OBJECTIVE: To assess the cost of walking in individuals with multiple sclerosis and to investigate its relationship with dyspnoea and fatigue.
METHODS: In 46 individuals with multiple sclerosis and in 36 healthy controls, the cost of walking was measured during the 6-min walk test. Perceived breathlessness after walking was rated on a visual analogue scale and corrected for the distance walked. The subjects’ perceived effect of fatigue was assessed by means of the Modified Fatigue Impact Scale.
RESULTS: The cost of walking was significantly higher in individuals with multiple sclerosis than in controls; however, individuals with multiple sclerosis with normal walking speeds had normal costs of walking. The cost of walking was directly related to the degree of disability, but not to breathlessness perception and fatigue. Individuals with an Expanded Disability Status Scale score greater than 2.5 were highly likely to show an increased cost of walking. Breathlessness perception was higher than in controls and was related to fatigue.
CONCLUSION: Individuals with multiple sclerosis, even with mild disability and not requiring any assistive devices, may have an increase in cost of walking. This suggests that an aerobic training programme should be considered in these patients. Energy expenditure when walking is not a determinant of fatigue or exertional dyspnoea in individuals with multiple sclerosis and low levels of disability.
Key words: walking; fatigue; disability; multiple sclerosis.
J Rehabil Med 2010; 42: 719–723
Correspondence address: Alfredo Chetta, Clinica Pneumologica – Padiglione Rasori, Azienda Ospedaliero-Universitaria, Viale Rasori 10, IT-43125 Parma, Italy. E-mail: chetta@unipr.it
Submitted February 11, 2010; accepted June 30, 2010
INTRODUCTION
The metabolic energy cost of walking (CW) may increase because of mechanical inefficiency in people with walking limitations resulting from neurological or orthopaedic diseases (1–4). The measurement of energy expenditure may provide a method to determine the energetic penalty of gait disabilities (5).
Until now, discordant results have been reported on energy costs in persons with multiple sclerosis (MS). Olgiati et al. (6) showed that individuals with MS had a poor exercise tolerance, which was related to an increased energy cost when exercising on a treadmill, depending mainly on spasticity rather than on ataxia or weakness of the lower limbs (7). Paul et al. (8) confirmed this finding in individuals with MS who walked at their own preferred walking speed using assistive devices. In their study, although functional electrical stimulation reduced the CW, the cost remained significantly greater than that of controls. Conversely, Tantucci et al. (9) found that the energy cost of incremental exercise on a cycle ergometer was not increased in persons with MS and mild disability, even if individuals with MS showed a poor training condition compared with control subjects. Mildly disabled individuals with MS did not differ from healthy subjects in oxygen costs during a graded exercise test on a cycle ergometer (10). Until now, the energy cost has not been investigated in individuals with MS who undergo self-paced corridor tests without any walking aids.
People with MS often have problems walking, which may cause restrictions in their social lives. In persons with MS, walking limitations may be related to limb weakness, spasticity, sensory loss, balance disturbances and lack of coordination. Furthermore, fatigue and poor exercise tolerance may contribute to worse gait, compromising functional walking ability to a greater extent. Fatigue is one of the most common symptoms of MS and it is considered to have a major impact on health-related quality of life (11). Fatigue in MS is multifactorial and complex, involving dysregulation of the immune system, changes in the nervous system related to the disease process, neuroendocrine and neurotransmitter changes, and other factors, such as physical deconditioning, sleep disturbance, pain, and side-effects of medication (11). Whether the energy CW in persons with MS is related to fatigue and exertional dyspnoea has not yet been investigated.
The aim of this study was to assess the CW during the self-paced corridor 6-min walk test (6MWT) in people with MS who have mild disability not requiring any assistive devices, compared with that of healthy subjects, and to investigate its relationship with the perceived effect of fatigue and breathlessness on exertion. In order to exclude a ventilatory limitation to the 6MWT, lung function was measured in all subjects.
METHODS
Subjects
Persons with MS were screened from a waiting list for a rehabilitation programme at the MS outpatient clinic at Modena New Civil Hospital between June 2008 and December 2009. Individuals with MS were diagnosed according to Poser’s criteria (12). Inclusion criteria were: (i) being ambulatory without any assistive device including cane, crutch or walker; and (ii) being willing and able to wear the oxygen analysis system while walking. Individuals with MS were excluded if they had a relapse 4 weeks before the study or had a history of cardiac, pulmonary, orthopaedic, metabolic, or other medical conditions precluding participation or were currently receiving steroid therapy or had been treated with steroids within two months prior to the study. Individuals with MS undergoing interferon treatment were asked to perform lung function testing and 6-min walk tests at least 24-h after administration of the drug.
