OBJECTIVE: We aimed to investigate whether position sense acuity of the upper extremity and tracking performance, pen pressure and muscle activity in a tracking task are affected in subjects with neck and upper extremity pain.
METHODS: Twenty-three subjects with neck and upper extremity pain and 26 healthy controls participated in the study. Position sense acuity of the upper extremity was measured while subjects pointed at targets, without vision of their arm and hand. In the computer tracking task, subjects were instructed to position a cursor within a moving target dot, using a pen on a tablet.
RESULTS: Position sense acuity of the upper extremity was impaired in subjects with pain. Their variable error was 20–30% larger than in healthy controls. Subjects with pain also showed reduced tracking precision. Both the mean and the standard deviation of the distance to target were significantly larger in subjects with pain than in healthy controls, 10% and 13% respectively. No differences between groups were found in pen pressure and muscle activity during tracking.
CONCLUSION: The results suggest that subjects with pain are limited in performing precision tasks due to impaired position sense of the upper extremity, but do not compensate with increased effort.
Key words: pain; upper extremity; muscle activity; psychomotor performance; proprioception; kinaesthesis.
J Rehabil Med 2010; 42: 876–883
Correspondence address: Maaike A. Huysmans, VU Medical Centre, PO Box 7057, NL-1007 MB Amsterdam, The Netherlands. E-mail: m.huysmans@vumc.nl
Submitted October 1, 2009; accepted May 24, 2010
INTRODUCTION
Despite a large quantity of literature, the pathophysiology of non-specific neck and upper extremity pain, also referred to as repetitive strain injury (RSI), is poorly understood (1). It has been suggested that impaired proprioception plays an important role in the onset and perpetuation of RSI (2). Proprioception is the perception of movement or position of body parts in relation to each other. Its quality is mostly assessed by measuring the positioning accuracy of the limb, while vision of the limb is blocked. In subjects with symptoms similar to RSI, such as whiplash-associated disorders, chronic neck pain or epicondylitis, diminished position sense acuity in the neck, shoulder or elbow was found (3–6).
Proprioceptive information is important for motor control (7). If the quality of this information is diminished, it will be more difficult to perform precise movements. When precision demands in a task increase, healthy subjects increase the positional accuracy of their hand or handheld tool by increasing endpoint impedance, which is the resistance of the endpoint against imposed motion (8, 9). This can be done by increasing muscular co-activation in the arm and by increasing friction between the hand or input device and the underlying substrate, e.g. by increasing pen pressure (10, 11). If proprioception is indeed impaired in subjects with neck and upper extremity pain and, as a result of this, these subjects have more difficulty in performing precise movements, the question arises as to whether they compensate similarly for their impaired precision as healthy subjects do in response to increased task precision demands. If so, one would expect higher muscle activity levels for subjects with neck and upper extremity pain compared with healthy controls when working at similar precision levels. Increased muscle activity is thought to play an important role in the onset and perpetuation of neck and upper extremity pain (2).
Therefore, the present study, aimed to investigate whether proprioception is impaired in subjects with neck and upper extremity pain, by testing performance in a position sense acuity task and performance in a tracking task.
METHODS
Subjects
Twenty-three subjects with pain in the neck and upper extremity and 26 healthy controls participated in the study. Subjects were recruited through advertisements in a local newspaper and among employees of the university. All subjects were right hand dominant, and had normal or corrected to normal vision.
Subjects with pain were included in the study if they reported pain in the right neck–shoulder for at least 4 weeks in the last 3 months, 4 days in the last week and on the day of measurement. Subjects were not diagnosed with a specific (neurological) pathology and they reported no acute trauma, injury or birth defect that could have caused the pain. They all considered their pain to be work-related and reported working for at least 4 h per work day on the computer. Subjects were not on prescribed medication and were all working in spite of their pain when participating in the experiment. Pain intensity was scored on a 11-point numerical scale, ranging from 0 “no pain” to 10 “worst pain ever” (12). Disability of the subjects was measured with the Dutch version of the 30-item Disabilities of the Arm, Shoulder and Hand questionnaire, resulting in a score between 0 “no disability” and 100 “extreme disability” (13).
The healthy controls had no history of pain in the neck and upper extremities and no other musculoskeletal problems in the month prior to the day of measurement. They experienced no disabilities due to musculoskeletal problems.
