Lech Furmaniuk, PhD, Grażyna Cywińska-Wasilewska, PhD and Dominik Kaczmarek, PhD
From the Department of Kinesiotherapy, The Eugeniusz Piasecki University School of Physical Education in Poznan, Poznan, Poland
Lech Furmaniuk, PhD, Grażyna Cywińska-Wasilewska, PhD and Dominik Kaczmarek, PhD
From the Department of Kinesiotherapy, The Eugeniusz Piasecki University School of Physical Education in Poznan, Poznan, Poland
OBJECTIVE: The aim of this study was to assess the influence of long-term wheelchair rugby training on the functional abilities of persons with tetraplegia over a 2-year period post-spinal cord injury.
DESIGN: A prospective non-randomized controlled trial.
PARTICIPANTS: Forty people with incomplete tetraplegia were examined. Participants were divided into 2 groups: a wheelchair rugby training group (n = 20) and a control group (n = 20).
Methods: The Wheelchair Skills Test was used to assess functional changes in patients. In order to assess the strength of the 10 key muscles in the upper limb, the American Spinal Injury Association (ASIA) motor score was used. All participants were assessed at the beginning of the study (at the start of wheelchair rugby training) and reassessed after 2 years. Between pre- and post-measurements patients from the wheelchair rugby group attended wheelchair rugby training once a week.
RESULTS: The baseline values of the Wheelchair Skills Test in the wheelchair rugby group was 71.3, and this increased significantly by 24%. In the control group, the mean Wheelchair Skills Test value was 63.2, and this improved by 4%. A significant correlation between Wheelchair Skills Test score and ASIA motor score was found in both groups.
CONCLUSION: Participation in regular wheelchair rugby training may preserve and augment functional abilities in individuals with incomplete tetraplegia.
Key words: spinal cord injuries; tetraplegia; wheelchair rugby; Wheelchair Skills Test.
J Rehabil Med 2010; 42: 688–690
Correspondence address: Lech Furmaniuk, Department of Kinesiotherapy, The Eugeniusz Piasecki University, School of Physical Education in Poznan, ul. Królowej Jadwigi 27/39, PL-61-871 Poznan, Poland. E-mail: lehoofur@wp.pl
Submitted September 14, 2009; accepted April 28, 2010
Introduction
The rehabilitation of patients after spinal cord injury (SCI) takes several years. In many cases, the process of rehabilitation is difficult because of complications that can be directly or indirectly the result of diminished motor activity. It is known that training improves physical capacity (increment in peak oxygen uptake (VO2peak) and peak power output (POpeak)), cardiorespiratory function cardiovascular, cardiac and metabolic state in patients after SCI (1–4). Hicks et al. (5) demonstrated that twice-weekly long-term resistance training can be as effective as thrice-weekly training in improving upper body muscle strength in persons with tetraplegia. Moreover, resistance training increased arm ergometry power output, and participants reported less pain, stress and depression after training (5). Additionally, it has been suggested that three weeks of massed practice training may contribute to the development of new movement strategies among patients with incomplete tetraplegia (6).
The activity of non-governmental organizations and sport clubs for disabled people is part of the rehabilitation process. In Poland, the Foundation of Active Rehabilitation (FAR) has the greatest experience in rehabilitating people after SCI. FAR organizes active rehabilitation training camps (ARTC), which provide the opportunity for wheelchair users to learn the basis of independent functioning. Moreover, FAR creates the opportunity for participation in regional training groups and wheelchair rugby (WR) training. There have been only a few studies on the effects of WR training in people with tetraplegia (7, 8). Therefore, the aim of this study was to assess the influence of long-term WR training on the functional abilities of persons with tetraplegia over a 2-year period post-spinal cord injury.
Methods
Study design
The design was a prospective non-randomized controlled study to compare the functional abilities of WR athletes and non-trained persons with tetraplegia.
Recruitment procedure
Participants were recruited in response to information given to the Polish Wheelchair Rugby League. Subjects admitted to the control group were recruited in response to information given to ARTC participants.
Inclusion/exclusion criteria
Patients were eligible to participate in the study if they had incomplete tetraplegia (ASIA impairment scale grades B and C) for more than a 5-year post-SCI period. Patients were excluded if they were unable to participate in exercise training due to cardiovascular or other disorders that could influence or limit their participation in training (sports injury, chronic neck or shoulder pain) or if they had pressure sores.
