Ana Claudia Gomes Carreira, OT, Anamaria Jones, PT and Jamil Natour, MD
From the Rheumatology Rehabilitation Section, Rheumatology Division, Federal University of São Paulo, Brazil
Ana Claudia Gomes Carreira, OT, Anamaria Jones, PT and Jamil Natour, MD
From the Rheumatology Rehabilitation Section, Rheumatology Division, Federal University of São Paulo, Brazil
OBJECTIVE: To assess the effectiveness of a functional splint for trapeziometacarpal osteoarthritis.
METHODS: Forty patients with a diagnosis of painful trapeziometacarpal osteoarthritis of the dominant hand were randomized into 2 groups. The study group received the splint at baseline and used it during activities of daily living for 180 days and the control group used the splint only during the evaluations for the first 90 days and during activities of daily living for the following 90 days. Pain, strength, hand function and dexterity (with and without splint) were measured by a blinded assessor at baseline, 45, 90 and 180 days.
RESULTS: The groups were homogenous at baseline for all outcomes evaluated. Pain without the splint was significantly different between groups over time; the study group experienced a decrease in pain beginning with the first evaluation (45 days), whereas the control group achieved a lower pain score only at the end of the study, after having used the splint for 90 days. No significant differences between groups were found for the other parameters.
CONCLUSION: Splint use during activities of daily living for patients with trapeziometacarpal osteoarthritis reduces pain, but does not alter function, grip strength, pinch strength or dexterity.
Key words: functional splint; trapeziometacarpal joint; osteoarthritis; pain; function.
J Rehabil Med 2010; 42: 469–474
Correspondence address: Dr. Jamil Natour, Disciplina de Reumatologia, Rua Botucatu 740, São Paulo SP, Brazil, CEP 04023-900. E-mail: jnatour@unifesp.br
Submitted February 18, 2009; accepted January 15, 2010
INTRODUCTION
Osteoarthritis (OA) is one of the most common joint diseases. It affects approximately 12% of the population over 65 years in the USA (1,2). In Brazil it affects between 6% and 12% of adult population (3). The incidence is lower among individuals under the age of 40 years and increases progressively. OA is more common between 51 and 60 years of age and is more symptomatic among post-menopausal females (1, 4).
The prevalence of OA of the hand varies widely. A prospective cohort study did in the Netherlands, based on radiographic data shows that 67% of women and 54.8% of men may have one joint affected. The most commonly affected sites are the distal interphalangeal joints (47.3%), trapeziometacarpal (TMC) joint (35.8%), proximal interphalangeal joints (18.2%) and metacarpophalangeal joints (MCP) (8.2%) (5).
Patients with OA of the hand normally experience a loss of manual ability and grip strength, especially when the TMC joint is affected (6–9). The TMC joint has 2 main functional characteristics: freedom of movement and stability (10, 11). It is considered one of the most important hand joints, as 45% of hand function results from the action of the thumb (12).
One of the primary factors in OA of the TMC joint is believed to be the inherent laxity of the volar oblique ligament. When this joint is repeatedly stressed, subluxation occurs, resulting in incongruity of opposing surfaces, inflammation and eventual degeneration. These joint changes cause stiffness, which is often increased by the formation of osteophytes in the trapezium or metacarpal base. Movement can be further limited if the TMC joint becomes fixed in a dorsally subluxed position, limiting radial adduction. The thumb metacarpophalangeal joint may become hyperextended in an effort to compensate (13).
The main symptoms of OA of the TMC joint are pain in the dorsoradial and volar face of the hand on the projection of the angle formed by the index finger and thumb in abduction, and loss of grip strength. The aims of conservative treatment include the preservation of the first interdigital space, pain relief, maintenance of thumb function, orientation regarding joint protection, energy conservation and the use of adaptations. In the rehabilitation process, splints are a therapeutic resource that provide patients with the opportunity to achieve their maximum recovery potential (14–17).
