OBJECTIVE: To use the International Classification of Functioning, Disability and Health (ICF) to describe and compare patient-reported disability in Guillain-Barré syndrome survivors and persons with multiple sclerosis, and to identify relevant environmental factors.
METHODS: Cross-sectional survey of 77 survivors of Guillain-Barré syndrome in the community. Their Guillain-Barré syndrome-related problems were linked with ICF categories (second level) using an open-ended questionnaire, consensus between health professionals and the “linking rules”, and compared with similar data collected previously for 101 persons with multiple sclerosis.
RESULTS: Guillain-Barré syndrome survivors were male (59%) and older than persons with multiple sclerosis (mean age 55 vs 49 years). Of 170 ICF categories, 113 were relevant for Guillain-Barré syndrome survivors (mean number 30 vs 18 for persons with multiple sclerosis). The linked categories for Guillain-Barré syndrome included: body function 27 (56%) compared with 48 (42%) for persons with multiple sclerosis; body structure 11 (68%) vs 16 (34%); activities and participation 48 (70%) and 68 (58%); and for environmental factors 27 (71%) compared with 38 (51%) for persons with multiple sclerosis. The main areas linked in the activities and participation domain were mobility, major life areas and interpersonal relationships; and environmental factors included support and relationships, attitudes and products and technology.
CONCLUSION: This is the first study to use ICF in Guillain-Barré syndrome survivors and towards development of the ICF Core Set for Guillain-Barré syndrome from a broader international perspective.
Key words: ICF; disability; multiple sclerosis; Guillain-Barré syndrome; outcome assessment; environmental factors.
J Rehabil Med 2010; 42: 708–714
Correspondence address: Fary Khan, Department of Medicine, Dentistry and Health Sciences, The University of Melbourne and Director of Rehabilitation Medicine, Royal Melbourne Hospital, Poplar Road Parkville, Melbourne VIC 3052, Australia. E-mail: fary.khan@mh.org.au
Submitted October 25, 2009; accepted May 27, 2010
Introduction
Guillain-Barré syndrome (GBS) (acute inflammatory demyelinating polyradiculopathy) is an immune-based illness that presents as an evolving acute polyneuritis, usually with motor features such as progressive symmetrical ascending paralysis (1, 2). GBS can occur at any age (it is most common between 30 and 50 years of age), affects both sexes, with a worldwide annual incidence of 1–2 per 100,000 (3). It is a significant cause of new long-term disability, affecting almost 1000 persons in the USA and 1500 in the UK annually (4). GBS is associated with high mortality and morbidity. In the acute phase of GBS, approximately 3% of patients may die due to acute complications (5); and 12 months later up to 20% have residual permanent severe disability, with deficits in ambulation, or require ventilator assistance (4). The impact of GBS on activities of daily living, work, social activities and quality of life (QoL) is considerable at 2 years after onset and probably persists beyond this time-point (6). Furthermore, reduction in leisure and social activities was reported in 44% of GBS survivors (7); and ongoing detrimental impact upon their and their carers’ lives was reported in 62% even 3–6 years later (1). Despite this, the patient perspective and long-term neurological sequelae of GBS have not been well studied (8).
Multiple sclerosis (MS) is a chronic progressive demyelinating disease of the central nervous system that affects approximately 2.5 million persons worldwide. There are more women than men with MS (3:1 ratio). Most persons with MS are diagnosed in early adulthood and it is a major cause of disability in young adults. Like GBS survivors, persons with MS have considerable morbidity and a detrimental impact on QoL. The impact of MS on disability, carer burden, QoL, vocational and economic issues on persons with MS have been reported extensively (9–13).
The National Services Framework (NSF) (14) for long-term neurological conditions (LTNC) aims to improve health and social care services, and QoL for persons with LTNC, by ensuring coordinated individualized care and support based on their needs. This framework classifies GBS as a “sudden onset” LTNC and MS as a “progressive” LTNC. It is very likely that neurological patients with various LTNC may have many similar areas of disability and care needs; and similar environmental factors that may influence their level of disability and participation. This, however, has not been explored previously.
The International Classification of Functioning, Disability and Health (ICF) (15), defines a common language for describing the impact of disease at different levels. The ICF framework therefore has the ability to capture “functioning” in both patient populations irrespective of the underlying health condition, and may provide valuable information about the patient-reported limitation in activity and participation. Furthermore, the identification of environmental (physical, attitudinal and policy) barriers that impact GBS survivors and persons with MS, and their adaptation may then meet the unique needs of these persons.
