Diana Kadetoff, MD and Eva Kosek, MD, PhD
From the Osher Center For Integrative Medicine, Stockholm Brain Institute, Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden
Diana Kadetoff, MD and Eva Kosek, MD, PhD
From the Osher Center For Integrative Medicine, Stockholm Brain Institute, Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden
OBJECTIVE: To assess activation of the sympathetic nervous system and the hypothalamic-pituitary-adrenocortical axis during static exercise in patients with fibromyalgia.
Patients and methods: Sixteen patients with fibromyalgia and 16 healthy controls performed a static knee extension until exhaustion. Plasma catecholamines, adrenocorticotropic hormone and cortisol, as well as blood pressure and heart rate, were assessed before, during and following contraction. Plasma C reactive protein was analysed at baseline.
RESULTS: Blood pressure and heart rate increased during contraction (p < 0.001) and decreased following contraction (p < 0.001) in both groups alike. Compared with baseline, plasma catecholamines increased during contraction in both groups (p < 0.001), but patients with fibromyalgia had lower levels of plasma adrenaline (p < 0.04) and noradrenaline (p < 0.08) at all times. Adrenocorticotropic hormone increased at exhaustion in controls (p < 0.001), but not in patients with fibromyalgia, who also had lower adrenocorticotropic hormone at exhaustion (p < 0.02) compared with controls. There were no group differences, or changes over time in plasma cortisol. High sensitivity C reactive protein was higher in patients with fibromyalgia compared with controls (p < 0.02).
CONCLUSION: Patients with fibromyalgia exhibited a hypoactive sympatho-adrenal system as well as a hypo-reactive hypothalamic-pituitary axis during static exercise.
Key words: fibromyalgia; exercise; catecholamines; hypothalamo-pituitary-adrenal axis; sympathetic nervous system; autonomic nervous system.
J Rehabil Med 2010; 42: 765–772
Correspondence address: Eva Kosek, Department of Clinical Neuroscience, Karolinska Institute, Retzius väg 8, SE-171 77 Stockholm, Sweden. E-mail: eva.kosek@ki.se
Submitted August 12, 2009; accepted June 9, 2010
INTRODUCTION
Fibromyalgia (FM) is a common chronic pain syndrome with a prevalence of 2% in the general population, which mainly affects women (80%) (1). Widespread pain and generalized allodynia to pressure are the hallmarks of FM, but associated symptoms, such as fatigue, sleep disturbance, irritable bowel syndrome, depression and anxiety, are frequently reported by patients with FM (2). The pain in FM is widespread, deep, mainly localized to muscles, with few pain-free intervals (3). Typically, the pain is exacerbated during and following physical activity (4), which has to be taken into account in the rehabilitation of patients with FM. Current treatment recommendations advocate low-intensity exercise in FM (2) in order to increase treatment compliance (5). However, a better understanding of the pathophysiological mechanisms is a prerequisite for the development of more efficient rehabilitation programmes for this large group of patients.
The pain in FM is most likely explained by a complex interaction between peripheral and central mechanisms, such as muscle ischaemia (6) and dysfunction of endogenous pain modulation (7, 8). From this perspective, the autonomic nervous system is of interest, since it is involved in the regulation of muscular blood flow as well as physiologically closely linked to endogenous pain modulatory mechanisms. Cohen et al. (9) reported evidence of a basal sympathetic nervous system hyperactivity with hypo-reactivity in patients with FM based on 24-h heart rate variability analysis. Others reported reduced sympathetic reactivity in patients with FM following exposure to various stressors (10).
The principal components of the human stress response are the locus ceruleus/noradrenaline-sympathetic system (i.e. the sympathoadrenal system) and the hypothalamic-pituitary-adrenocortical (HPA) axis (11). Kvetansky et al. (12) described a mutually stimulatory interaction between these systems. Kjaer et al. (13) reported increased serum catecholamine and adrenocorticotropic hormone (ACTH) levels, as well as an increase in blood pressure (BP) and heart rate (HR) during a two-legged sustained static knee extension corresponding to 15% maximal voluntary contraction force (MVC) in healthy subjects. Therefore, we choose this kind of physical exercise in our study to assess autonomic reactivity in patients with FM. We hypothesized that patients with FM would have a relative hypo-reactivity of the sympatho-adrenal and the HPA-axis during static muscle contractions manifested by reduced serum adrenaline and ACTH/cortisol levels, while the baseline serum concentrations of these hormones would be normal. Furthermore, we hypothesized that patients with FM would have reduced release of noradrenaline during static contractions as a sign of sympathetic nervous system hypo-reactivity.