For subject characteristics see Table I. Prior to participation subjects signed an informed consent. The study was approved by the medical ethics committee of the VU University Medical Center.
| Table I. General subject information for the subjects with pain and the healthy controls. t-test and χ2 results of the statistical differences between both subject groups. Skinfold thickness (in mm) is given of the skin above the M. extensor carpi radialis right (ECRr) and the M. trapezius pars descendens right (TDr) |
| | Subjects with pain | Healthy controls | Statistical test results |
| Number of subjects (n) | 23 | 26 | |
| Age, year, mean (SD) [range] | 43.0 (10.7) [24–61] | 42.4 (11.1) [24 – 62] | F(1,48) = 0.780 p = 0.781 |
| Gender, male/female, n | 4/19 | 4/22 | X2(1) = 0.036 p = 0.850 |
| Body height, m, mean (SD) [range] | 1.73 (0.10) [1.50–1.98] | 1.73 (8.7) [1.57–1.91] | F(1,48) = 0.016 p = 0.899 |
| Body weight, kg, mean (SD) [range] | 68.9 (14.9) [48 – 110] | 70.6 (12.1) [51–95] | F(1,48) = 0.410 p = 0.525 |
| BMI, kg/m2, mean (SD) [range] | 22.9 (4.1) [16.6–36.8] | 23.6 (4.2) [17.9–36.2] | F(1,48) = 0.519 p = 0.475 |
| Skinfold thickness above ECRr, mm, mean (SD) [range] | 7.6 (3.1) [3.0–14.0] | 7.5 (2.1) [3.5–11.5] | F(1,44) = 2.779 p = 0.103 |
| Skinfold thickness above TDr, mm, mean (SD) [range] | 14.4 (5.3) [5.0–23.5] | 15.81 (4.2) [8.0–21.5] | F(1,44) = 0.453 p = 0.504 |
| Location of the pain, n (%) Right neck-shoulder Right arm-wrist-hand Left neck-shoulder Left arm-wrist-hand | 23 (100%) 4 (17%) 7 (30%) 5 (23%) | | |
| Duration of the pain, years, mean (SD) [range] | 3.7 (2.8) [0.5-10] | | |
| Pain intensity, median [range] Worst pain in last 3 months Average pain in last 3 months Pain at day of measurement | 6 [3–10] 4 [2–9] 4 [1–10] | | |
| Disability, median [range] | 22.5 [10–45] | | |
| SD: standard deviation; BMI: body mass index. |
Position sense acuity task
In the position sense acuity task, subjects were standing, with their chin resting in a standardized position on a large digitizing tablet, which was placed upside down (Calcomp Digitizer Products, Columbia, USA, Drawingboard III, Model no. 34480, size: 0.92 × 1.22 m). On top of the tablet, a starting point and 3 target dots were visible (Fig. 1a). For the exact location of targets with respect to the starting point see Fig. 3. Subjects were instructed to point to the targets, under the tablet, with a pen held in their dominant hand, with the pen tip pointing upwards. The pen was held immediately below the pen tip with fingers folded around it (Fig. 1b), such that there was no tactile contact between fingers and tablet while pointing. Subjects could not see the pen or their arm and hand during the task. Each pointing movement was started in the starting point, located right in front of the subject. In order to guarantee that subjects started each pointing movement from the exact same position, a small piece of foam as attached underneath the tablet to guide the subjects to the correct position. From the starting point subjects had to point to 1 of the 3 targets, as verbally indicated by the experimenter. Subjects were instructed to make a pointing movement at a comfortable speed (not too fast), without touching the tablet. When they felt they had reached the position of the target, they touched the tablet with the pen tip. Contact between pen and tablet was signalled by a beep. After that they had to return to the starting point, to start a new pointing movement. Subjects practiced the task by making 10 pointing movements. When the procedure and pointing movements were clear to the subject and the movements were correctly performed, the actual measurement protocol was started. Each target was pointed at 20 times, and the order of the targets was randomized. After each block of 10 pointed targets, subjects took a rest break for 2 min to prevent fatigue.
Fig. 1. Measurement set up for the position sense acuity task. (a) Subjects rest their chin in the standardized position and see the starting point and the 3 targets on top of the tablet. (b) Subjects point at the targets under the tablet with a pen in their hand. (c) A typical example is given of the ellipse, fitted to the 95% confidence interval of 20 pointed targets (*) at the actual target. The variable error is defined as the area of the ellipse, calculated as π * major axis of the ellipse* minor axis of the ellipse.