The use of ICF has been previously well described for persons with MS (16, 17), but not in the GBS population. Within this classification the GBS-related impairments (muscle weakness, dysphagia), can limit “activity” (decreased mobility and self-care, pain) and “participation” (work, family, social reintegration). Similar to persons with MS, these limitations have a cumulative effect over time and cause considerable distress, not only to GBS survivors, but also to their families, resulting in reduced QoL. There are significant cost and socioeconomic implications with increased demand for healthcare, social and vocational services. This is especially important given the high incidence of GBS amongst the young age population (2, 8).
The objectives of this study were to compare patient-reported disability in 2 LTNCs; a GBS and an MS community cohort using the ICF; and to identify relevant environmental factors. This study will provide information regarding relevant health areas for GBS survivors compared with data previously collated for persons with MS.
Methods
Participants and setting
This study included a cross-sectional survey of persons residing in the community with a confirmed diagnosis of GBS. A clinical audit at the Royal Melbourne Hospital (RMH), a tertiary referral centre in Victoria, Australia, identified 157 consecutive patients admitted for acute care in the period 2000–08. These patients had a primary diagnosis of ICD Code (G61.0) for GBS (first admission only). The RMH Access Database was used for cross-indexing of diseases from HOMER (a RMH patient administration database), using the Hospital Information Services of the Department of Health Victoria. The source of these patients was a pool of persons residing in the community, referred to the RMH from public and private medical clinics across greater Melbourne in Victoria. This study was approved by the Human Research and Ethics Committee at the RMH.
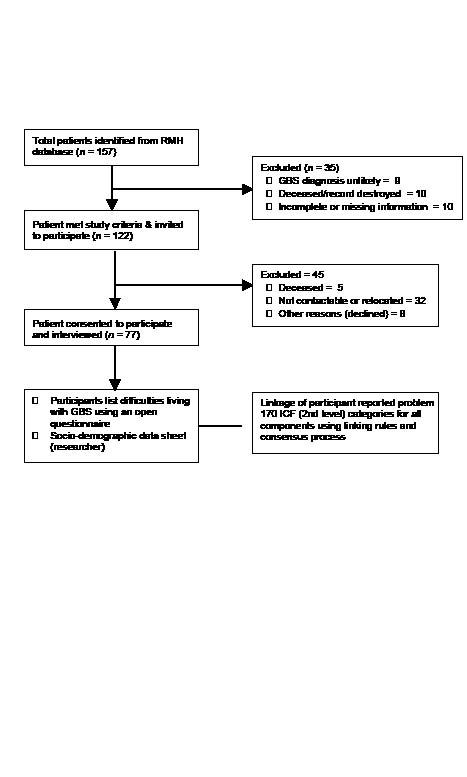
All patients identified were reviewed and assessed by an independent neurologist (in person) at the RMH. They had a confirmed diagnosis of GBS based on standard diagnostic criteria defined by the National Institute of Neurologic Disorders and Stroke clinical criteria (3). These participants were aged between 18 and 65 years of age at onset of GBS, resided in the community, and had known limitations in their neurological status (including mobility) at admission and discharge from RMH, representing the entire spectra in GBS from mild to severe disease. GBS survivors who were unable to be traced or contacted due to various reasons were excluded (Fig. 1), as they were unavailable.
Fig. 1. Recruitment process for study of Guillain-Barré syndrome (GBS). ICF: International Classification of Functioning, Disability and Health; RMH: Royal Melbourne Hospital.
The recruitment and selection of persons with MS (n = 101) was reported previously (10, 11, 13, 16). This community cohort included more females than males (3:1 ratio), aged between 18 and 65 years with definite MS, and comprised all MS disease stages. Disability was measured using the Expanded Disability Status Scale (EDSS) scores (mobility score range 2–8 and cognition Kurtzke Functional System score 0–2) (11, 16).
Data collection procedures and measurement
At the time of recruitment 122 of 157 GBS patients listed on the RMH GBS Database were eligible for this study due to entry criteria. All were invited by post to participate in the study and the 77 who consented were recruited for the project (flowchart Fig. 1). All interviews were conducted by a trained research assistant and a physician who participated in 3 half-day structured ICF workshops at RMH. This involved education about the model and core ICF principles, and practical application and linkage rules for ICF.