The objective of this study was to compare patients with FM and healthy controls during the same absolute contraction force in order to avoid the potential confounding factors related (i) to possible differences in fitness levels between patients and controls; and (ii) to the difficulty in correctly assessing the true % MVC (14). Previously, it has been shown that trained individuals exhibit higher adrenaline, noradrenaline (15) and ACTH (16) release during the same relative exercise intensity compared with sedentary subjects. However, lower release of adrenaline, noradrenaline (15) and ACTH (17) have been reported following the same absolute exercise in trained individuals compared with untrained. Since patients with FM are often physically unfit, the finding of lower levels of catecholamines and ACTH in patients with FM compared with controls during the same absolute workload would signify a true hypo-reactivity in the sympathetic nervous system and the HPA-axis.
METHODS
Subjects
Patients. Sixteen female patients with FM with a mean age of 38.2 years (age range 22–56 years) participated. The patients were new referrals and were all outpatients at the Department of Rehabilitation Medicine and fulfilled the classification criteria proposed by the American College of Rheumatology 1990 for fibromyalgia published by Wolfe et al. (18). The mean duration of widespread pain was 3 years (range 6 months–10 years). All the patients had normal laboratory tests regarding erythrocyte sedimentation rate, haematology count, liver enzymes, creatinine kinase, thyroid function, rheumatoid factor and antinuclear antibodies. Exclusion criteria were: presence of autoimmune or neurological disease, liver or renal impairment, diabetes mellitus, thyroid dysfunction or other endocrine diseases, malignancies, cardiovascular/pulmonary disease, pregnancy or breastfeeding, severe psychiatric illness, and other serious medical conditions that would interfere with participation in the study.
No medication was taken on a regular basis and no analgesics had been used on the day of assessment. One patient was working full-time, 4 patients were on 50% sick-leave and the remaining patients were on 100% sick-leave.
Controls. Sixteen healthy sex- and age-matched subjects with a mean age of 38.3 years (age range 22–53 years) participated. They were recruited by local advertisements at the Karolinska Hospital/Institute. They were matched following a group-wise procedure. All subjects had previously participated in another study by the same authors (4).
The study was approved by the local ethics committee and all subjects gave their informed consent to participate in the study. The study followed the guidelines according to the Declaration of Helsinki.
Materials
BP and HR was measured using an automatic digital blood pressure monitor UA-767 (DBPM) (A and D Instruments Ltd, Oxford, UK). The Borg CR-10 scale (19) was used to rate exertion/fatigue and pain intensity. The scale is anchored with the numbers 0 (nothing at all) through 10 (extremely strong) and a dot symbolizing maximal. There is no upper limit to the scale and participants can use fractions to describe level of sensation. Maximal isometric strength was assessed using a dynamometer (0–500 N) (PIAB Test System, Mecmesin Ltd, West Sussex, UK). Pressure pain thresholds (PPTs) were assessed using a pressure algometer (Somedic Sales AB, Hörby, Sweden) with a probe area of 1 cm² and a rate of pressure increase of approximately 50 kPa/s.
Procedure
The tests were performed at standardized times in the morning (9 patients and 9 controls) and in the early afternoon (7 patients and 7 controls) in a quiet laboratory room. An intravenous cannula (Venflon) was inserted into the left antecubital vein. The subjects were then seated comfortably in a chair and familiarized with the equipment and the procedure. Following 10 min of rest they were asked to rate global pain intensity on the Borg CR-10 scale (19). The sites for pressure algometry assessments were identified and marked (m. quadriceps femoris dx; midway between the groin and the apex of the patella and m. deltoideus dx; lateral part 10 cm below acromion). The algometer was demonstrated and the subjects were instructed to push the button at the moment when the pressure sensation became painful. A minimum of two assessments were performed in sites not included in the study to ensure adequate subject performance. PPTs were always determined twice at each site. The mean value was calculated and used for further analysis (as the actual PPT). Following additional 20 min of rest the first blood sample was drawn (p-adrenaline, p-noradrenaline, p-ACTH, p-cortisol, p-myoglobin, p-CK (creatine kinase), p-CRP (highly sensitive C-reactive protein), followed by determination of BP, HR and ratings of exertion/fatigue and pain at the thighs (baseline values).
The subjects were then instructed to perform a standardized isometric contraction with m. quadriceps femoris bilaterally. The contraction was performed in a sitting position, with the hips and knees held in approximately 90° flexion pushing against a resistance (8 kg × 9.81 m/s² = 78.5 N) attached horizontally to the ankles. The contraction was held until exhaustion or for a maximum of 20 min. Following 2.5 min of contraction a second blood sample was drawn (p-adrenaline, p-noradrenaline, p-ACTH, p-cortisol), followed by determination of BP, HR, ratings of exertion/fatigue and pain at the thighs and assessment of PPTs. A third blood sample was drawn at exhaustion (during contraction) (p-adrenaline, p-noradrenaline, p-ACTH, p-cortisol), followed by determination of BP, HR, ratings of exertion/fatigue and pain at the thighs. After 30 min of rest in the sitting position the fourth blood sample was drawn (p-cortisol, p-myoglobin, p-CK) followed by determination of BP, HR, PPTs and ratings of exertion/fatigue and pain. Finally, the maximal isometric knee extensor strength (MVC) at 90° of knee flexion was determined during a 15 s contraction, 3 times, with 1 min of rest in-between trials. The best value noted on the dynamometer was used to calculate % MVC during the isometric contraction period. We refrained from assessing maximal strength at the beginning of the session in order to avoid interference with the baseline laboratory analysis.