Conservative treatment of OA of the TMC includes analgesics, joint protection, strengthening exercises of the intrinsic and extrinsic muscles of the thumb, assistive devices and splints. Surgical management may be recommended to relieve intractable pain. The procedure used varies according to disease stage (13).
Splints for OA of the TMC provide external support to the joint, thereby stabilizing the adjacent joints capable of compensatory movements and maintaining the first joint space (18, 19). The literature on splints for OA of the TMC is scarce, but a number of authors report that many rheumatologists recommend their use, although they do not publish studies on the subject (20). A prospective study that examined the effectiveness of steroid injection in combination with splinting found that this kind of treatment provided reliable long-term relief to the thumb (21).
A randomized controlled trial (RCT) comparing 2 6-week splint and exercise regimens for patients with trapeziometacarpal OA found that both groups improved; however, no differences were found between groups regarding pain, strength or hand function (22). Another RCT comparing a custom-made neoprene splint and usual care found that the splint had no effect on pain at 1 month, but improved pain and disability at 12 months; however, the splint was a rigid rest splint recommended for use only at night and the assessor was not blinded (23). Another RCT comparing a joint protection programme alone and joint protection programme with the addition of day/night splints and hot pack/home exercise found that when an exercise regimen and a splint are added to a joint protection programme, there is a greater improvement in pain, stiffness, grip strength and performance on activities of daily living in comparison with the joint protection programme alone (24).
A review published in 2007 concluded that, although evidence regarding the effectiveness of splinting for carpometacarpal OA is underdeveloped, the research to date indicates that splinting may help relieve pain. Further investigation is recommended using a controlled methodology, more thorough reporting of outcomes and tracking of analgesic use. Given the conservative nature and relatively low cost of splinting, it is recommended that patients be given the opportunity to try a splint (25).
The aim of the present study was to assess the effectiveness of a functional splint for the thumb of the dominant hand of patients with Grade II and III OA of the TMC joint.
METHODS
Forty patients with a diagnosis of OA of the TMC joint of the dominant hand were randomized into 2 groups of 20 individuals. Eligibility criteria were: a clinical and radiological diagnosis of idiopathic Grade II and III OA of the TMC joint of the dominant hand; (26) either gender; over 40 years of age; and pain in the base of the thumb of the dominant hand of between 3 and 7 on the 0–10 cm visual analogue scale (VAS) for pain.
Exclusion criteria were patients with severe deformities of the dominant hand that did not allow gripping between the first, second and third fingers; deformities of the distal interphalangeal joint; the use of a splint on the thumb in the previous 6 months; surgery on the hand under study in the previous 6 months or scheduled in the upcoming 6 months; allergy to the splint material; incapacity to respond to the questionnaire and perform the tests; geographical inaccessibility; injections in the hand under study in the previous 6 months; other associated diseases such as carpal tunnel syndrome, fractures in the carpus, tendonitis, chronic inflammatory arthropathy and alterations in the use of anti-inflammatory medication and analgesics in the previous 3 months.
The present study was approved by the ethics committee. All patients signed terms of informed consent and were randomly allocated to 2 groups of 20 patients: splint group (SG) and control group (CG). A computer-generated randomization list was used to randomly allocate patients into the groups and concealed allocation was carried out with opaque sealed envelope.
This trial was registered at clinicaltrials.gov (ID: NCT00612248).
Intervention
An occupational therapist (ACGC) specialized in rheumatology with 10 years experience confected a functional thermoplastic splint for the participants of both groups, the aim of which was to stabilize the TMC joint, maintaining the pulp of the distal phalange of the index finger free for gripping with the other fingers and leaving the thumb in a functional position (Fig. 1) (18). Patients in the SG received the splint on the day of the first evaluation and took it with them for use during activities of daily living, including paid or unpaid work. They were instructed to remove it during rest (sleeping), bathing and activities in which they had contact with heat. They were also instructed as to how to put the splint on and cleaning procedures. In cases of discomfort regarding the use of the splint, patients were instructed to communicate with the therapist in order to perform the necessary adjustments.