Tracking task
For the tracking task, subjects were seated behind a desk. They had to use a pen on a small digitizer tablet (WACOM Europe GMBH, Krefeld, Germany, Intuos A4, Model: GD-0912-R) placed on the desk, while looking at a computer screen. Seat height and screen height were adjusted to the anthropometrics of the subject, to ensure that subjects sat with a knee angle of 90°, feet flat on the ground, upper arms vertical with relaxed shoulders and elbows flexed 90°. The forearm was supported by the arm rests of the chair. The tablet was centred in front of the subject, with the lower side at the edge of the table. The top of the computer screen was placed at eye height.
The task consisted of tracking a target dot, which moved quasi-randomly across part of the computer screen with a constant speed of 20 mm/s (Fig. 2). Subjects were instructed to keep the cursor (dot with a diameter of 1.9 mm) positioned as well as possible within the target dot by moving the pen on the tablet. The pen movement corresponded one to one with the cursor movement. Subjects started with performing 4 practice trials of 1 min each with a target dot of 12.8 mm in diameter. This was found to be enough to eliminate learning effects (14). Between the practice trials subjects rested for at least 3 min to prevent fatigue. Then, subjects performed 4 tracking trials with a duration of 2 min, 2 trials with a small target dot (ST, diameter 6.4 mm), and 2 trials with a large target dot (LT, diameter 19.2 mm). A different target trajectory was used for the experimental trials and the practice trials, to prevent subjects from recognizing the trajectory after several trials.
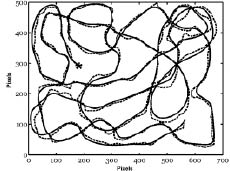
Fig. 2. The tracking trajectory of the experimental trials is shown as a solid line. An example of the position of the cursor is represented by the dashed line. The starting point is indicated with an asterisk.
Subjects were encouraged to explore different working techniques during the practice trials, but were instructed to chose a certain technique prior to the experimental trials and keep it constant during the experimental trials.
The order of the tracking trials was balanced across subjects, either ST-LT-ST-LT; ST-LT-LT-ST; LT-ST-LT-ST or LT-ST-ST-LT. In between the trials at least 5 min of rest was taken to prevent fatigue. During the tracking task, tracking performance, muscle activity of 8 muscles in the neck and upper extremities and axial pressure of the pen on the tablet were measured. Immediately after the task subjects were asked to rate their mental and physical perceived exertion. For each of the dependent variables the 2 trials for the small target and the 2 trials for the large target were averaged.
Data acquisition and analysis
Position sense acuity task. Horizontal and vertical coordinates of the pointed positions were collected with a spatial accuracy of 0.25 mm. Data points per target were fitted with an ellipse corresponding to the 95% confidence interval (CI), with the centre of the ellipse corresponding to the mean coordinates of the positions pointed at for each target. The variable error was defined as the area of the ellipse, i.e. π * major axis of ellipse (1.96*largest standard deviation (SD) of data points)* minor axis of ellipse (1.96*smallest SD of data points) (Fig. 1c).
Tracking task. The tracking task was programmed in LabVIEW (National Instruments Corporation, Austin, USA). The trajectory used in the experimental trials is illustrated in Fig. 2. In all experimental trials, the same trajectory was used, because the level of precision that can be achieved seems to be dependent on factors such as location and movement direction (15–17). Therefore, it appears that the level of difficulty cannot be fully standardized in random trajectories. Tracking performance proved to be highly reliable for this trajectory, with intraclass correlation (ICC) values higher than 0.92, and 4 practice trails were found to be enough to eliminate learning effects (14). The target moved within a window of 160 mm high and 220 mm wide on the computer screen. Horizontal and vertical position of the pen on the tablet was measured in tablet pixels, with a spatial accuracy of 0.25 mm, at a sample frequency of 100 Hz. After low-pass filtering the horizontal and vertical position of the pen with a 4th order Butterworth filter with a cut-off frequency of 12 Hz, the following measures were calculated using MATLAB (The MathWorks, Inc., Natick, USA):
• Percentage time on target (%TT), the percentage of the total number of samples for which the cursor was completely within the target.