Laboratory analysis
Plasma catecholamines (adrenaline and noradrenaline). Samples were collected in a 5 ml Na-heparin tube and placed on ice immediately. The samples were centrifuged for 10 min at 2000 g/+10°C. The plasma was pipetted into a collection tube (5 ml polypropylene) and frozen at –70°C. The samples were analysed by high performance liquid chromatography using 1,2-difenyletylendiamin as pre-column fluorescence derivatization reagent.
Plasma adrenocorticotropin hormone. Samples were collected in a 5 ml EDTA tube (siliconized). The samples were centrifuged for 10 min at 2000 g/+10°C. The plasma was pipetted into a collection tube (5 ml polypropylene) and frozen at –20°C. The analysis was performed by chemoluminescence (Advantage Instrument, Nichols, Masison, NJ, USA).
Serum cortisol, high-sensitivity C-reactive protein, creatine kinase (CK) and myoglobin. Samples were collected in a 5 ml serum tube and centrifuged for 10 min at 2000 g/+22°C. Analysis of s-cortisol was performed by immunofluorescence (AutoDelfia, Wallac, Turku, Finland). S-CRP was analysed by latex-enhanced immunonephelometry (Behring Nephelometer II, Dade Behring, Deerfield, IL, USA). S-CK was analysed using an enzymekinetic LX instrument (Beckman Coulter, Brea, CA, USA).
S-myoglobin was analysed by electrochemoluminescence (Elecys 2010, Roche, Basel, Schweiz).
Statistics
Group differences in contraction force and duration of contraction were analysed by Student’s t-test. BP, HR, PPTs and plasma levels of adrenaline, noradrenaline, ACTH and cortisol were analysed by a two-way repeated measures analysis of variance (ANOVA). The within-subjects variable was time, with 3 or 4 levels (before contraction, during contraction (2.5 min and at exhaustion) and following contraction), and the between-subjects variable was group, with two levels (patient and control). Differences between levels of the within factor time were evaluated by the Fisher LSD test if the sphericity condition was tenable, otherwise specific contrasts were applied. When more than 3 pairwise comparisons were performed, the p-values were corrected according to the Bonferroni procedure. When the two-factor interaction was significant, simple main effects were examined, i.e. effects of one factor holding the other factor fixed. For example, test of group effect (fibromyalgia vs controls) at different time points (before, during (2.5 min and at exhaustion) and following contraction). The degrees of freedom of the F-tests associated with the time factor were corrected according to Greenhouse-Geisser if the sphericity condition did not hold. Since the distribution of some of the variables were positively skewed, appropriate power transformations were carried out before analyses (log X and –1/X). Between group differences in CRP, CK and myoglobin were analysed by Mann-Whitney U-test with correction for ties and within-group differences by Wilcoxon’s signed-rank test. Differences between groups in the ratings of pain and exertion/fatigue were analysed by Mann-Whitney U-test with corrections for ties. The Friedman’s test was used for within-group comparisons of ratings over time, with post hoc analysis using the Wilcoxon’s signed-rank test. For the omnibus tests, p < 0.05 was considered statistically significant, whereas the Bonferroni method was applied for post hoc contrasts, i.e. 0.05 divided by the number of contrasts performed. Software used: Statistica 7.1, StatSoft®, Inc. Tulsa, OK, USA.
RESULTS
Maximal voluntary contraction force and contraction time
The mean MVC corresponded to 240.2 Nm in patients and 345.4 Nm in controls (p < 0.002). On average, the contraction corresponded to 11% MVC in patients and 8% MVC in controls (p < 0.01). The mean contraction time to exhaustion was 12 min in patients and 16 min in controls (p < 0.001). Only two controls and one patient performed the contraction for 20 min.
Ratings of exertion/fatigue and pain intensity
Patients with FM rated higher global pain intensity (median: 3, range 0–6.2) compared with controls who were all pain-free (p < 0.001). Patients with FM also had higher ratings of exertion/fatigue (p < 0.001) and pain in the thighs (p < 0.001) at all times compared with controls (Table I).