Fig. 1. Model of confected splint.

Patients in the CG initially used the splint only during the evaluations. The splints remained in the possession of the researcher and were only given to patients for home use after the third evaluation (T90). Patients of the CG used the splint daily between T90 and T180.
Evaluations
Evaluations were carried out by a blinded assessor at baseline (T0), after 45 days (T45), after 90 days (T90) and after 180 days (T180). All evaluations were performed by a physiotherapist trained to administer the tests. At the beginning of each evaluation the occupational therapist in charge of the study inspected the splints of the patients in the SG and gave the splints to the patients in the CG so that all patients saw the assessor wearing their splints. Patients were instructed not to comment to the evaluator regarding the use of the splint.
The primary outcome was:
• Pain in the base of the thumb – a VAS from 0 to 10 cm was used, for which 0 represents no pain and 10 represents unbearable pain. The patient indicated his/her level of pain on the scale using the tip of a pen. Pain was assessed in 2 stages:
• Pain without the splint – average pain the patient felt in the previous week without the use of the splint;
• Pain with the splint – average pain the patient felt using the splint during the evaluation.
The secondary outcomes were:
• Functional capacity – the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire was used. This instrument is composed of 30 questions measuring function and symptoms. It includes 2 items on physical function, 6 items on symptoms and 3 items on social aspects (Q3). There are also 2 optional modules with 4 items each –one for athletes and musicians (Q1) and another for workers (Q2). All items were answered based on the patient’s experiences in the previous week. If the patient did not have the opportunity to perform one of the activities in the previous week, he or she was asked to estimate the most accurate response. The score ranges from 0 to 96 points, for which higher scores represent worse functional capacity (27).
• Grip strength – the Jamar dynamometer was used. The test was carried out of the dominant hand with and without the splint. Patients were seated with the elbow at 90 degrees of flexion and the wrist in a neutral position between pronation and supination. The dynamometer was set at number 2, in accordance with the instruction manual (PC-5030J1 – Preston/Trenton, Ontario Canada; Mathiowetz, 1984). Measurements were taken in Kgf, from which the mean result was considered for analysis. Participants were verbally encouraged to make an effort during all measurements.
• Pinch strength – a pinch gauge dynamometer was used. The test was performed with the dominant hand both with and without the splint. Patients were in the same position as in the grip strength test. Three measures were taken for each pinch (tip and key pinch), for which the mean in Kgf was considered in the analysis, in accordance with the instruction manual for the equipment (A853-4-Smith & Nephew/Germantown, USA, Mathiowetz, 1984). Participants were verbally encouraged to make an effort during all measurements.
• Upper limb dexterity – the O’Connor test equipment was used (Lafayette Instrument®, USA). Dexterity in the O’Connor test is defined as the time it takes to place three pins in one hole on five rows of the board. Patients performed the test while seated and the board was placed on a table in front of them. Patients were allowed to make a practice run in order to become familiar with the test, following the manufacturer’s instructions. The performance time was recorded in seconds using a chronometer from the first to fifth row (1st time) and then from the sixth to tenth row (2nd time). Both times were used for the calculation of the final score.
Statistical analysis
A minimum of 17 patients per group were needed in order to identify a 2-cm improvement in the VAS for pain with a 0.05 alpha and 0.20 beta. Forty patients were randomized in order to compensate for a possible loss of 20%. The significance level was set at p < 0.05. All tests were performed using the SPSS version 10 (SPSS, Chicago, IL, USA) and intention-to-treat analysis was carried out when necessary. Pearson’s χ2 and Fisher’s exact tests were employed to determine the homogeneity of the sample. Categorical variables were analysed using the Mann-Whitney test.
The data were analysed in 2 stages:
• Period A – comparison between groups over time – between T0 and T90.
• Period B – comparison between groups over time – between T0 and T180.