• Mean distance to target (MDT), mean distance between the centre of the target and the centre of the cursor.
• Standard deviation of distance to target (SDDT), the standard deviation of the distance between the centre of the target and the centre of the cursor.
• Percentage lag (%lag), the percentage of the total number of samples for which the centre of the cursor was behind the midline of target (the line through the centre of target perpendicular to the target movement direction).
Pen pressure. Axial pressure of the pen on the tablet was measured with a sensitivity of 0.0036 N at a rate of 100 s–1 (the pen belonged to the digitizing tablet used; WACOM Europe GMBH, Krefeld, Germany, Intuos A4, Model: GD-0912-R). The cumulative probability distribution of the pen pressure during the 2-minute tracking trial was calculated. Subsequently, 3 percentiles were used to express the static level (P10), the median level (P50), and the peak level (P90) of pen pressure (18).
Muscle activity. Muscle activity was assessed of 8 muscles in the neck and upper extremities, i.e.:
• M. extensor carpi radialis right (ECRr) and left side (ECRl);
• M. flexor carpi radialis right (FCRr) and left side (FCRl);
• M. deltoideus pars clavicularis right side (DCr);
• M. deltoideus pars acromialis right side (DAr);
• M. trapezius pars descendens right (TDr) and left side (TDl).
To measure muscle activity, bipolar Ag/AgCl surface electrodes (Ambu®, Glen Burnie, USA, Blue Sensor electrodes, gel-skin contact area of 1 cm2), were positioned on the muscle bellies, according to the locations described by Basmajian (19) with an inter-electrode distance of 25 mm, after standard skin preparation. Location of the electrodes was confirmed by palpation of the muscle, while the subject performed a contraction against manual resistance, i.e. dorsal flexion and radial abduction of the wrist (ECRr and ECRl), palmar flexion and radial abduction of the wrist (FCRr and FCRl), anteflexion of the arm (DCr), abduction of the arm (DAr) and lifting the shoulders (TDr and TDl). At the location of the electrodes on the ECRr and TRr skinfold thickness was measured to the nearest 0.2 mm, using a Harpenden skinfold caliper. A reference electrode was placed on the C7 spinous process. Electromyography (EMG) signals were amplified 20 times (Porti-17TM, TMS, Enschede, The Netherlands, input impedance > 1012 Ω, CMRR > 90 dB), band-pass filtered (10–400Hz) and A-D converted (22-bits) at a sample rate of 1000 s–1. EMG signals were full-wave rectified and low-pass filtered at 5 Hz (4th order Butterworth) using MATLAB (The MathWorks, Inc., Natick, USA).
From these resulting signals, the cumulative probability distribution was calculated with the levels P10, P50 and P90, analogue to pen pressure (18).
Perceived exertion. Immediately after tracking, subjects were asked to rate their perceived mental exertion and their perceived physical exertion during tracking, using the Borg-scale. The Borg-scale is a 10-point scale with ratio properties ranging from 0 “not at all demanding” to 10 “very, very demanding” (20).
Statistical analysis
Differences between subjects with neck and upper extremity pain and healthy controls in age, gender, body height, and body weight were tested with t-tests and with a χ2 test. Dependent variables were all normally distributed as tested with Kolmogorov-Smirnov tests. Therefore, parametric statistics were used. Analysis of variance (ANOVAs) for repeated measures with subject group as a between-subject factor and target as a within-subject factor were used to test for differences between subjects with pain and healthy controls regarding the absolute and variable error in the position sense acuity test, tracking performance measures, pen pressure, muscle activity and perceived exertion. p-values less than 0.05 were considered statistically significant.
A 2-tailed Pearson’s correlation was used to determine the relation between position sense acuity measures (mean for the 3 targets) and tracking performance and kinematics measures for the small and the large target (mean for the 2 trials). Only the measures that were significantly different between subject groups were used in this analysis.
RESULTS
The t-tests and a χ2 test showed that subject groups were not different in terms of age, gender, body height, body weight, body mass index (BMI) and skinfold thickness (Table I).
