especially from pain.
During the stay in the clinic, and on average, the patients reported substantial improvements in important health dimensions and no worsening of any score (Table III): at discharge there were large and statistically significant improvements in SF-36 role physical and moderate improvements in SF-36 physical functioning, SF-36 bodily pain, SF-36 vitality, SF-36 physical component summary (PCS), and NASS pain. CSQ catastrophizing showed only small improvement. At the 3-month follow-up there were comparable effects. At the 6-month follow-up most effects were persistent, e.g. large improvements in SF-36 physical functioning and SF-36 role physical.
Considering all 3 follow-up time-points and using the 5% type I error level, 21/30 comparisons of baseline to follow-up scores showed significance in the SF-36 scores, 10/12 in the NASS, 1/6 in the HADS, and 9/15 in the CSQ. Using the more conservative, Bonferroni-corrected p = 0.0023 (see Methods), 19/30 comparisons showed significance in the SF-36 scores, 9/12 in the NASS, 1/6 in the HADS, and 6/15 in the CSQ (Table III). The improvements in SF-36 general health, SF-36 social functioning, SF-36 role emotional, SF-36 MCS, NASS neurogenic symptoms, HADS depression and anxiety, CSQ activity level, CSQ control pain, and CSQ decrease pain were small at all time-points.
Working capacity and medication (secondary outcomes)
Regular medication (at least 1 dose/day) during the observation period is shown in Table IV. During the hospital stay, the medication regimen was changed by reduction of all drugs, especially analgesics and anti-inflammatory drugs. Only 4.9% of the patients entered the clinic without medication, but 38.8% left the clinic without any regular medication. Approximately 4 of 5 patients who took analgesics, antiphlogistics, or myorelaxants regularly on admission could manage without them on discharge. No patient took opiates. The serotonin noradrenalin reuptake inhibitors (SNRIs) were prescribed more frequently during the hospital stay since they are well known to have positive effects on pain perception. The other antidepressants remained largely unchanged during the course of the study. At home, i.e. at the 3 and 6 month follow-upps, it revealed that the medication pattern had reverted slightly towards that of baseline, but there was still a substantial decrease, especially pain medication. We refrained from significance testing on these changes in order to limit the volume of data.
| Table IV. Medication and change in medication during the course of the disease |
| Patients (%) on: | Entry | Discharge | 3 months | 6 months |
| No medication | 4.9 | 38.8 | 17.5 | 15.5 |
| Paracetamol | 49.5 | 10.7 | 26.2 | 31.1 |
| Opioids | 23.3 | 4.9 | 13.6 | 14.6 |
| NSAIDs | 60.2 | 8.7 | 22.3 | 24.3 |
| Tricyclics | 18.4 | 17.5 | 12.6 | 17.5 |
| SSRIs | 10.7 | 12.6 | 10.7 | 14.6 |
| SNRIs | 5.8 | 10.7 | 7.8 | 6.8 |
| Tranquillizers | 2.9 | 1.9 | 4.9 | 4.9 |
| Myorelaxants | 20.4 | 4.9 | 6.8 | 9.7 |
| Other drugs | 28.2 | 35.9 | 10.7 | 14.6 |
| NSAIDs: non-steroidal anti-inflammatory drugs; SSRIs: selective serotonin reuptake inhibitors; SNRIs: selective serotonin and norepinephrine (noradrenaline) reuptake inhibitors. |
Working capacity was assessed by working hours per week as categorized in Fig. 2. On entry, and at the 3- and the 6-month follow-ups, this was reported by the patients themselves and reflects the effectively performed working hours. On discharge, this was assessed and prescribed by the clinic physician at the final visit. The median working hours were 42 before the accident (average full-time work-load in Switzerland), 15 after the accident, 8 on entry to the clinic, 21 on discharge, 20 at 3 months, and 21 h at 6 months after baseline. The working capacity increased significantly at all 3 follow-ups compared with that at baseline (each Wilcoxon’s p < 0.001). No working capacity (0 h/week) was reported by 45.6% of subjects on entry, 6.8% on discharge, 16.0% at the 3 month, and 18.4% at the 6 month follow-up. The corresponding proportions for full working capacity (at least 42 h/week) were 2.9%, 11.7%, 10.6% and 13.6%.
Outcome of drop-out patients (post-hoc analysis)
The 72 patients lost to follow-up between discharge and the 6-month follow-up (i.e. when returned home) showed similar characteristics to those of the 103 study completers regarding sex, age, all baseline and effect data of the SF-36 and the HADS. For example, mean age was 36.4 vs 37.9 (Wilcoxon’s p = 0.362) (always: patients lost to follow-up vs study completers), baseline SF-38 bodily pain 26.5 vs 27.3 (p = 0.802) and ES = 0.41 vs 0.67 (p = 0.080), and baseline HADS depression 59.9 vs 63.8 (p = 0.150) and ES = 0.25 vs 0.27 (p = 0.903). This means that the patients lost to follow-up were slightly younger, reported slightly more symptoms, and experienced slightly lower improvements at discharge, but none of these differences reached statistical significance.
Discussion
In this observational, prospective cohort study, small to large effects (ES up to 0.87) in biopsychosocial health and coping were observed in patients with chronic neck pain after whiplash injury who had undergone a standardized inpatient interdisciplinary pain management programme. Moderate to large lasting improvements were seen in all important health domains. Analgesic and antiphlogistic medication was reduced and working capacity was substantially increased for the long-term (median of working hours/week: from 8 to 21). Patients underwent more active strengthening and exercise therapy during the programme than before. Although the effects cannot be exactly quantified because of the lack of randomized controlled study design, the observed findings show that interdisciplinary programmes can improve health in severely affected whiplash patients. Although the effects cannot be quantified exactly because of the lack of randomized controlled study design, the observed findings may have consequences for countries in which whiplash injury is accepted as a disorder (3, 4, 6, 7, 35).