For data with normal distribution in periods A and B, analysis of variance (ANOVA) for repeated measurements was used to determine differences in the behaviour of the groups over time considering the existing relationship between evaluations of a single individual. When a statistically significant difference over time was found between groups, the Mann-Whitney or t-tests were used to analyse differences at each time. Analysis of the VAS for pain score with the use of the splint was performed at T45, T90 and T180 using an independent-sample t-test, as both groups were only assessed for this parameter beginning at T45, at which point the difference was already evident. Pain, strength and dexterity parameters with and without the use of the splint were compared in both the SG and CG at each assessment time using a paired t-test.
RESULTS
The groups were homogenous at baseline with regard to age, disease duration, gender, degree of OA of the TMC, dominance, race and profession. Median age was 65.5 years in the control group and 64.8 years in the study group. There was a predominance of female subjects, which is similar to the prevalence of the disease (4, 7). All 40 patients who began the study completed all the evaluations; no patient was lost throughout the study period. Fig. 2 shows the patient flow-chart for each step of the study. Table I displays the sample characteristics with regard to age, disease duration, gender, ethnicity, level of schooling, profession, pain, DASH, grip strength, pinch strength and dexterity on the initial evaluation.
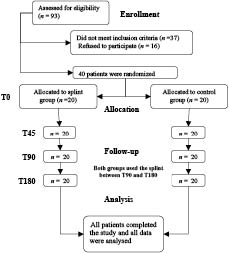
Fig. 2. Participants in each stage of the trial.
| Table I. Population characteristics at baseline | |||
| SG (n = 20) | CG (n = 20) | p | |
| Age, years, mean (SD) | 62.8 (8.5) | 65.1 (10.1) | 0.665 |
| Duration of disease, years, | 6.3 (3.4) | 7.7 (6.1) | 0.503 |
| Gender, female/male, n | 20/0 | 18/2 | 0.147 |
| Degree disease, II/III, n | 19/1 | 20/0 | 0.311 |
| Ethnicity, white/non-white, n | 13/7 | 14/6 | 0.736 |
| Hand dominance, right/left, n | 19/1 | 20/0 | 0.311 |
| Pain – VAS, cm, mean (SD) | |||
| without splint | 5.1 ( 1.4) | 5.1 (1.1) | 0.978 |
| Grip strength (Kgf – mean (SD)) | |||
| with splint | 18.1 (8.8) | 20.2 (7.3) | 0.185 |
| without splint | 18.7 (6.8) | 20.5 (7.7) | 0.409 |
| Pinch strength – key, Kgf, mean (SD) | |||
| with splint | 4.6 (1.5) | 4.9 (1.5) | 0.413 |
| without splint | 5.4 (1.9) | 5.2 (1.7) | 0.625 |
| Pinch strength – tip, Kgf, mean (SD) | |||
| with splint | 3.5 (1.3) | 3.4 (1.2) | 0.775 |
| without splint | 3.3 (1.2) | 3.1 (0.9) | 0.303 |
| Dexterity, s, mean (SD) | |||
| with splint | 334.2 (57.4) | 333.8 (66.5) | 0.871 |
| without splint | 357.4 (76.0) | 359.3 (81.6) | 0.766 |
| Hand function – DASH, mean (SD) | |||
| Question 1 | 2.8 (12.6) | 1.6 (5.7) | 0.594 |
| Question 2 | 15.0 (20.4) | 22.8 (28.0) | 0.383 |
| Question 3 | 42.0 (18.4) | 39.1 (16.9) | 0.655 |
| SG: study group; CG: control group; VAS: visual analogue scale; DASH: Disabilities of the Arm, Shoulder and Hand questionnaire; Kgf: kilogram force. | |||
Period A – analysis between T0 and T90
A reduction in the VAS for pain without the splint was observed in the SG, whereas pain remained constant in the CG. This difference was statistically significant between groups (p = 0.003) (Table II) and was observed at T45 and T90 (p = 0.013 and p = 0.002, respectively). In the intra-group comparison, pain reduced in the SG significantly in T0/T45 (p < 0.001) and T0/T90 (p < 0.001), demonstrating that the reduction in pain occurred in the first 45 days of treatment and was maintained for another 45 days (T90).