Each participant was interviewed using a structured format and asked to nominate a list of the problems affecting their everyday life due to GBS (open questionnaire available from authors). There was no prompting or use of GBS problem lists. The information provided was checked and clarified with the patient medical record, RMH database and, where possible, with carers. Any discrepancies were resolved with discussion (with the participant) and consensus agreement between reviewers. Each problem reported by GBS survivors was then linked with the ICF checklist of 170 from the 362-second level categories of the whole ICF classification system. This checklist was identical to that used for persons with MS in our previous report (16), and incorporated the 125 categories in the World Health Organization (WHO) checklist (18) and another 45 added ICF categories that linked with the MS participant answers (available from authors). With regards to all categories in the second level of the ICF, this checklist included 48 (42%) categories from the component body function, 16 (34%) from body structure, 68 (58%) from activities and participation and 38 (51%) from environmental factors. Barriers (hindrances) were identified as a major influence on a persons’ ability to engage in activity, participation and good health practices.
Health professionals trained in ICF used the linking rules to match each problem reported by the participant with an appropriate code from the ICF categories (second level). All problems pertaining to personal factors currently not coded within the ICF were grouped under “personal factors”. Consensus between reviewers was used to decide which categories should be linked to each answer. After data extraction, both reviewers compared their results. Any disagreements concerning selected categories and codes were resolved by a trained third health professional (LN).
Information relating to participant socio-demographic and disease status was collated using a standard data form.
Statistical methods
Descriptive analysis was used to describe the study population. The frequency of participant-reported problems due to GBS were linked with the ICF categories (second level), and compared with categories linked for persons with MS (16).
The frequency of participants reporting limitation in the categories for the component “Activities & Participation” are presented. For environmental factors, the frequencies of persons reporting a specific category as a barrier are reported.
If the patient repeatedly assigned one ICF category, it was counted only once to avoid bias. Consensus opinion was used if there was a discrepancy in the GBS-related problem listed by the participant and their carer. Carer report was included in the information used to link ICF categories for problems listed by the GBS survivor. All data was entered twice to avoid errors on data entry. SPSS 17.0 for Windows was used for analysis.
Results
The socio-demographic and disease characteristics of the GBS survivors (n = 77) are shown in Table I. The GBS cohort compared with the persons with MS were slightly older (median age: GBS 55 years, persons with MS 49 years), had a shorter disease duration (median GBS 6 years, persons with MS 10 years) and included more men (GBS: 59%, persons with MS: 28.7%). The mean number of problems reported by the GBS participant was 30 (range 3–65), compared with the mean number of problems reported by persons with MS at 18 (range 8–30) (detailed data for persons with MS has been reported previously (16). There was 100% agreement between reviewers for linkage of participant-reported problems with the ICF categories.
| Table I. Socio-demographic and clinical characteristics of Guillain-Barré syndrome (GBS) survivors at initial presentation |
| Characteristics | n = 77 |
| Male, n (%) | 46 (59.7) |
| Age (years) median (IQR) | 56 (18.4–65.5) |
| Disease duration (years) median (IQR) | 6 (2.9–10) |
| LOS acute (days), median (IQR) | 9.5 (5–50) |
| Intensive care unit admission, n (%) | 18 (23.4) |
| Non-invasive ventilation, n (%) | 13 (16.9) |
| LOS subacute (days), median (IQR) | 63.5 (23–131) |
| Facial weakness, n (%) Mild Moderate Severe | 10 (13.0) 10 (13.0) 5 (6.5) |
| Dysarthria, n (%) Mild Moderate Severe | 9 (11.7) 5 (6.5) 1 (1.3) |
| Dysphagia, n (%) Mild Moderate Severe | 5 (6.5) 3 (3.9) 4 (5.2) |
| Ophthalmoplegia, n (%) Mild Moderate Severe | 4 (5.2) 4 (5.2) 3 (3.9) |
| Urinary dysfunction, n (%) | 13 (16.9) |
| Bowel dysfunction, n (%) | 12 (15.6) |
| Autonomic dysfunction, n (%) | 8 (10.4) |
| Pain, n (%) | 46 (59.7) |
| Sensory loss – spinothalamic, n (%) | 34 (44.2) |
| Sensory loss – dorsal column, n (%) | 26 (33.8) |
| Electrophysiological data consistent or possible with GBS, n (%) | 47 (62.7) |
| Treatment received, n (%) Plasma exchange IVIG Steroid – IV Steroid – oral | 18 (23.4) 61 (79.2) 8 (10.4) 10 (13.0) |
| Discharge destination n (%) Community (home/family member) Rehabilitation Acute transfer | 35 (45.5) 35 (45.5) 7 (9.1) |
| LOS: length of stay; LOV: length of ventilation; IV: intravenous; IVIG: intravenous immunoglobulin; IQR: interquartile range. |
Tables II–V show the frequency of limitations in categories reported by at least one-third of the GBS participants (for each category), linked with the ICF categories for all 4 components: “body function”, “body structure”, “activities and participation” and “environmental factors”. The comparative frequency of each category for persons with MS reported by at least one-third of participants is also presented.