| Table I. Ratings (Borg CR-10 scale) of exertion/fatigue and pain in the thighs (median and 25th to 75th percentile) before, during (2.5 min and exhaustion) and following (Follow) a two-legged isometric knee extension until exhaustion in patients with fibromyalgia and healthy controls. Statistically significant differences from controls are indicated. | ||||||||
| Fibromyalgia | Controls | |||||||
| Before | 2.5 min | Exhaustion | Follow | Before | 2.5 min | Exhaustion | Follow | |
| Exertion/fatigue | 1.5* (0–2.2) | 7.5* (5.0–10.0) | 10.0* (7.5–10.0) | 2.75* (2.0–3.5) | 0 (0–0) | 2.75 (1.75–4.0) | 5.0 (5.0–7.0) | 0 (0–0) |
| Pain | 1.5* (0–2.5) | 6.0* (5.0–9.0) | 7.0* (8.9–10.5) | 2.0* (1.25–4.0) | 0 (0–0) | 1.5 (0.1–2.75) | 3.0 (1.25–4.5) | 0 (0–0) |
| *p < 0.001. | ||||||||
Compared with baseline, ratings of exertion/fatigue in the thighs increased in both groups at 2.5 min of contraction (difference between baseline and 2.5 min) (p < 0.001) and continued to increase until exhaustion (difference between 2.5 min and exhaustion) (p < 0.001) in both groups. Following contraction (30 min) the ratings of exertion/fatigue remained elevated compared with baseline in patients with FM (p < 0.003), but had returned to baseline in controls. The increase from baseline in ratings of exertion/fatigue was more pronounced in patients with FM at all times compared with controls (2.5 min: p < 0.001; exhaustion: p < 0.007; and following contraction: p < 0.001) (Fig. 1).
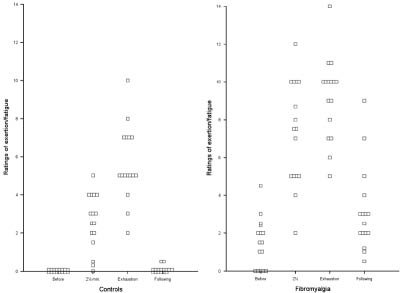
Fig. 1. Ratings of exertion/fatigue (Borg CR-10 scale) in 16 patients with fibromyalgia and 16 healthy controls before, during (at 2.5 min and exhaustion (Exh)) and 30 min after a two-legged isometric knee extension until exhaustion. Ratings of exertion/fatigue increased in both groups compared with baseline at 2.5 min (p < 0.001) and continued to increase until exhaustion (p < 0.001). The ratings of exertion/fatigue had returned to baseline following contraction (30 min) in controls, but remained elevated in the patients (p < 0.003). The increase from baseline was more pronounced in the patients at all times compared with controls (2.5 min: p < 0.001; exhaustion: p < 0.007; and following contraction: p < 0.001).
Compared with baseline, ratings of pain intensity in the thighs increased in both groups at 2.5 min of contraction (p < 0.001) and continued to increase until exhaustion (difference between 2.5 min and exhaustion) (p < 0.001). The ratings of pain intensity remained elevated in patients with FM at 30 min after contraction (p < 0.001), but had returned to baseline in controls (no controls reported any pain at this time). The increase from baseline in ratings of pain intensity was more pronounced in patients with FM at all times compared with controls (p < 0.001) (Fig. 2).
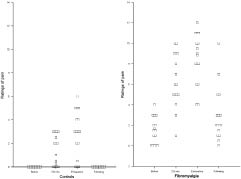
Fig. 2. Ratings of pain (Borg CR-10 scale) in 16 patients with fibromyalgia and 16 healthy controls before, during (at 2.5 min and exhaustion (Exh)) and 30 min after a two-legged isometric knee extension until exhaustion. Ratings of pain intensity increased in both groups compared with baseline at 2.5 min (p < 0.001) and continued to increase until exhaustion (p < 0.001). The ratings of pain intensity remained elevated in the patients at 30 min after contraction (p < 0.001), but had returned to baseline in controls. The increase from baseline in ratings of pain intensity was more pronounced in the patients at all times compared with controls (p < 0.001).
Blood pressure and heart rate
There was no statistically significant difference between groups in systolic (p < 0.77, dF = 1, F value = 0.09) or diastolic (p < 0.74, dF = 1, F value = 0.11) BP. The change over time was statistically significant for systolic (p < 0.0001, dF = 3, F value = 70.77) and diastolic (p < 0.0001, dF = 3, F value = 74.96) BP, but no statistically significant group/time interaction was seen for systolic (p < 0.99, dF = 3, F value = 0.03) or diastolic (p < 0.63, dF = 3, F value = 0.63) BP. In both groups alike, systolic and diastolic BP increased compared with baseline at 2.5 min of contraction (p < 0.001), continued to increase during the contraction period (difference between 2.5 min and exhaustion) (p < 0.001) and had returned to baseline 30 min after contraction (Table II).