| Table II. Inter-group comparison of hand pain (VAS), functional capacity, grip strength, pinch strength and dexterity | ||||||||||
| T0 | T45 | T90 | T180 | |||||||
| CG | SG | CG | SG | CG | SG | p1 | CG | SG | p3 | |
| Pain (VAS – cm) | ||||||||||
| without splint | 5.1 (1.4) | 5.1 (1.1) | 4.8 (1.9) | 3.1 (2.1) | 5.2 (2.0) | 2.9 (2.2) | 0.003* | 4.4 (2.5) | 2.5 (2.6) | 0.009* |
| p2 | 0.950 | 0.013* | 0.002* | 0.023* | ||||||
| with splint | – | – | 4.8 (2.6) | 2.1 (1.6) | 4.3 (2.2) | 1.9 (1.9) | 0.680 | 3.4 (2.6) | 1.7 (2.1) | – |
| p2 | < 0.001* | 0.001* | 0.026* | |||||||
| Grip strength, Kgf | ||||||||||
| without splint | 18.7 (6.8) | 20.5 (7.7) | 18.3 (6.9) | 21.6 (5.8) | 20.1 (6.1) | 20.9 (6.4) | 0.311 | 20.1 (5.2) | 20.8 (5.3) | 0.207 |
| with splint | 18.08 (8.8) | 20.18 (7.3) | 18.3 (6.8) | 22.4 (5.5) | 19.5 (7.6) | 22.1 (7.2) | 0.150 | 20.2 (7.1) | 22.3 (5.6) | 0.217 |
| Pinch strength – key, Kgf | ||||||||||
| without splint | 5.4 (1.9) | 5.2 (1.7) | 5.5 (1.8) | 5.7 (1.4) | 5.7 (1.8) | 5.9 (1.6) | 0.360 | 5.7 (1.7) | 6.0 (1.7) | 0.882 |
| with splint | 4.6 (1.5) | 4.9 (1.5) | 4.9 (1.3) | 5.4 (1.2) | 5.2 (1.6) | 5.4 (1.7) | 0.742 | 5.3 (1.5) | 5.5 (1.6) | 0.540 |
| Pinch strength – tip, Kgf | ||||||||||
| without splint | 3.3 (1.2) | 3.1 (0.9) | 3.3 (1.2) | 3.7 (0.9) | 3.7 (1.1) | 3.8 (1.1) | 0.322 | 4.4 (1.3) | 4.1 (0.9) | 0.118 |
| with splint | 3.5 (1.3) | 3.4 (1.2) | 3.5 (1.3) | 3.9 (0.8) | 3.9 (1.2) | 4.1 (1.2) | 0.176 | 4.3 (1.0) | 4.3 (0.8) | 0.373 |
| Dexterity, s | ||||||||||
| without splint | 357.4 (76.0) | 359.3 (81.6) | 356.5 (146.5) | 330.8 (94.4) | 341.4 (117.1) | 309.5 (89.2) | 0.255 | 321.7 (67.7) | 295.7 (80.5) | 0.316 |
| with splint | 334.1 (57.4) | 333.8 (66.5) | 376.1 (157.1) | 318.1 (70.7) | 335.0 (97.8) | 295.4 (59.9) | 0.092 | 324.6 (63.2) | 297.1 (66.2) | 0.114 |
| Hand Function – DASH | ||||||||||
| Question 1 | 2.8 (12.6) | 1.6 (5.7) | 0.6 (2.8) | 1.6 (5.7) | 2.8 (12.6) | 3.1 (10.4) | 0.524 | 2.2 (9.8) | 2.5 (6.8) | 0.689 |
| Question 2 | 15.0 (20.4) | 22.8 (28.0) | 15.0 (18.9) | 20.3 (25.1) | 13.7 (17.5) | 19.4 (26.3) | 0.893 | 16.2 (17.5) | 15.3 (26.0) | 0.459 |
| Question 3 | 42.0 (18.4) | 39.1 (16.9) | 34.4 (14.5) | 31.8 (17.6) | 35.3 (13.2) | 28.6 (18.0) | 0.382 | 32.2 (11.1) | 22.0 (20.0) | 0.225 |
| Data are reported as mean (standard deviation); SG: study group; CG: control group; T0: baseline; T45: 45 days from baseline; T90: 90 days from baseline; T180: 180 days from baseline; VAS: visual analogue scale; DASH: Disabilities of the Arm, Shoulder and Hand questionnaire; Kgf: kilogram force; p1: p-value between SG and CG groups over time (T0–T90) using ANOVA; p2: p-value between SG and CG groups at each time using t-test; p3: p-value between SG and CG groups over time (T90–T180) using ANOVA. *Significant p-value. | ||||||||||