Position sense acuity task
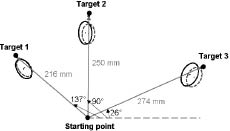
ANOVA for repeated measures revealed that the variable error was significantly larger for subjects with pain compared with the healthy controls (Table II and Fig. 3). The variable error, expressed by the area of the ellipse describing the 95% confidence interval of the pointed targets, was on average 20–30% larger for the subjects with pain.
| Table II. Means and standard deviations (SD) of position sense task performance and the statistical results of the analysis of variance (ANOVAs) for repeated measures to test the effects of target and subject group on position sense. |
| | Position sense task performance | Statistical test results |
| Subjects with pain Mean (SD) | Healthy controls Mean (SD) | Subject group | Target | Subject group × Target |
| Variable | Target 1 | Target 2 | Target 3 | Target 1 | Target 2 | Target 3 | F(2,94) | p-value | F(1,47) | p-value | F(1,94) | p-value |
| Variable error, mm2 | 62 (29) | 64 (29) | 81 (35) | 51 (19) | 52 (17) | 61 (31) | 5.091 | 0.029* | 9.023 | < 0.000* | 0.748 | 0.476 |
| * p < 0.05 | | | | | | | | | | | | |
Fig. 3. Mean ellipses of all subjects for the 3 targets. Ellipses with a solid line represent the data for the subjects with neck and upper extremity pain. Ellipses with a dashed line represent the data for the healthy control subjects. Also given are the distances between the starting point and the 3 targets and the angles between the line from the starting point to the target with the right horizontal.
Tracking task
ANOVA for repeated measures showed that MDT and SDDT were both significantly larger in cases than in controls. %TT and %lag were not different between subject groups (Table III). The interaction effect of group and target size was not statistically significant.
| Table III. Means and standard deviations (SD) of tracking performance measures; percentage time on target (%TT) mean distance between cursor and centre of target (MDT), standard deviation of the distance to target (SDDT) and percentage lag (%lag) for the small target (ST) and large target (LT) for the subjects with pain and the healthy controls. Statistical results of ANOVAs for repeated measures to test for the effects of subject group and target size on tracking performance. |
| Variable | Tracking performance | Statistical test results |
| Subjects with pain Mean (SD) | Healthy controls Mean (SD) | Subject group | Target | Subject group × Target |
| ST | LT | ST | LT | F(1,47) | p-value | F(1,47) | p-value | F(1,47) | p-value |
| %TT, % | 43.8 (12.7) | 98.2 (3.0) | 47.4 (9.4) | 99.4 (0.8) | 2.489 | 0.122 | 1370.791 | <0.001* | 1.100 | 0.300 |
| MDT, mm | 2.7 (0.6) | 3.3 (0.7) | 2.5 (0.3) | 3.0 (0.5) | 4.573 | 0.038* | 107.759 | <0.001* | 1.281 | 0.264 |
| SDDT, mm | 1.5 (0.4) | 1.8 (0.3) | 1.3 (0.1) | 1.6 (0.2) | 7.767 | 0.008* | 64.560 | <0.001* | 0.082 | 0.776 |
| %lag, % | 81.5 (6.6) | 70.7 (10.3) | 82.9 (6.5) | 75.0 (10.2) | 1.770 | 0.109 | 59.274 | <0.001* | 1.318 | 0.257 |
| * p < 0.05 | | | | | | | | | | |
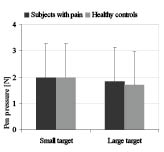
For pen pressure and muscle activity, the levels P10, P50 and P90 showed similar results. Therefore, only the analyses for the P50 values will be reported. ANOVAs for repeated measures showed that pen pressure and muscle activity in the different muscles were not significantly affected by subject group (Table IV). The interaction effects of group and target size were also not significant for pen pressure and muscle activity (Table IV and Figs. 4–5).