Participants
A total of 54 men with tetraplegia were initially recruited to our study, with a mean age of 29.4 years (range 21–54 years). Participants were divided into 2 groups: the WR group (n = 23) and control group (n = 31). During the study, 3 people dropped out of the WR group: 1 because of illness, 1 because of the implantation of a cardiac pacemaker, and 1 resigned. Eleven people in the control group dropped out because of transportation difficulties and work conflicts.
The study was approved by the local institutional review board, and all subjects read and signed an informed consent form before participating.
Rehabilitation programme
All patients from both groups attended the ARTC before the study. ARTC was an 8-day sports camp. Each day the participants had 3 training sessions, each lasting for 1.5 h, e.g. in wheelchair skills, swimming, table tennis and archery. Three athletes from the WR group participated at the health resort (including therapeutic exercises, cryotherapy, hydrotherapy, and electrotherapy) once a year, and none of them had individual physical therapy. Among the participants from the control group, 4 attended FAR’s training groups for 2 months of the first year of the study and 2 men participated in the rehabilitation camp. Only 1 person from the control group had individual physical therapy twice a week.
WR training plan
Patients assigned to the WR group were expected to attend supervised exercise sessions once a week for 2 years. Their training plan involved 3 phases. The main goal of the first phase was the physical preparation of athletes, and consisted of muscle strength and endurance training. The second phase included mainly technical skills, such as ball handling, passing, catching, carrying and dribbling, and wheelchair skills, such as pushing, starting, stopping, directional changes, tackling and blocking. During the third phase, athletes focused on tactical team skills. Exercise sessions included 10–15 min of warm-up, followed by WR training. The total exercise time was approximately 2 h. This was followed by a cool-down period of 10–15 min.
Outcome measures
All measurements and tests were performed in a professional sports centre and were supervised by experienced physiotherapists and trainers. The first assessment (initial examination) was performed at the start of the WR training programme (for WR group) and after the ARTC (for control group). The second assessment (final examination) was performed after 2 years.
The primary outcome was the estimation of the functional changes, measured using the Wheelchair Skills Test version 2.4 (WST). The test is based on 10 groups of skills: 6 groups of skills regarding wheelchair activities (e.g. wheelies, overcoming obstacles, turning and rolling, reaching objects and transferring into and out of a wheelchair) and 4 groups of skills about the wheelchair equipment (e.g. how to open and fold the wheelchair, how to move the footrests and armrests, and how to apply the brakes). If a participant failed to perform a skill on the first attempt, a second trial was permitted. The test duration was not time-limited. Each of the skills was assessed according to the following system: 0 – failed, 1 – passed. The result obtained was divided by the total number of skills and the final result was formulated as a percentage (WST%) (9). The secondary outcome was to assess changes in the strength of the 10 key muscles in the upper limb by manual muscle test, using a 7-grade scale according to the protocol of ASIA motor score (10).
In order to determine the effect of level of upper limb impairment on wheelchair skills changes we evaluated the relationship between ASIA motor score and the differences in the initial and final WST scores in both groups.
Statistical methods
Data are presented as means and standard deviations (SD). Differences between the means of the two dependent trials were assessed using Wilcoxon’s signed-rank test. Differences between groups were assessed using a Mann-Whitney U test, with the corresponding 95% confidence interval (95% CI). The relationship between the differences in the WST initial and final values and ASIA motor score was examined using Spearman’s rank correlation coefficient. The significance level was set at p < 0.05, and the statistical analysis was conducted using Statistica version 7.0 software.
Results
Twenty participants admitted to the WR group (mean age 30.0 years (SD 8.0)) and 20 participants from the control group (mean age 28.8 years (SD 5.3)) completed the 2-year study.