| Table II. Mean values and standard deviations for systolic and diastolic blood pressure (BP), heart rate (HR), pressure pain thresholds (PPTs) and plasma levels of adrenaline, noradrenaline, adrenocorticotropic hormone (ACTH) and serum cortisol before, during (2.5 min and exhaustion) and following (Follow) a two-legged isometric knee extension until exhaustion in patients with fibromyalgia and healthy controls. Statistically significant differences from controls are indicated | ||||||||
| Fibromyalgia | Controls | |||||||
| Before | 2.5 min | Exhaustion | Follow | Before | 2.5 min | Exhaustion | Follow | |
| Systolic BP (mmHg) | 113 (16) | 129 (17) | 143 (16) | 117 ± 15 | 115 (12) | 131 (12) | 144 (12) | 117 (10) |
| Diastolic BP (mmHg) | 76 (11) | 90 (11) | 95 (11) | 80 ± 11 | 76 (6) | 88 (8) | 95 (8) | 77 (7) |
| HR (bpm) | 75 (10) | 87 (9) | 93 (14) | 74 ± 10 | 69 (7) | 85 (12) | 94 (12) | 70 (8) |
| PPTs Quadr (kPA) | 216 (82)† | 204 (82)† | NA | 195 ± 73† | 494 (207) | 496 (231) | NA | 464 (183) |
| PPTs Delt (kPa) | 123 (59)† | 127 (50)† | NA | 118 ± 45† | 281 (154) | 322 (157) | NA | 282 (109) |
| Adrenaline (nmol/l) | 0.11 (0.06)* | 0.16 (0.09)* | 0.24 (0.13)* | NA | 0.16 (0.10) | 0.23 (0.14) | 0.38 (0.22) | NA |
| Noradrenaline (nmol/l) | 2.70 (1.07) | 2.84 (0.88) | 3.74 (1.32) | NA | 3.29 (0.87) | 3.29 (0.92) | 4.51 (1.01) | NA |
| ACTH (pmol/l) | 3.04 (1.52) | 3.06 (1.69) | 3.29 (1.51)* | NA | 3.36 (1.63) | 3.76 (1.72) | 4.90 (2.25) | NA |
| Cortisol (nmol/l) | 302 (148) | 299 (154) | 312 (163) | 319 ± 175 | 303 (116) | 295 (112) | 332 (178) | 314 (141) |
| *p < 0.05, †p < 0.001. Quadr: m. quadriceps femoris; Delt: m. deltoideus; NA: non-applicable. | ||||||||
There was no statistically significant difference in HR between groups (p < 0.34, dF = 1, F value = 0.94). HR increased over time (p < 0.0001, dF = 3, F value = 65.13) but there was no statistically significant group/time interaction (p < 0.30, dF = 3, F value = 1.23). In both groups alike, HR increased compared with baseline at 2.5 min of contraction (p < 0.001), continued to increase during the contraction period (difference between 2.5 min and exhaustion) (p < 0.001) and had returned to baseline 30 min after contraction (Table II).
Pressure pain thresholds
PPTs were lower in patients with FM compared with controls at m. quadriceps dx. (p < 0.0001, dF = 1, F value = 41.36) and at m. deltoideus dx. (p < 0.0001, dF = 1, F value = 42.59). There was no statistically significant time effect in m. quadriceps (p < 0.19, dF = 2, F value = 1.72) nor m. deltoideus (p < 0.07, dF = 2, F value = 2.83), nor a significant interaction between group/time (quadriceps: p < 0.78, dF = 2, F value = 0.25, deltoideus: p < 0.62, dF = 2, F value = 0.48) (Table II).
Plasma catecholamine levels
Fibromyalgia patients had reduced levels of p-adrenaline at all times compared with controls (p < 0.04, dF = 1, F value = 4.40). The p-adrenaline level increased over time (p < 0.0001, dF = 2, F value = 33.70), but there was no statistically significant time/group interaction (p < 0.88, dF = 2, F value = 0.13). P-adrenaline increased in both groups alike at 2.5 min compared with baseline (p < 0.002) and continued to increase until exhaustion (difference between 2.5 min and exhaustion) (p < 0.001) (Fig. 3) (Table II). The average increase from baseline in adrenaline (± 95% confidence interval (CI)) was 0.050 ± 0.038 nmol/l in patients with FM and 0.064 ± 0.042 nmol/l in controls at 2.5 min and 0.129 ± 0.054 nmol/l in patients with FM and 0.211 ± 0.088 nmol/l in controls at exhaustion. The average increase from 2.5 min to exhaustion was 0.079 ± 0.057 nmol/l in patients with FM and 0.147 ± 0.074 nmol/l in controls. The study had a power of 0.8 to detect an increase corresponding to 0.038 nmol/l in patients with FM and 0.064 nmol/l in controls (Alpha = 0.05; Beta = 0.2).
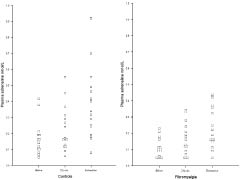
Fig. 3. Plasma adrenaline levels in 16 patients with fibromyalgia and 16 healthy controls before and during (at 2.5 min and at exhaustion) a two-legged isometric knee extension until exhaustion. The patients had lower concentrations of plasma adrenaline at all times compared with controls (p < 0.04). Compared with baseline, p-adrenaline increased in both groups alike at 2.5 min of contraction (p < 0.002) and continued to increase until exhaustion (p < 0.001).