| Table IV. Statistical results of ANOVAs for repeated measures to test for the effects of subject group and target size on pen pressure and muscle activity in the M. extensor carpi radialis right (ECRr) and left side (ECRl), M. flexor carpi radialis right (FCRr) and left side (FCRl), M. deltoideus pars clavicularis right side (DCr), M. deltoideus pars acromialis right side (DAr), M. trapezius pars descendens right (TDr) and left side (TDl). |
| | Subject group | Target size | Group × target size |
| F(1,47) | p-value | F(1,47) | p-value | F(1,47) | p-value |
| Pen pressure | 0.306 | 0.552 | 15.599 | < 0.001* | 1.127 | 0.294 |
| ECRr | 2.786 | 0.102 | 27.856 | < 0.001* | 0.882 | 0.352 |
| ECRl | 0.723 | 0.399 | 17.872 | < 0.001* | 1.839 | 0.181 |
| FCRr | 0.237 | 0.629 | 39.181 | < 0.001* | 0.055 | 0.816 |
| FCRl | 0.388 | 0.536 | 19.341 | < 0.001* | 2.586 | 0.114 |
| DCr | 1.310 | 0.258 | 0.248 | < 0.001* | 1.4444 | 0.235 |
| DAr | 0.131 | 0.719 | 10.681 | 0.002* | 0.054 | 0.817 |
| TDr | 0.909 | 0.345 | 5.356 | 0.025* | 0.885 | 0.352 |
| TDl | 1.138 | 0.291 | 7.366 | 0.009* | 0.047 | 0.830 |
| * p < 0.05 | | | | | | |
Fig. 4. Pen pressure during tracking for subjects with neck and upper extremity pain and healthy controls. Values are given as means and standard deviations.
Fig. 5. Muscle activity in the M. extensor carpi radialis right (ECRr) and left side (ECRl), M. flexor carpi radialis right (FCRr) and left side (FCRl), M. deltoideus pars clavicularis right side (DCr), M. deltoideus pars acromialis right side (DAr), M. trapezius pars descendens right (TDr) and left side (TDl) during tracking, for subjects with neck and upper extremity pain and healthy controls for tracking the small target (ST) and for the large target (LT). Values are given as means and standard deviations.
ANOVA for repeated measures showed that perceived physical exertion was rated significantly higher by the subjects with pain, namely 5.8 (SD = 1.9) for the small target and 4.3 (SD = 1.9) for the large target, compared with, respectively, 3.5 (SD = 2.0) and 2.4 (SD = 1.3) for the healthy controls. There was no significant effect of subject group on mental exertion. On average subjects with pain rated their perceived mental exertion with 5.2 (SD = 2.2) for the small target and 3.3 (SD = 1.6) for the large target, while healthy controls rated their mental exertion with, respectively, 3.5 (SD = 2.0) and 2.4 (SD = 1.3). No interaction effect was present of subject group and target size.
Relation between position sense acuity and tracking performance
The variable error in the position sense acuity task was significantly different between subject groups. In the tracking task, differences between subject groups were found for MDT and SDDT. Therefore the 2-tailed Pearson’s correlation was used to determine the relation between the variable error of the position sense acuity task (mean for the 3 targets) and tracking performance measures; MDT and SDDT (mean value of the 2 trials for the small target and for the large target were tested separately). Significant correlations of 0.418 (p = 0.003) and 0.566 (p < 0.001) were found between the variable error and tracking performance measures MDT and SDDT, respectively, but only for the small target. For the large target no significant correlation between the variable error and tracking performance was found. The correlations were 0.237 (p = 0.105) for MDT and 0.280 (p = 0.054) for SDDT.
DISCUSSION
The present study aimed to investigate whether neck and upper extremity pain affects position sense acuity and performance, pen pressure, muscle activity and perceived exertion in a tracking task. Position sense acuity was found to be impaired in subjects with neck and upper extremity pain and these subjects showed lower tracking performance. Subjects with and without neck and upper extremity pain showed similar pen pressure and muscle activity levels during tracking. Nevertheless, subjects with neck and upper extremity pain perceived the tracking task as physically more demanding, whereas mental exertion was rated similarly in both subject groups. A significant correlation between position sense acuity and performance in the tracking task was observed.
In the position sense acuity task, the variable error, i.e. the area of the ellipse, was significantly larger in the subjects with neck and upper extremity pain. Where absolute errors give information about the current status of the calibration of position sense acuity, variability is a more suitable measure of the degree of noise within the information processing system (21).