The control group comprised age- and gender-matched healthy subjects. Control subjects were recruited from the medical staff of the University Hospital of Parma and the Modena New Civil Hospital. All subjects gave informed consent to participate in the study. The study was approved by the local ethics committee.
Clinical assessment
The subjects’ neurological impairment and degree of disability were assessed by the Expanded Disability Status Scale (EDSS), which provides a score ranging from 0, indicating normal neurological findings, to 10, indicating death from MS (13). This scale is a reliable and valid measure of impairment and disability in individuals with MS (14). The EDSS score was assigned by a neurologist (Patrizia Sola) who was unaware of the subjects’ pulmonary function and walking test results. Only individuals with a score of 4 or less on the EDSS were included.
The subjects’ perceived effect of fatigue during the previous 4 weeks was assessed by the Modified Fatigue Impact Scale (MFIS) (15), which has been validated in individuals with MS (16, 17). The MFIS is a structured, self-report, 21-item questionnaire that provides an assessment of the effects of fatigue in terms of physical, cognitive and psychosocial functions. Scores on the MFIS range from 0 to 84, and all items are scaled so that higher scores indicate a greater effect of fatigue on a person’s activities. Fatigue is defined as a self-reported lack of physical or mental energy that is perceived by the individual to interfere with usual and desired activities (16).
Lung function testing and 6-min walk test
Pulmonary function was measured with a flow-sensing spirometer and a body plethysmograph connected to a computer for data analysis (Vmax 22 and 6200, Sensor Medics, Yorba Linda, USA). Baseline total lung capacity (TLC), forced expiratory volume in the first second (FEV1), and FEV1/vital capacity (VC) ratio were recorded. TLC and FEV1 were expressed as the percentage of predicted value (18) and FEV1/VC as a percentage.
Individuals with MS and controls performed two 6MWTs according to a standard protocol (19). The 6MWT is self-paced and involves measuring the distance a patient can walk on a level course in 6 min. The 6MWT is a symptom-limited exercise test, so subjects were allowed to stop if necessary, although they were instructed to resume walking as soon as possible. The second 6MWT was performed in the same manner as the first, following a rest of at least 60 min. The walk distance (WD, in m) and the walking speed (WS, in metres/s) were recorded. Oxygen uptake (VO2, in ml/kg/min) was monitored continuously with a portable lightweight system (Oxycon Mobile, Jäger, Würzburg, Germany) from 5 min before the walk until test completion, as well as 5 min after completion or until return to the baseline level. The CW during the walk, which refers to the amount of oxygen consumed per unit of body mass and walked distance, was expressed in ml O2*kg–1*m–1 (6, 20) as mean value over the 6-min walk period. Results from the second walk only were used for analysis to allow for any learning effect (19, 21).
Before and immediately after the 6MWT, subjects rated the magnitude of their perceived breathlessness on an interval scale, which was a 100-mm horizontal visual analogue scale (VAS) (22). The VAS consisted of a horizontal ruler without any markings on the subject’s side and with the words “not at all breathless” and “extremely breathless” on the left and right end, respectively. Breathlessness perception ratings were expressed in mm from 0 to 100 and corresponded to the distance of the marker from the left end of the VAS (BPVAS).
Statistical analysis
Values are presented as means (standard deviations), unless otherwise specified. The distribution of variables was assessed by way of the Kolmogorov-Smirnov goodness-of-fit test. The unpaired t-test, the Mann-Whitney rank-sum test and the χ2 test were used for comparison between individuals with MS and controls, when appropriate. The relationship between measurements in the MS group was estimated by Pearson’s correlation coefficient (r) or Spearman’s rank correlation coefficient (rs), when appropriate. In order to linearize the relationship between WS and CW, variables were log-transformed before analysis. In healthy subjects, WS and CW mean values ± 2 standard deviations (SD) were chosen as upper and lower limits of the normal range. The receiver operating characteristic (ROC) curve method (23) was used to plot the true positive rate (sensitivity) in function of the false-positive rate (100-specificity) for different cut-off points of the EDSS score with respect to an increased value of CW. A p-value ≤ 0.05 was considered to be significant.