There were no significant differences between groups over time regarding the Q1 and Q2 scores of the DASH (p = 0.524 and p = 0.893, respectively). Both groups had a reduction in Q3 scores (p = 0.382). Regarding dexterity, grip and pinch strength with and without the splint, there were no significant intra-group differences over time (Table II).
| Table III. Intra-group comparisons between measurements with and without splint at each evaluation time for hand pain (VAS), grip strength, pinch strength and dexterity | ||||||||||||||||
| T0 | T45 | T90 | T280 | |||||||||||||
| CG | p1 | SG | p2 | CG | p1 | SG | p2 | CG | p1 | SG | p2 | CG | p1 | SG | p2 | |
| Pain, VAS, cm | ||||||||||||||||
| without splint | 5.1 (1.4) | 5.1 (1.1) | 4.8 (1.9) | 3.1 (2.1) | 5.2 (2.0) | 2.9 (2.2) | 4.4 (2.5) | 2.5 (2.6) | ||||||||
| with splint | – | – | 4.8 (2.6) | 0.920 | 2.1 (1.6) | 0.038* | 4.3 (2.2) | 0.078 | 1.9 (1.9) | 0.009* | 3.4 (2.6) | 0.039* | 1.7 (2.1) | 0.064 | ||
| Grip strength, Kgf | ||||||||||||||||
| without splint | 18.7 (6.8) | 0.517 | 20.5 (7.7) | 0.850 | 18.3 (6.9) | 0.927 | 21.6 (5.8) | 20.1 (6.2) | 20.9 (6.4) | 20.1 (5.2) | 20.8 (5.3) | |||||
| with splint | 18.1 (8.8) | 20.2 (7.3) | 18.3 (6.8) | 22.4 (5.5) | 0.443 | 19.5 (7.6) | 0.577 | 22.1 (7.2) | 0.264 | 20.2 (7.1) | 0.937 | 22.3 (5.6) | 0.140 | |||
| Pinch strength – key, Kgf | ||||||||||||||||
| without splint | 5.4 (1.9) | 0.003* | 5.2 (1.7) | 0.296 | 5.5 (1.8) | 5.7 (1.4) | 5.7 (1.8) | 5.9 (1.6) | 5.7 (1.7) | 6.0 (1.7) | ||||||
| with splint | 4.6 (1.5) | 4.9 (1.5) | 4.9 (1.3) | 0.004* | 5.4 (1.2) | 0.244 | 5.2 (1.6) | 0.011* | 5.4 (1.7) | 0.022* | 5.3 (1.5) | 0.026* | 5.5 (1.6) | 0.018* | ||
| Pinch strength – tip, Kgf | ||||||||||||||||
| without splint | 3.3 (1.2) | 0.320 | 3.1 (0.9) | 0.219 | 3.3 (1.2) | 3.7 (0.9) | 3.7 (1.1) | 3.8 (1.1) | 4.4 (1.3) | 4.1 (0.9) | ||||||
| with splint | 3.5 (1.3) | 3.4 (1.2) | 3.5 (1.3) | 0.175 | 3.9 (0.8) | 0.102 | 3.9 (1.2) | 0.298 | 4.1 (1.2) | 0.093 | 4.3 (1.1) | 0.501 | 4.3 (0.8) | 0.353 | ||
| Dexterity, s | ||||||||||||||||
| without splint | 357.4 (76.0) | 359.3 (81.6) | 366.5 (146.5) | 330.8 (94.4) | 341.4 (117.1) | 309.5 (89.2) | 321.7 (67.7) | 295.7 (80.5) | ||||||||
| with splint | 334.2 (57.4) | 0.014* | 333.8 (66.5) | 0.011* | 376.1 (157.1) | 0.061 | 318.1 (70.7) | 0.206 | 335.0 (97.8) | 0.422 | 295.4 (59.9) | 0.155 | 324.6 (63.2) | 0.552 | 297.1 (66.2) | 0.846 |
| Data are reported as mean (standard deviation); SG: study group; CG: control group; T0: baseline; T45: 45 days from baseline; T90: 90 days from baseline; T180: 180 days from baseline; VAS: visual analogue scale; DASH: Disabilities of the Arm, Shoulder and Hand questionnaire; Kgf: kilogram force; p1: p-value between CG measurements with and without splint using paired t-test; p2: p-value between SG measurements with and without splint using paired t-test. *Significant p-value. | ||||||||||||||||
Period B – analysis between T90 and T180