| Table II. International Classification of Functioning, Disability and Health (ICF) – Frequency of limitation in the linked categories for the component “body function” reported by at least one-third of the Guillain-Barré syndrome (GBS) participants compared with persons with multiple sclerosis (MS)1 |
| ICF Code | ICF Code description | Total number of participants linked responses, n (%) |
| GBS (n = 77) | MS (n = 101) |
| b130 | Energy and drive functions | 51 (66.2) | 98 (97.0) |
| b134 | Sleep | | 84 (83.1) |
| b140 | Attention | | 66 (65.3) |
| b144 | Memory | | 62 (61.4) |
| b152 | Emotional functions | | 97 (96.0) |
| b210 | Seeing | | 47 (46.5) |
| b235 | Vestibular (incl. Balance functions) | 39 (50.6) | 71 (70.3) |
| b265 | Touch2 | | 34 (33.7) |
| b280 | Sensation of pain | 34 (44.2) | 76 (75.2) |
| B455 | Exercise tolerance functions2 | 67 (87.0) | 97 (96.0) |
| b525 | Defecation | | 89 (88.1) |
| b620 | Urination functions | | 94 (93.1) |
| b640 | Sexual functions | | 57 (56.4) |
| b730 | Muscle power | 62 (80.5) | 96 (95.1) |
| b735 | Muscle tone | | 94 (93.1) |
| b740 | Muscle endurance function2 | 74 (96.1) | 93 (92.1) |
| b760 | Control of voluntary movement functions2 | | 66 (65.3) |
| b770 | Gait pattern functions2 | 62 (80.5) | 99 (98.0) |
| 1MS data source: Khan & Pallant (16). 2Categories added to the ICF (checklist version 2.1a) (18) after linkage of participant responses. |
| Table III. International Classification of Functioning, Disability and Health (ICF) – Frequency of limitation in the linked categories for the component “body structure” reported by at least one-third (33%) of Guillain-Barré syndrome (GBS) participants compared with persons with multiple sclerosis (MS)1 |
| ICF Code | ICF Code description | Total number of participants linked responses, n (%) |
| GBS (n = 77) | MS (n = 101) |
| s110 | Brain | 63 (81.8) | 100 (99.0) |
| s610 | Urinary system | | 93 (92.1) |
| s730 | Upper extremity (arm, hand) | 31 (40.3) | 44 (43.6) |
| s750 | Lower extremity (leg, foot) | 61 (79.2) | 97 (96.0) |
| s760 | Trunk | | 85 (84.2) |
| 1MS data source: Khan & Pallant (16). |
| Table IV. International Classification of Functioning, Disability and Health (ICF) – Frequency of limitation in the linked categories for the component “activities and participation” reported by at least one-third (33%) of Guillain-Barré syndrome (GBS) participants compared with persons with multiple sclerosis (MS)1 |
| ICF Code | ICF Category description | Total number of participants linked responses. n (%) |
| GBS (n = 77) | MS (n = 101) |
| d160 | Focusing attention2 | 26 (33.8) | 70 (69.3) |
| d175 | Solving problems | | 34 (33.6) |
| d177 | Making decisions2 | 26 (33.8) | 59 (58.4) |
| d220 | Undertaking multiple tasks | 40 (51.9) | 88 (87.1) |
| d230 | Carrying out daily routine2 | 48 (62.3) | 80 (79.2) |
| d240 | Handling stress and other psychological demands2 | 36 (46.8) | 101 (100.0) |
| d430 | Lifting and carrying objects | 37 (48.1) | 53(52.5) |
| d440 | Fine hand use (picking up, grasping) | 41 (53.2) | 51 (50.5) |
| d445 | Hand and arm use2 | 31 (40.3) | 37 (36.6) |
| d450 | Walking | 47 (61.0) | 101 (100.0) |
| d455 | Moving around2 | 53 (68.8) | 99 (98.0) |
| d465 | Moving around and using equipment (wheelchair, skates, etc.) | | 98 (97.0) |
| d470 | Using transportation (car, bus, train, plane, etc.) | 58 (75.3) | 100 (99.0) |
| d475 | Driving (riding bicycle and motorbike, driving car etc.) | 56 (72.7) | 99 (98.0) |
| d510 | Washing oneself (bathing, drying, washing hands, etc.) | | 41 (40.6) |
| d520 | Caring for body parts (brushing teeth, shaving, grooming, etc.) | | 40 (39.6) |