The mean value of WST in WR athletes at the beginning of the study was 71.3 (SD 4.7), and this significantly increased by 24.0%, whereas in the control group the mean value was 63.2 (SD 15.6), and this improved by 4.1%. The difference between the WR and control groups was 7.5% (95% CI = 0.7–15.5; p = 0.03) at the initial examination, and this increased by 28.0% (95% CI = 20.3–35.7; p < 0.001) at the final examination (Table I).
| Table I. Comparison of mean values of the Wheelchair Skills Test (WST) scores and the upper limb’s manual muscle test scores (American Spinal Injury Association (ASIA) motor score) in both groups | ||||
| WR group (n = 20) Mean (SD) | Control group (n = 20) Mean (SD) | |||
| I Term | II Term | I Term | II Term | |
| WST | 71.3 (4.7)† | 95.3 (2.5)†,* | 63.2 (15.6) | 67.3 (16.8)* |
| ASIA motor score | 20.7 (9.6) | 20.7 (9.6) | 22.9 (9.5) | 22.9 (9.5) |
| Significant differences: *p < 0.01 in comparison with I term (Wilcoxon’s signed-rank test); †p < 0.05 in comparison with the control group (Mann-Whitney U test). WR: wheelchair rugby. | ||||
According to ASIA classifications, in WR group there were 8 athletes with a C5, 5 with a C6, and 7 with a C7 level of neurological impairment. In the control group, 3 persons had a C5, 10 had a C6, and 7 had a C7 level of impairment.
The comparison of mean values of ASIA motor scores is shown in Table I. There were no differences between groups for ASIA motor scores at initial examination (p = 0.46). During the 2-year period, the ASIA score did not change in either group.
Fig. 1 presents the relationship between ASIA motor score and the differences in the initial and final WST scores. A significant negative Spearman’s correlation was found between changes in WST and ASIA score for the WR group showing larger improvements in participants with lower ASIA score (C5) compared with those with higher ASIA scores (C6–C7). By contrast, in the control group the improvement was highest among persons with C6 and C7 level of impairment. For 5 persons a maintenance of, and for 1 person, a decrease in, WST value was noted.
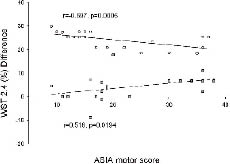
Fig. 1. Relationships between American Spinal Injury Association (ASIA) motor score and difference between final and initial Wheelchair Skills Test (WST) scores in wheelchair rugby (WR) group (circles) and control group (squares).
Discussion
The present study showed that 2 years’ participation in WR training resulted in significant improvements in the WST by patients with all levels of impairment of the spinal cord. The improvement was highest in patients with a C5 level of neurological impairment. Persons with tetraplegia who did not participate in sports training obtained poorer results in the WST after 2 years.
In our study, muscle strength, assessed with manual muscle testing according to the ASIA motor score, did not change in either group during the study. Similarly, Valent et al. (1) found no changes in upper-arm strength measured with the manual muscle test in patients with tetraplegia who were hand-cycling once a week or more for one year. However, Dallmeijer et al. (7) observed improvement in the maximal isometric strength performed on the ergometer in untrained persons after 3 and 6 months of quad rugby training. Therefore, the lack of changes in muscle strength observed in our study might be the result of poor sensitivity of the manual muscle test method. One of the factors that might have contributed to improvement of WST in persons from the WR group is the ability to learn new motor patterns during sports training. The capability to create new motor patterns under the influence of training among patients with SCI was shown in a study by Rodgers et al. (11). Moreover, Dallmeijer et al. (12) indicated an increase in motor ergonomics in persons after SCI. During their study, an improvement in motor precision, the symmetry and synchronization of motor patterns, and the optimal dosage of power under the influence of regular training was observed.
The abilities obtained during WR training (driving the wheelchair, controlling and passing the ball, blocking competitors) are reflected in the skills assessed during the WST. In this context, participants from the WR group significantly mastered motor patterns in groups of skills, such as reaching, rolling and turning. In addition, several groups of WST activities (obstacles, wheelies, folding/opening, transfers) were used to arrive at, and participate in, training by athletes. The repeatability of these skills may also influence performance in the final WST.
A major limitation of our study is the absence of randomization. This was partly because of the difficulty of selecting patients and partly the reduced willingness to participate in organized sports among persons after SCI. Persons with higher levels of functional abilities were more willing to attend physical training, whereas persons with lower levels preferred traditional rehabilitation programmes. This influences the interpretation of the results. However, higher progress in functional skills among persons participating in WR training, as seen in our study, can motivate people with a lower physical status to participate in organized sports.
In conclusion, during 2 years of study both groups improved their functional skills; however, the WR group obtained better results from the WST. The highest improvement in WST was observed among WR athletes with a C5 level of neurological impairment.
References