In the comparison between groups from T0 and T180, there was only a statistically significant difference in pain without the splint. The significant difference between groups from T0 to T90 regarding pain without the splint remained significant between T0 and T180 (p = 0.009). This demonstrates that, despite the improvement in the CG after using the splint for 90 days during activities of daily living, this improvement did not match that of the SG at the end of the study, which clearly demonstrates the benefit of the splint regarding pain. This benefit was already clear by T90 and the improvement in this parameter continued, demonstrating an additional gain for the SG regarding pain without the splint through to T180. No statistically significant differences between groups were found in Period B for the DASH, strength or dexterity (Table II).
VAS for pain with the splint
There was a statistically significant difference between groups regarding pain during the use of the splint (p < 0.001 at T45; p = 0.001 at T90; and p = 0.026 at T180).
Intra-group comparisons with and without the splint regarding pain, strength and dexterity
In the SG, a statistically significant difference was found for key pinch strength at T90 (p = 0.022) and T180 (p = 0.018), in which strength with the splint was lower than without the splint. Regarding dexterity, the test was performed slower with the splint than without the splint at T0 (p = 0.011). Pain scores were lower during the use of the splint (p = 0.038 at T45 and p = 0.009 at T90) (Table III).
In the CG, a statistically significant difference was found for key pinch strength for all the evaluations (p = 0.003 at T0, p = 0.004 at T45, p = 0.011 at T90 and p = 0.026 at T180), with strength always lower during the performance of the test with the splint. Regarding dexterity, the test was performed slower without the splint at T0 (p = 0.014). Pain scores were lower during the use of the splint at T180 (p = 0.039) (Table III).
DISCUSSION
The aim of the present study was to assess the effectiveness of a splint for OA of the TMC. The main parameter was pain reported by patients with and without the use of the splint, as pain is one of the reasons for dysfunction in manual abilities and the seeking of medical care. Together with deformities, pain can cause disability and dependence in activities of daily living. The participants in the study also complained of difficulty in performing daily tasks, correlating this difficulty to pain in the TMC joint.
The use of a splint during activities of daily living reduced pain in patients with OA of the TMC joint. Both groups showed improvement – the improvement in the SG occurred early in the study, whereas improvement in the CG occurred after T90, when this group also began using the splint during activities of daily living. This demonstrates the effectiveness of the splint in controlling pain related to OA of the TMC.