| d570 | Looking after one’s health | 31 (40.3) | 88 (87.1) |
| d620 | Acquisition of goods and services (shopping, etc.) | | 92 (91.1) |
| d630 | Preparation of meals (cooking etc.) | 32 (41.6) | 89 (88.1) |
| d640 | Doing housework (cleaning washing, laundry, ironing) | 51 (66.2) | 94 (93.1) |
| d650 | Caring for household objects2 | | 84 (83.2) |
| d660 | Assisting others | 27 (35.1) | 87 (86.1) |
| d720 | Complex interpersonal interaction | 40 (51.9) | |
| d750 | Informal social relationships | | 35 (34.6) |
| d760 | Family relationships | 56 (72.7) | 73 (72.2) |
| d770 | Intimate relationships | 31 (40.3) | 61 (60.40) |
| d845 | Acquiring keeping and terminating a job2 | 40 (51.9) | 73 (72.2) |
| d850 | Remunerative employment | 38 (49.4) | 90 (89.1) |
| d865 | Complex economic transanction | 28 (36.4) | |
| d870 | Economic self-sufficiency | 55 (71.4) | 84 (83.2) |
| d910 | Community life | 39 (50.6) | 79 (78.2) |
| d920 | Recreation and leisure | 71 (92.2) | 97 (96.0) |
| 1MS data source: Khan & Pallant (16). 2Categories added to the ICF (checklist version 2.1a) (18) after linkage of participant responses. |
| Table V. International Classification of Functioning, Disability and Health (ICF) – Frequency of limitation in the linked categories for the component “Environmental factors” reported by at least one-third (33%) of the of Guillain-Barré syndrome (GBS) participants compared with persons with multiple sclerosis (MS)1 |
| ICF Code | ICF Code description | Total number of participants linked responses n (%) |
| GBS (n = 77) | MS (n = 101) |
| e110 | For personal consumption (food, medicines) | | 101 (100.0) |
| e120 | For personal indoor and outdoor mobility and transportation | 66 (85.7) | 91 (90.1) |
| e150 | Design, construction and building products and technology of buildings for public use | | 70 (69.3) |
| e210 | Physical geography | | 39 (38.6) |
| e225 | Climate | | 99 (98.0) |
| e310 | Immediate family | 36 (46.8) | 45 44.5) |
| e315 | Extended family | 41 (53.2) | 42 (41.6) |
| e415 | Individual attitudes extended family | 28 (36.4) | |
| e460 | Societal attitudes | | 31 (30.7) |
| e540 | Transportation services, systems and policies | 33 (42.9) | 68 (67.3) |
| e580 | Health services, systems and policies | 64 (83.1) | 79 (78.2) |
| 1MS data source: Khan & Pallant (16). 2Categories added to the ICF (checklist version 2.1a) (18) after linkage of participant responses. |
Previously, problems reported by persons with MS were linked to a total of 170 ICF categories (16); these were compared with problems reported by GBS survivors linked with ICF categories. Of these, 113 (66.5%) were relevant to GBS survivors and no additional categories were identified by the GBS cohort. In the “body function” component, problems identified by the GBS survivors were linked to 27 ICF categories (of 48 ICF categories (56%)). They reported limitation in at least one of the categories of the chapters: mental function (66% –b130 energy and drive) and function of cardiovascular system (87% –b455 exercise tolerance function); and 3 categories were linked for neuromuscular and movement related functions (80% each for b730 – muscle power and b770 – gait pattern function; and 96% in b740 – muscle endurance function). In comparison with GBS survivors, at least 90% persons with MS reported limitation in at least one category of the above chapters including genitourinary and reproductive function. For persons with MS, in the component “body function”, 10 categories each were selected for mental function, and neuromuscular and movement related functions, sensory function and pain (6 categories each) and genitourinary functions (5 categories) (16).