Detailed analysis of our results shows that pain decrease was recorded at all follow-up time-points as a moderate effect both in general (SF-36) and neck-specific (NASS) pain. Physical function improved mainly in general activities and ambulation as assessed by the SF-36 (ES up to 0.81) but less by the NASS (ES up to 0.41), which asks about functional limitations due to neck pain. Affective health and coping dimensions were less responsive. This may also be due to lack of responsiveness of some of the instruments’ scales (30).
This is, to the best of our knowledge, the first study reporting outcome after interdisciplinary rehabilitation where such significant effects in patients with chronic whiplash-associated disorders were observed. Other reviewed studies about multimodal rehabilitation programmes showed no or small effects (15). The only directly comparable study examined 62 patients after 5- and 8-week outpatient interdisciplinary pain programmes in Sweden (5). Measured on the pain visual analogue scale (VAS), neck pain decreased by ES = 0.30 on discharge and ES = 0.21 at the 6-month follow-up in this Swedish study, i.e. effects on pain were far lower than ours (ES = 0.62 and 0.65 at discharge, 0.45 and 0.63 at 6 months). Effects on pain and function were close to zero and not significant when measured on the sensitive Multidimensional Pain Inventory (MPI). Depression and coping scales did not show significant improvements. A randomized controlled trial (RCT) compared outpatient multimodal physiotherapy (n = 36) with self-management (n = 35) and reported an ES = 0.51 for an aggregated score of pain and disability (calculated from the data) (35). Possible reasons for the higher effects observed in our study are the patients’ high level of motivation to participate in the therapy programme, the intensive therapy programme consisting of evidence-based modalities (e.g. exercise therapy, cognitive behavioural therapy, etc.), the high level of experience of the therapy team, and the peer group effect during the clinic stay (36).
Due to the lack of a control group and randomization in this study it was not possible to compare the effects with those of other interventions or to draw strong causal conclusions about the relationships between intervention and effect (9, 37). Nevertheless, these encouraging results are likely to be at least partly explained by the intervention itself, by high patient motivation, and the experienced care team. The positive effects were coincident to the therapeutic intervention and most of the aetiopathogenetic pathways (e.g. exercise improves function, cognitive behavioural therapy reduces pain, information about the disorder improves self-competence and reduces symptoms) were empirically proven by other studies (9–15, 18). Coincidence and known pathway are 2 important criteria for causality (8, 38). A randomized controlled design is the so-called “gold standard” to quantify effects and to examine causalities, but it is difficult to realize. The complex situation of difficult patients and their expectations and beliefs, high disease burden and psychosocial problems, and unwillingness of health insurance companies to pay are high obstacles to performing this design of an ideal study in clinical reality. An indication of these difficulties is the high drop-out rate when patients return home, as was observed in our parallel programme for chronic (back/fibromyalgia) pain (8).
Strengths of the study are: the observational, “naturalistic” study design, i.e. without artificial processes of patient allocation or adaptation of the intervention, is close to clinical reality and has been discussed in detail previously (8, 36, 37). The comprehensive and specific assessment of health and quality of life satisfies the WHO’s concept for the International Classification of Function, Disability and Health (ICF) (39). Dimensions of all 3 ICF levels were assessed by the SF-36 and the MPI: level 1: function/impairment of the organ/tissue, level 2: functional impairment of the whole person, level 3: participation/restriction in social interaction. The HADS mainly addresses level 2, the CSQ levels 2 and 3, and the additional data regarding sports, working capacity, etc. levels 2 and 3. Self-assessments are valid, especially for whiplash injury (39). The 4 standardized, validated, internationally applied instruments and standardized effects allow quantifying, comparing, and interpreting the results to evidence-based standards.
The study’s main limitations are the non-randomized design and the relatively high drop-out rate between discharge and the 6-month follow-up of 72/175 (41%). In epidemiology, v< 25% would be an “acceptable” drop-out rate, i.e. one with low potential for selection bias. Patients lost to follow-up showed slightly worse health and slightly lower effects than the study completers (see: Results, post-hoc analysis), but overall similar characteristics. The highest difference was observed in the SF-36 vitality scale: ES at discharge: 0.41 for the drop-outs (n = 72), 0.67 for the study completers (n = 175). Therefore, if all included patients had completed the study at 6 months the effects would have tended to be lower. For SF-36 vitality, the ES at 6 months can be estimated by an effect reduction by (0.67–0.41)/0.67*(72/175)*100% = 16.0%, i.e. an ES = 0.45 (hypothetic n = 175) instead of the observed ES of 0.53 (n = 103). All other differences between the study completers and the drop-outs were lower and all were not significant. By that, no substantial selection bias on the effect results should be assumed.
In conclusion, after inpatient, structured interdisciplinary rehabilitation including adaptation of drug regimen, graded activity exercise, relaxation therapies, and cognitive and operant behavioural therapy, moderate to large short- and mid-term improvements were shown in pain, physical health, vitality, working capacity, medication reduction, and coping. These effects were observed in severely affected, chronic whiplash patients with poor response to previous outpatient therapies. Further controlled studies are required to quantify and attribute these improvements more precisely.
ACKNOWLEDGEMENTS
This study was supported by the Zurzach Rehabilitation Foundation SPA. We are grateful to Ms Joy Buchanan for helping to prepare the manuscript.
Conflict of interest: The authors declare no conflicts of interest.
REFERENCES