There was a non-significant tendency of lower p-noradrenaline levels in patients with FM compared with controls (p < 0.08, dF = 1, F value = 3.25). P-noradrenaline increased over time (p < 0.0001, dF = 2, F value = 53.95), but there was no significant time/group interaction (p < 0.46, dF = 2, F value = 0.78). There was no statistically significant difference between p-noradrenaline at 2.5 min compared with baseline, but p-noradrenaline increased at exhaustion in both groups alike compared with baseline (p < 0.001) and compared with 2.5 min (p < 0.001) (Fig. 4) (Table II).
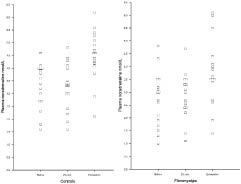
Fig. 4. Plasma noradrenaline levels in 16 patients with fibromyalgia and 16 healthy controls before and during (at 2.5 min and at exhaustion) a two-legged isometric knee extension until exhaustion. There was a non-significant tendency of lower plasma noradrenaline levels in the patients compared with controls at all times (p < 0.08). There was no statistically significant difference between p-noradrenaline at 2.5 min compared with baseline, but p-noradrenaline had increased at exhaustion in both groups alike compared with baseline (p < 0.001) and to 2.5 min (p < 0.001).
The average increase (± 95% CI) in noradrenaline from baseline to exhaustion was 1.034 ± 0.396 nmol/l in patients with FM and 1.212 ± 0.302 nmol/l in controls and the average increase from 2.5 min to exhaustion was 0.919 ± 0.345 nmol/l in patients with FM and 1.225 ± 0.406 in controls. The study had a power of 0.8 to detect an increase corresponding to 0.685 nmol/l in patients with FM and 0.557 nmol/l in controls (Alpha = 0.05; Beta = 0.2).
Plasma adrenocorticotropic hormone and cortisol
The ACTH samples of two patients were lost due to technical failure. The analysis of ACTH were therefore based on 14 patients with FM and 16 controls. No statistically significant group difference was found in the concentration of p-ACTH (p < 0.18, dF = 1, F value = 1.90). P-ACTH increased during contraction (p < 0.0001, dF = 2, F value = 19.31) and a significant group/time interaction was found (p < 0.002, dF = 2, F value = 7.12). In healthy controls, there was a tendency to an increase in p-ACTH at 2.5 min compared with baseline (p < 0.09), and p-ACTH had increased at exhaustion compared with baseline (p < 0.001) and compared with 2.5 min (p < 0.001), respectively. No statistically significant change in p-ACTH was found in patients with FM (p < 0.23). There was no statistically significant difference in p-ACTH between patients and controls at baseline (p < 0.64), nor at 2.5 min (p < 0.29), but patients with FM had lower p-ACTH levels at exhaustion compared with controls (p < 0.02) (Fig. 5) (Table II). The average increase in ACTH (± 95% CI) in controls was 2.106 ± 1.194 pmol/l from baseline to exhaustion and 1.138 ± 0.621 pmol/l from 2.5 min to exhaustion. The study had a power of 0.8 to detect an increase corresponding to 0.973 pmol/l in patients with FM and 1.043 pmol/l in controls (Alpha = 0.05; Beta = 0.2).
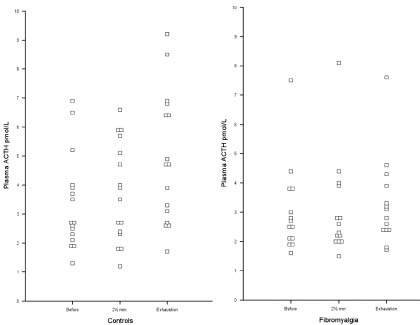
Fig. 5. Plasma adrenocorticotropic hormone (ACTH) levels in 14 patients with fibromyalgia and 16 healthy controls before and during (at 2.5 min and at exhaustion) a two-legged isometric knee extension until exhaustion. In controls, there was a tendency to an increase in p-ACTH at 2.5 min compared with baseline (p < 0.09), and p-ACTH had increased at exhaustion compared with baseline (p < 0.001) and compared with 2.5 min (p < 0.001), respectively. No statistically significant change in p-ACTH was seen in the patients during contraction and the patients had lower concentrations of p-ACTH at exhaustion compared with controls (p < 0.02).
We did not find any statistically significant differences in p-cortisol between subjects assessed in the morning compared with those assessed in the afternoon. There was no statistically significant difference in p-cortisol between groups (p < 0.81, dF = 1, F value = 0.06) and no statistically significant time effect was found (p < 0.19, dF = 3, F value = 1.64) nor a significant time/group interaction (p < 0.92, dF = 3, F value = 0.16). We did not find any statistically significant differences in p-cortisol between subjects assessed in the morning compared with those assessed in the afternoon (Table II).