RESULTS
Fifty-three individuals with MS (30 females; age range 29–61 years) were invited to participate in this study. Four of the 53 selected individuals withdrew from the study because they had a relapse 2–4 weeks before the study and 3 of the 53 individuals were excluded because they had a history of co-morbidity. The personal characteristics and pulmonary function test results of the 46 enrolled individuals with MS (27 females) and of the 36 healthy control subjects (21 females) are shown in Table I. Twenty-one individuals with MS were undergoing interferon treatment. There was no significant difference between individuals with MS and controls when age, gender, BMI and lung function were considered. The average duration of disease was 7 years, ranging from 1 to 20 years, and the median (range) EDSS score was 3 (1–4). Forty-two individuals had relapsing-remitting MS and 4 had a secondary progressive form of the disease. Thirty-eight individuals had a prevalent involvement of the pyramidal functional system, 4 individuals had mainly brainstem signs, 3 individuals had cerebellar deficiency, and one individual showed prevalent sensory function disturbances. The medians (ranges) of the total, physical, cognitive and psychosocial subscale MFIS scores were 27 (1–79), 15 (0–37), 7 (0–27), and 2 (0–6), respectively.
| Table I. Characteristics of 46 individuals with multiple sclerosis (MS) and 36 healthy subjects |
| | Individuals with MS | Healthy subjects | p-value |
| Age, years, mean (SD) | 39 (8) | 40 (9) | 0.615 |
| Sex ratio, F/M | 1.4 | 1.4 | 0.973 |
| BMI, kg/m2, mean (SD) | 23 (4) | 23 (3) | 0.896 |
| Disease duration, years, mean (SD) | 7 (6) | – | – |
| EDSS score (0–10), median (range) | 3 (1–4) | – | – |
| FEV1 (% of predicted), mean (SD) | 103 (14) | 104 (19) | 0.949 |
| FEV1/VC (%), mean (SD) | 82 (6) | 84 (6) | 0.259 |
| TLC (% of pred), mean (SD) | 109 (10) | 107 (16) | 0.710 |
| BMI: body mass index; EDSS: Expanded Disability Status Scale; FEV1: forced expiratory volume at 1st s; FEV1/VC: FEV1 in precentage of VC; TLC: total lung capacity; SD: standard deviation. |
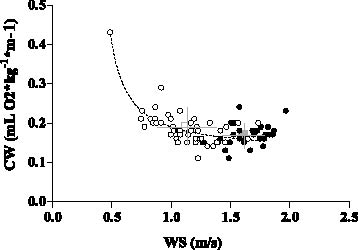
All of the individuals with MS were able to complete a 6MWT without stopping. The results of the 6MWT outcome measures in individuals with MS and in healthy controls are shown in Table II. There was a significant mean difference of 170 m in walk distance between individuals with MS and healthy controls (p = 0.001). CW and WS mean values were significantly different between individuals with MS and healthy controls (Table II). In the 12 individuals with MS (8 females) who had WS values in the normal range (1.25–1.97 m/s), CW values did not differ from those of healthy controls (0.169 (0.02) vs 0.168 (0.03) ml O2*kg–1*m–1, p = 0.948). In all subjects, the relationship between CW and WS was curvilinear (Fig. 1). In individuals with MS, when log-transformed, WS and CW were inversely correlated (r = –0.635, p = 0.001).
| Table II. Six-min walk test values of 46 individuals with multiple sclerosis (MS) and 36 healthy subjects |
| | Individuals with MS | Healthy subjects | p-value |
| WD, m, mean (SD) | 408 (88) | 578 (64) | 0.001 |
| WS, m/s, mean (SD) | 1.13 (0.25) | 1.61 (0.18) | 0.001 |
| VO2, ml/kg/min, mean (SD) | 12.6 (2.5) | 16.6 (3.7) | 0.001 |
| CW, ml O2*kg–1*m–1, mean (SD) | 0.19 (0.05) | 0.17 (0.03) | 0.017 |
| Dyspnoea (mm), median (range) | 20 (0–80) | 20 (0–76) | 0.613 |
| BPVAS/WD, median (range) | 0.050 (0–0.61) | 0.033 (0–0.13) | 0.011 |
| WD: walking distance; WS: walking speed; VO2: oxygen uptake; CW: cost of walking; BPVAS: breathlessness perception ratings on visual analogue scale after walk; SD: standard deviation. |
Fig. 1. Relationship between walk speed (WS) and energy cost of walking (CW) in 46 individuals with MS (open diamonds) and in 36 healthy control subjects (closed diamonds), while performing the 6-min walk test. Open and closed squares and bars represent mean and standard deviation values, respectively, in patients and controls.