In order to plan, prepare and execute a reaching movement, visual information about the position of the target and information about the current position of the hand and arm must be integrated. During visually guided reaching, the position of both the hand and the target are derived from a combination of visual and proprioceptive signals (22, 23). If the hand has not been visible during several movements (as in the present experiment), its position must be derived solely through proprioceptive information of arm muscles (24). For the visual localization of the target, retinal information needs to be combined with extra-retinal (e.g. proprioceptive) information about the orientation of the eyes in the head and of the head on the trunk. Therefore, in the position sense acuity task used in the present study, the variable error in pointing reflects the probability distributions for both the localization of the target and the proprioceptive localization of the hand (25). Since gaze direction and the initial hand position could also influence pointing errors (26), these were controlled in the present position acuity task. We did this by standardizing the position of the chin on top of the tablet and by asking subjects to gaze at the target before and during pointing. Moreover, all subjects had normal or corrected to normal vision. Therefore, it is not likely that the localization of the targets was different between subject groups and could explain the larger variable error found for patients. Consequently, the significantly larger ellipses for the subjects with pain seem to be the direct result of impaired proprioceptive information about either head orientation on the trunk or hand location, and thus position sense acuity seems to be impaired in subjects with pain. This is in line with the reduced repositioning accuracy reported for similar subject populations, such as subjects with chronic neck pain (3), whiplash disorders (4, 5) and lateral epicondylitis (6). For the head and neck in whiplash patients, Armstrong et al. (27) found no position sense impairment, but this may have been due to the fact that the whiplash patients in this study were less severely affected than those in the studies of Feipel et al. (4) and Sandlund et al. (5). The choice for testing position sense acuity in a multi-joint functional pointing task instead of testing it in a single joint repositioning task, was based on the fact that in everyday life information on hand position is more meaningful than joint angle information (16). It is likely that in the subjects with neck and upper extremity pain the affected proprioception is not limited to a single joint, similar to the fact that the pain is mostly not limited to a single joint in these subjects. In subjects with whiplash disorders, not only neck (3, 4), but also shoulder position sense (5) and elbow position sense (28) were affected.
Subjects with neck and upper extremity pain showed higher MDT and SDDT during tracking than healthy controls. This is in line with the larger distance to target as reported for subjects with pain in the arm, wrist and/or hand during tracking (15, 17) and the larger standard deviation of distance to target for subjects with fatigued arm muscles (14). In a tracing task, Jensen et al. (29) found no accuracy differences between subjects with upper extremity pain and controls, but it was not clear if the time to complete the task was standardized in this study. When movement time is not restricted, subjects with upper extremity pain have been reported to perform tasks slower (e.g. 30, 31). In the present study, the mean and standard deviation of tracking velocity were not different for the subjects with pain compared with the healthy controls.
Tracking performance measures MDT and SDDT were significantly correlated with position sense acuity while tracking the ST. However, the explained variances of 17% and 32%, respectively, were not high. It is likely that the visual feedback of performance in the tracking task, allows subjects partially to compensate the negative effects of impaired proprioception. An alternative explanation for the reduced performance in both tasks may be that the pain has competed with task demands for attention (32). However, this seems unlikely, since post-hoc analyses showed that pain ratings were not significantly correlated with task performance in either the position sense acuity task or the tracking task. Similarly, the DASH scores were not significantly correlated with task performance. Also, in the study of Sandlund et al. (33) in which subjects with non-specific neck pain had poorer repositioning acuity compared with healthy controls, no association was found between concentration difficulties and repositioning acuity. The larger errors in tracking were most likely not the result of a lack of motivation or a lack of effort, because subjects with and without neck and upper extremity pain showed similar muscle activity and pen pressure levels. It also seems unlikely that the reduced performance in the subjects with pain can be explained by fatigue. The tasks were rather short and long periods of rest were given between the trials. Even though these alternative explanations cannot completely be excluded, impaired position sense acuity seems the most likely explanation for the reduced performance in the position sense task.