The problems named by the patients in the component “body structure” were linked to 11 ICF categories (out of 16 ICF categories (68%)). Thirty-one (40%) and 61 (79%) of GBS survivors reported involvement of upper extremity (s730) and lower extremity (s750), respectively. In contrast, 93 (92%) persons with MS had reported structure of genitourinary system (s610).
The problems highlighted by the patients were linked with ICF categories across the 9 chapters of the “activities and participation” component and included 68 categories. Of these, 48 (70%) categories were relevant for GBS survivors with reported limitation. The main areas linked: mobility (8 categories), learning and applying knowledge (3 categories), major life areas such as employment (3 categories), and interpersonal relationships (4 categories). In contrast, for persons with MS the problems identified were linked with ICF categories in all 9 chapters of the “activities and participation” component (68 categories). The main areas linked were: mobility (11 categories), learning and applying knowledge (10 categories), and major life areas such as employment (9 categories), and interpersonal relationships (7 categories).
The problems listed by persons with MS in the “environment” component were linked with 38 ICF categories; of these, 27 (71%) were also identified as barriers by the GBS survivors. These included: systems and policies (2 categories compared with 11 for persons with MS); support and relationships (2 categories compared with 8 for persons with MS); and for attitudes and products and technology (1 category each compared with 6 for persons with MS).
Discussion
This is the first study to use ICF to compare patient-reported disability in 2 different LTNCs: GBS survivors and persons with MS in a community cohort; and to identify relevant environmental factors. Clinically, patients with different LTNCs may report similar problems that impact everyday life (e.g. mobility, self-care, continence). The comparison of patient-reported problems in different neurological populations, however, is now possible using the ICF framework, as it can highlight “functioning” irrespective of the underlying health condition. In this study, problems highlighted by both GBS survivors and persons with MS linked to specific ICF categories show overlapping domains in activity limitation and restriction in participation. These have the potential to allow clinicians to provide targeted intervention to facilitate communication, assessment and management of these persons across settings and interventions (19).
Previously the International Classification of Impairments, Disabilities and Handicaps (ICIDH) model in patients with immune polyneuropathies found significant associations between its various levels (20), where the combined impairment and disability scales accounted for 77% of the variance in handicap (participation). However, other variables not accounted for in this model included psychosocial factors (such as anxiety, and depression), which contributed to persistent disability, in addition to muscle weakness, sensory dysfunction and fatigue (21, 22). The ICF therefore provides an improved framework and additional information, as it integrates the conceptual factors.
This study highlights the long-term neurological sequelae in GBS survivors, which have not been well studied in the literature. Of the 170 ICF categories previously identified for persons with MS, 113 (66%) were relevant for GBS survivors. This is not surprising, as MS is a “progressive” LTNC causing many disabilities that have a cumulative effect over time, while GBS is a “sudden onset” LTNC and patients are usually expected to make a much greater degree of recovery.
In the “body function” domain 66% of GBS survivors reported limitation in mental function (b130 energy and drive), as reported previously (23, 24). As the median disease duration in GBS participants was 6 years, the report of ongoing lack of energy and fatigue is significant, and requires further study. In contrast, MS fatigue and “lack of energy” reported by 97% of the MS cohort is well documented (11, 25).
Although prevalence of anxiety and depression in persons with MS has been published widely (10–12), few longer-term studies exist in the GBS population (21, 22). Psychosocial dysfunction (including emotional problems) can occur in GBS survivors 6 years later, even in those with minimal physical deficits (22). A 6-month follow-up study of GBS survivors reported significant limitation in energy, emotional reactivity, sleep, pain and social isolation (compared with controls); and identified female gender, lower education status and social isolation as factors associated with tendency to depression (24). Other reports of GBS patients in intensive care settings report high levels of anxiety (82%) and depressive episodes (67%) (26); these, however, were associated with severe tetraparesis, mechanical ventilation and cranial nerve dysfunction (26). In this GBS cohort a lower number (n = 18) required intensive care. Furthermore, over time they may have altered their functional expectations – the “response shift phenomenon”; similar to a recent report in persons with MS (13). More studies are needed to understand factors contributing to mood disorders and response shift phenomenon in the GBS population.