Plasma high-sensitivity C-reactive protein, creatine kinase and myoglobin
The mean P-CRP was higher in patients with FM (2.66 mg/l) compared with controls (1.16 mg/l) (p < 0.02). There were no statistically significant group differences at baseline in average CK concentrations (patients: 0.88 µkat/l; controls: 1.30 µkat/l) or myoglobin concentrations (patients: 26.81 µg/l; controls: 29.06 µg/l). No significant changes were seen when CK values were compared before and following the contraction in patients (0.88 µkat/l and 0.87 µkat/l) or controls (1.30 µkat/l and 1.16 µkat/l). The same was found for myoglobin values before and following contraction (patients: 26.81 µg/l and 28.62 µg/l (NS); controls: 29.06 µg/l and 37.19 µg/l (NS)).
DISCUSSION
To our knowledge, this is the first study comparing sympathetic and HPA-axis activity in patients with FM and healthy controls during the same absolute physical activity. The main findings of our study were that patients with FM had reduced adrenaline levels at baseline and during exercise, showing a hypo-active sympathoadrenal system. In addition, patients with FM exhibited a hypo-reactivity of the HPA-axis during exercise. The hypo-active sympatho-adrenal system and the hypo-reactive HPA-axis in patients with FM could contribute to the exercise intolerance, which is one of the main characteristics of FM. Furthermore, patients with FM had higher levels of high-sensitivity CRP, indicating elevated inflammatory activity compared with controls. Confirming our previous results Kadetoff & Kosek (4), we found reduced strength and endurance, higher ratings of exercise-induced pain and exertion/fatigue as well as lower PPTs at all times, in our patients with FM compared with healthy controls. There were no statistically significant baseline group differences in BP or HR. BP and HR increased in both groups alike at 2.5 min of contraction and at exhaustion, indicating that patients with FM were truly exhausted even though they had shorter contraction times compared with controls.
Plasma catecholamines at baseline and during exercise
We found lower plasma adrenaline and a tendency (p < 0.08) to lower plasma noradrenaline levels at baseline in patients with FM compared with controls. Previously, Giske et al. (20) reported normal baseline plasma catecholamine levels in patients with FM. However, Crofford et al. (21) found lower levels of plasma neuropeptide Y (a correlate of sympatho-adrenal and sympatho-neural output) in patients with FM. Reduced physical fitness could explain the lower adrenaline levels at baseline in our patients with FM, since adrenaline concentrations increase in trained individuals (16).
The increase in plasma adrenaline during exercise is considered to reflect adreno-medullary secretion, while the noradrenaline concentration is regarded as an index of sympathetic nervous activity (16). In our study, plasma catecholamines increased compared with baseline at 2.5 min of contraction and continued to increase until exhaustion, in both groups alike, which is in accordance with previous findings by Kjaer et al. (13) in healthy individuals. However, our patients with FM had significantly lower plasma adrenaline levels and a tendency to lower plasma noradrenaline levels at 2.5 min of contraction and at exhaustion compared with healthy controls. Peronnet et al. (15) reported lower release of adrenaline and noradrenaline following the same absolute exercise in trained individuals compared with untrained. Therefore, the lower concentration of plasma adrenaline at 2.5 min of contraction in our patients with FM signified a true reduction in sympatho-adrenal activity that cannot be explained by lower fitness.
We are not aware of any other study comparing catecholamine secretion during the same absolute workload in patients with FM and healthy controls. Our results tally those of previous studies, where a reduced adrenaline, but not noradrenaline, response was reported in patients with FM during repetitive static contractions corresponding to 30% MVC (20) and during dynamic exercise (22), respectively. Hypothetically, the long-term basal increase in sympathetic tone (9) could lead to a down-regulation of catecholamines and explain the low catecholamine concentrations at baseline and during exercise in our patients with FM.
Plasma adrenocorticotropic hormone and serum cortisol at baseline and during exercise
In accordance with previous studies (23, 24) we found normal baseline ACTH and cortisol levels in our patients with FM. There were no statistically significant differences in ACTH levels between 2.5 min of contraction and baseline in either group, but ACTH had increased at exhaustion in controls but not in patients with FM, while cortisol levels remained unchanged during and following contraction in both groups. Our findings of increased ACTH, but not cortisol, during contractions in controls are in accordance with previous findings in healthy subjects (13). Normally, ACTH secretion increases during physical activity in relation to intensity and duration (16). Leal-Cerro et al. (17) reported a lower release of ACTH following the same absolute workload in trained individuals compared with untrained. Furthermore, no difference was found in plasma ACTH between athletes and sedentary controls following repeated concentric knee extensions, even though the total workload was higher in athletes (25). Therefore, the lower ACTH concentration at exhaustion in our patients with FM compared with controls was probably not explained by reduced physical fitness in the patient group.