Subjects with pain did not compensate for their lack of positional precision by increasing pen pressure or muscle activity. Static, median and peak levels of pen pressure and muscle activity were similar for subjects with pain and healthy controls. A study on aiming did reveal a more abrupt increase in pen pressure in subjects with neck and upper extremity pain compared with controls, but average pen pressure was not different (34). The effect of pain on muscle activity levels in published studies is not conclusive. Lower (35), similar (e.g. 32, 36) and higher trapezius muscle activity levels (37) have been reported for office workers with pain compared with those without pain. In the forearm extensors, similar muscle activity levels (32) and in the neck extensors, lower muscle activity levels (37) have been reported for symptomatic office workers. However, in most of these studies, performance or movement velocity was not measured or standardized, and different normalization procedures were applied, which complicates the interpretation and comparison of the muscle activity results. In the present study, we decided not to normalize muscle activity values, since we found different muscle activity levels during reference contractions for subjects with pain and controls, because of patients executing the reference contractions differently, most likely because they tried to avoid pain. Differences between patients and controls for maximal and sub-maximal contractions have been reported previously (35, 38) and normalizing task EMG to these values will introduce bias, and thus impair validity. Not normalizing may result in a loss of statistical power because of larger variation due to the between-subject variability caused by differences in the thickness and electrical properties of the tissue between the muscle and the electrode (39). Even though validity problems cannot be fully excluded when using non-normalized EMG data, they are not likely to be present in the current study. The larger between-subject variation due to not normalizing the EMG data is expected to be random and similar for the subjects with pain and the controls, since groups did not differ in gender, age, BMI and skin thickness above the muscle. Therefore, we preferred the loss of power above the introduction of bias, which would have resulted from normalizing EMG results to maximal or sub-maximal values. Since no tendencies were found for an effect, and the number of subjects in the present study should provide sufficient statistical power, despite using non-normalized data (40), we do not expect different outcomes if more subjects were to be tested. However, the possibility that the absent group difference in muscle activity can be explained by low precision due to using non-normalized EMG values cannot be fully excluded.
Increased muscle activity is thought to play an important role in the onset and perpetuation of neck and upper extremity pain (2). It has been suggested that, as a result of fatigue and/or cell damage, metabolites are released in the muscle, which leads to a decrease in proprioceptive acuity, as well as pain. The negative effects of impaired proprioception on motor control can be counteracted by an increase in muscle activity. This is thought to initiate a vicious cycle, as a higher muscle activity will accelerate metabolite accumulation. However, contrary to what is expected in this model (2), we did not find a higher muscle activity in subjects with neck and upper extremity pain. This implies that the vicious cycle is not closed, possibly because reduced performance on the task had no consequences for the subject, and therefore, this patho-physiological model was not supported. Because of the cross-sectional nature of the study we can only speculate whether the impaired position sense is the cause or the effect of the pain. It is recommended to investigate position sense acuity in a longitudinal study in order to get more insight in its role in the development of neck and upper extremity pain.
The subjects with pain in the present study were included without applying strict inclusion criteria, except for presence and duration of self-reported pain in the neck and right shoulder. This resulted in a subject population which was heterogeneous in terms of pain intensity, lateralization of the pain, and disability. Stricter inclusion criteria were not applied, since no specific diagnosis can be made in the majority of patients with neck and upper extremity pain (41) and little evidence exists to define specific sub-groups within this population (42). This may have reduced the power of the study to detect effects, which were nevertheless found. However, the differences between subject groups in the position sense acuity and the tracking task were rather small and one can question the clinical relevance of these differences. Moreover, the tasks used were highly standardized and position of the arm and pointing direction in the position sense acuity task were different from those in most daily tasks. Nevertheless, we expect that the results can be generalized to practice, in that subjects with neck and upper extremity pain are likely to have more difficulty with tasks demanding a high level of precision. Since many work situations and everyday tasks depend on high precision, even small increases in movement and positional variability can have implications for an individual’s everyday functioning. If allowed, subjects with pain are likely to reduce their movement velocity in response to high precision demands, but if movement velocity is imposed and there are no direct consequences of working less accurately, as in the present study, their level of precision will probably be reduced. If both movement velocity and precision are imposed, subjects with pain are possibly forced to increase physical exertion or fail to perform the task. In this way impaired position sense acuity and positional precision could increase disability levels in subjects with pain in neck and upper extremity. Brouwer et al. (15, 17) have indeed shown that impaired precision in tracking was positively related to disability score and impairment level.
We conclude that position sense acuity and tracking performance are impaired in subjects with neck and upper extremity pain. Performance in both tasks was related, which suggests that the reduced tracking performance can be explained by the impaired position sense. Unfortunately, alternative explanations for the reduced performance in the position sense task and the tracking task, such as attentional deficits, motivational problems and fatigue, could not completely be excluded. Subjects with neck and upper extremity pain did not compensate for their reduced tracking performance by increasing pen pressure or muscle activity. Despite similar pen pressure and muscle activity levels to those of healthy controls, subjects with neck and upper extremity pain perceived the tracking task as physically more demanding.
REFERENCES