Various types of pain have been studied extensively in the MS population (27). Up to 70% of GBS survivors in acute settings can develop musculoskeletal and neuropathic pain (28). To our knowledge, there are no longer-term studies of pain in the GBS population. The identification of factors associated with fatigue, depression and/or pain in this GBS cohort, however, was beyond the scope of this preliminary study. Other areas of reported limitation include exercise tolerance, muscle power and movement-related functions in the GBS population, which have been reported previously (4, 20, 28), as is also the case in the MS population (29, 30).
In contrast with persons with MS (31), those with GBS did not report genitourinary or sexuality issues, and this needs further investigation. Although GBS affects the peripheral nervous system, up to 30% of GBS survivors can develop disturbed bladder sensation and areflexia (32). These conditions, however, usually resolve over time. This GBS cohort had a median time since diagnosis of 6 years, and it is possible that any bladder dysfunction may have resolved. Approximately 30% of GBS patients develop urinary infections acutely (33). All participants in the study were monitored regularly over the years by their general practitioner and received treatment as required. GBS survivors may also develop detrusor hyperactivity over time, which may persist many years after GBS (personal communication: Professor C. Fowler, National Hospital for Neurology and Neurosurgery, UK); however, currently there are no longer-term studies of bladder dysfunction in the GBS population.
A large number of patient-reported problems were linked to categories for “activities and participation”, as both MS and GBS impact on many aspects of everyday life. The relevant domains include: mobility, learning and applying knowledge, domestic life, inter-personal, family and intimate relations. These areas are similar to those reported by patients with chronic conditions (stroke, diabetes, arthritis) and mental health conditions (depression) (34). Many of the linked categories in the above domains are consistent with other reports in the literature for persons with MS (35); however, these domains have not been well documented for the GBS population (8). For example in the domain learning and applying knowledge, 33% of GBS survivors reported difficulty focusing attention and making decisions, and related this to their fatigue levels; this needs further investigation. One report (36) highlights changes made by GBS survivors 5 years later in their jobs, hobbies or social activities despite near complete functional recovery. Furthermore, the GBS participants highlighted limitation in major life areas (economic self-sufficiency, remunerative employment) similar to the report in the MS cohort (16). Although this is in keeping with other studies in MS (9), no such studies currently exist for the GBS population, and further research is needed.
Other environmental categories linked for both GBS survivors and persons with MS, such as products of technology for use for mobility and transportation, and access to health services were also reported by patients with chronic conditions (16, 34). Unlike persons with MS, climate was not highlighted by GBS survivor. The limited access to healthcare services and systems reported by GBS survivors was similar to that reported by persons with MS (16) and by patients in the acute hospital (37). Adaptation and modification of the environment could eliminate these barriers and improve participation (38).
There are some limitations of this study. This is a cross-sectional survey and does not provide longitudinal information. All participants met the inclusion criteria and were listed on a database of people with GBS and MS held at the RMH and agreed to participate in research projects. In an attempt to reduce recall bias, all questions were limited in the main to the current situation. Medical records were used only to confirm participant report and no additional information was obtained. This method of information gathering has potential information bias.
Only patient-reported problems were linked to the ICF categories. The ICF checklist in this study was previously used in an MS cohort, and we considered it comprehensive enough for use in the GBS population. We did not use the WHO qualifiers scale (0–4) nor report concurrent co-morbidities, which may contribute to problems in function.
The participant report is subject to interviewers’ interpretation; however, ICF categories linked were consistent with medical information available for participants. This consistency can therefore be interpreted as cross-validation of the results. The generalizability and validity of these findings need to be established in future studies.
This is the first study to use ICF to compare patient-reported disability in GBS survivors and persons with MS; and to identify relevant environmental factors. Mapping patient-reported limitations to the ICF framework outlines the domains affected by the 2 disease conditions. This information has the potential to allow clinicians to provide targeted intervention to facilitate communication and management of these persons. The longer-term neurological sequelae and environmental factors in the GBS population need further study in larger cohorts. The GBS patient perspective may lay an empirical foundation from the Australian perspective to develop an ICF Core Set for GBS.
Acknowledgements
We would like to thank all GBS participants and their carers. We are grateful to Dr R. Bignell for medical record audit. We also acknowledge Professor L. Turner- Stokes and Dr D. Playford for their comments and support.
Conflicts of interest: The authours declaire no conflicts of interest.
References