To our knowledge, ACTH secretion in response to static contractions has not previously been studied in FM, although Gürsel et al. (24) did not find a statistically significant difference in ACTH secretion between patients with FM and healthy controls during an exercise stress test (treadmill). However, in accordance with our results, Adler et al. (23) reported a reduced ACTH but not cortisol response in patients with FM following a graded stressor that allowed for counter-regulatory processing (i.e., a stepped hypoglycaemic hyperinsulinaemic clamp test). The reports of exaggerated ACTH response to exogenous corticotrophin-releasing hormone (CRH) in patients with FM have been proposed to reflect up-regulation of pituitary CRH receptors as a consequence of chronic hypoactive CRH neurones (26). The lower ACTH secretion at exhaustion in our patients with FM could be explained by a reduced CRH response to exercise. A reduced CRH response in FM could hypothetically be due to the high concentrations of substance P (SP) in the cerebrospinal fluid (27), since SP is a potent inhibitor of CRH, and/or could be mediated by decreased sympathetic stimulation (26).
We found no increase in cortisol levels in either group during contraction, which is in accordance with the lack of cortisol increase during a two-legged knee extension corresponding to 15% MVC reported by Kjear et al. (13). The most likely explanation is that the exercise intensity in our study was too low to induce an increase in cortisol levels (28).
Plasma creatine kinase, myoglobin and high-sensitivity C-reactive protein
As expected, plasma CK and myoglobin levels were normal, indicating that there was no major muscle tissue damage. High-sensitivity plasma CRP was elevated in patients with FM compared with controls, with the average concentration of CRP in patients with FM corresponding to the double control value. High-sensitivity CRP is a sensitive, but non-specific, marker of inflammation reflecting increased production of interleukin-1 (IL-1) and IL-6 (29). Salemi et al. (30) reported increased concentrations of IL-1, IL-6 and TNF-alpha in the skin of patients with FM and Uceyeler et al. (31) reported reduced blood levels of the anti-inflammatory cytokines IL-4 and IL-10 in patients with chronic widespread pain. The altered autonomic balance with a relative reduction in parasympathetic tone, as has been described by Cohen et al. (9) in patients with FM, could hypothetically alter the balance between pro- and anti-inflammatory cytokines in favour of the former through the reduction in the anti-inflammatory vagal reflex (32). Over-production of pro-inflammatory cytokines in the central nervous system has been shown to contribute to central sensitization causing enhanced pain and fatigue (33), which calls for further research regarding central inflammatory processes in FM.
Limitations
There are several limitations to this exploratory study. One is that the investigator was not blinded to which group the subjects belonged. However, great care was taken to give all instructions in a standardized manner and to follow a strict protocol. Furthermore, due to the low number of subjects and to the fact that patients with FM were recruited from a rehabilitation department our results need to be verified in other studies before being generalized to the whole FM population. In addition, it must be remembered that our results do not reflect the 24-h catecholamine secretion. Therefore, we cannot exclude that the subjects were mentally preparing for the physical exercise to come so that our baseline levels actually reflected a relative hypo-reactivity of the sympathetic nervous system in patients with FM, rather than a true basal hypo-activity. During the post-awakening period, ACTH and cortisol levels are normally increased and there is dissociation between ACTH and cortisol secretion (34). Sleep disturbances are common in patients with FM and could have affected our ACTH and cortisol assessments. A weakness is that we did not assess sleep quality or wake-up times in our subjects. However, we did not find any statistically significant baseline group differences in ACTH and cortisol levels between the groups, neither any difference between subjects examined in the morning vs those examined in the afternoon, making a major contribution of circadian rhythms/wake-up times unlikely.
Perspectives
Our findings of a hypo-active sympatho-adrenal system and a hypo-reactive HPA axis in patients with FM are interesting given the role of the autonomic nervous system in the regulation of muscular blood flow as well as in endogenous pain modulation. Normalization of the function of the sympatho-adrenal system and the HPA axis in patients with FM would be expected to lead to reduced pain due to improved muscle blood flow (6) and increased release of analgesic substances such as adrenal enkephalins (35) and beta-endorphins (36). Currently, the recommended rehabilitation of patients with FM consists of multi-professional treatment, including physical exercise, cognitive behavioural therapy (CBT) and pharmacological treatments (2). Physical exercise could be beneficial for patients with FM by increasing/normalizing catecholamine concentrations at baseline (16), which has been supported in one pilot study (37). These effects could also act to normalize HPA-axis reactivity given the mutually stimulating interactions between the sympathetic nervous system and the HPA-axis (12). Hypo-activity of the HPA axis is common in subjects living with long-term stress or pain (38). CBT aims at improving coping with pain and reducing stress in patients with FM, which in turn would be expected to improve/normalize the function of the HPA-axis. Currently, we have an ongoing study assessing the effect of CBT on symptoms and autonomic function in patients with FM, which has, to our knowledge, not been assessed previously. Furthermore, we are currently planning a prospective, multicenter study assessing the effects of specific exercise programmes on symptoms, function and autonomic nervous system activity in patients with FM.
ACKNOWLEDGEMENTS
The study was supported by grants from the Swedish Rheumatism Association, Trygg Hansa’s Research Foundation, King Gustaf V: the 80th Year Foundation and the Karolinska Institute.
Conflict of interest: No financial support from commercial sources for this study.
REFERENCES