Rannou et al. (22) found similar results regarding pain among patients with OA of the TMC joint; however, this benefit was observed only after 12 months and the assessor of this trial was not blinded. An RCT published in 2004 also found a decrease on pain, but since the patients in both groups wore a splint and did exercise, it is difficult to say whether this result occurred due to the splint or the exercises (22). Nicholas et al. (28) found a similar result regarding pain, reporting that immobilization of the hands with the use of a splint provided a reduction in inflammation of the finger joints and concluding that patients obtain this reduction in pain depending on the duration of splint use; however, the study was not a controlled study. Another study proposing conservative treatment with the use of a splint as an alternative for patients with OA of the TMC joint demonstrated the benefit of splints in the reduction of the severity of symptoms, allowing patients to return to normal functions without significant pain. Unfortunately, this study was also not a controlled study, only employed one assessment instrument and had a short intervention time of just 3–4 weeks (29).
Despite the improvement in pain, the patients had no improvement in function, which was surprising, as we believed that function would improve with the reduction in pain. However, the DASH scores revealed no differences between groups, thereby demonstrating that the patients had no improvement in functional capacity. Upon analysing our results, we perceived that the DASH scores for both groups diminished and the improvement tended to be greater in the SG, despite not being statistically significant. We believe this may have occurred due to the fact that the patients did not exhibit an expressive functional loss at the initial evaluation (DASH scores indicated moderate disability). It is perhaps for this reason that no improvement in function was observed. Another consideration regarding the lack of effect measured by DASH is that this instrument has a number of items that are not specific to hand use or particularly the use of the thumb; thus, responsiveness for this particular purpose could be limited.
Regarding grip and pinch strength, we initially believed that the splint would stabilize the thumb, thereby improving strength and the reduction in pain would benefit this parameter as well, but we also feared that immobilization could lead to muscle atrophy and a reduction in strength. However, we observed no changes in palmar grip strength or tip pinch strength with the use of the splint. Therefore, the splint can be used without a loss of strength, even though its main function is the stabilization of the TMC joint during the performance of activities of daily living. With regard to key pinch strength, the splint led to reduced strength in both the SG and CG.
Caporrino (30) found mean palmar grip strength of 44.2 Kgf and 40.5 Kgf on the dominant and non-dominant side of healthy males, respectively, and 31.6 Kgf and 28.4 Kgf on the dominant and non-dominant side of healthy females, respectively. In the present study, we found lower means, consistent with those among patients with RA. Mean tip pinch strength is 6.70 Kgf for males and 4.67 Kgf for females and mean key pinch strength is 9.9 Kgf for males and 6.7 Kgf for females in the normal population (13). The means found in the present study were lower for both types of pinch strength, but also consistent with those among patients with RA.
No statistically significant difference was found between groups regarding manual dexterity. However, the patients in the SG had a shorter performance time on the O’Connor test with the use of the splint. We can therefore state that the use of a splint for OA of the TMC on this test, in which there are a greater number of repeated movements, offered protection to the TMC joint.
The discussion is hampered by the lack of publications with methodological quality on this subject. Very few articles have been published that scientifically report the use of a splint on OA of the TMC joint.
The present study had an uncommon design for a RCT, but it could help analyse better the effectiveness of splint use, as comparisons could be made with the control group, which did not use the splint the first 90 days, and further comparisons could be made between the group that used the splint for 180 days and the group that used it for 90 days to determine whether there was further improvement in the former after the first 90 days of splint use.
There were some limitations to the present study that should be addressed. The results cannot be extrapolated to other populations, as nearly all the participants were female. Data on compliance/adherence, side-effects and patients’ opinion of the splints were not assessed and blinding the patients was not possible.
The use of a splint during activities of daily living for patients with OA of the TCM joint in the dominant hand reduces pain in both the short and long term. Splint use does not change the final result of grip strength or tip pinch strength; nor does it have a great impact on functional capacity. It does, however, reduce key pinch strength during use.
ACKNOWLEDGEMENTS
This project was supported by the Fundacao de Amparo a Pesquisa do Estado de Sao Paulo (FAPESP).
REFERENCES