The CW were significantly related to the EDSS scores (rs = 0.575, p = 0.001). Moreover, according to the ROC curve method, the plot of the true-positive rate (sensitivity) in function of the false-positive rate (100-specificity) for different cut-off points of the EDSS score with respect to a CW ≥ 0.23 ml O2*kg–1*m–1, as threshold value, showed a 0.800 area under the curve value (p = 0.0149). The EDSS cut-off point, which maximized sensitivity (1.0) and specificity (0.54), was > 2.5. The CW were not related to any MFIS subscale score and to BPVAS after walking.
BPVAS after walking were not statistically different between individuals with MS and healthy subjects; however, when corrected for the WD (BPVAS/WD), they differed significantly (Table II). BPVAS/WD was significantly, even if moderately related to total (rs = 0.308, p = 0.039), physical (rs = 0.427, p = 0.003) and psychosocial (rs = 0.332, p = 0.025), but not cognitive (rs = 0.186, p = 0.221) subscale MFIS scores.
DISCUSSION
The present study showed that the energy cost of self-paced walking in mildly disabled individuals with MS was higher than that of control subjects. The CW was inversely related to the walking speed and was directly related to the degree of disability, but not to the perceived effect of fatigue and perception of breathlessness after the walk. Individuals with normal walking speeds had a normal CW, while those with an EDSS score greater than 2.5 were highly likely to show an increase in the CW. Lastly, in individuals with MS, when corrected for the walk distance, perception of breathlessness after walking was higher than that in controls and was related to fatigue.
Functional exercise capacity was assessed using the 6MWT, which, in the absence of heart and lung impairment, can be considered to be a sub-maximal endurance exercise test of limb muscles, since it demands the ability to sustain the exercise, rather than the capacity for maximum exercise (19). Moreover, since most activities of daily living are performed at sub-maximal levels of exertion, the 6MWT may reflect the functional exercise level of daily physical activities (24). Furthermore, walking on a treadmill may be unfamiliar to many patients, who may be unable to pace themselves, even at low speeds, and treadmill test results may underestimate the walking performance assessed by self-paced corridor tests (25, 26).
The present study found that individuals with MS had, on the whole, an increase in energy expenditure during the self-paced walk of 10%, compared with healthy subjects. The CW was related strictly to the walk speed and was in the normal range when measured in the individuals with MS, who walked at normal speed. In healthy subjects, the energy cost of level walking is speed-dependent following a curvilinear trend that has a minimum at an optimal speed of approximately 1.1–1.3 m/s (20, 27); lower or higher walk speeds are associated with an increased energy CW, thereby compromising gait performance efficiency. It is possible that our individuals with MS, who were unable to maintain a normal speed because of problems with walking, spontaneously adopted a slower, but costlier, gait in order to improve stability or to decrease discomfort. It is generally assumed that patients with gait disturbances (1, 2, 4, 8), when walking at their own preferred speed, may increase their energy demand because of compensatory biomechanical mechanisms that they adopt to improve stability. Coordination disturbances and spasticity of the lower limbs could affect the efficiency of the pendulum-like mechanism of walking, described by Cavagna et al. (28), and minimize any possible interchange between potential and kinetic energy. Lower limb spasticity may also increase per se the energy cost of exercise (7).
A previous study (6) demonstrated that persons with MS had an increased CW on a treadmill, which was 2–3 times greater at all speeds compared with a control group. In that study, individuals with MS showed a higher CW, even when they walked at normal speeds. It is of note that in Olgiati et al’s study (6), 15 out of 24 individuals with MS utilized a walking aid on the treadmill. Paul et al. (8) found that individuals with MS, who needed assistive devices to walk, had a higher energy cost at their own preferred walk speeds in comparison with controls who walked at matched walk speeds (8). Differences in the selection criteria of individuals with MS and in study protocols may explain the difference between Olgiati et al’s and Paul et al’s results and those of the present study. Whether the kinematics of gait on a treadmill are comparable with those of walking on the ground in healthy subjects as well as in individuals with walking limitations is not known (29–31). Moreover, the use of walking aids requires upper limb(s) muscle activity, which in itself increases oxygen requirements (2).
Interestingly, Tantucci et al. (9) reported that individuals with MS and low degrees of disability had a normal cost of exercise during incremental testing on a cycle ergometer, thereby concluding that effort-related spasticity and ataxia of the lower limbs did not occur in those individuals. This finding has been confirmed by Morrison et al. (10), who found no significant difference in oxygen costs between mildly disabled individuals with MS and healthy controls when performing a graded exercise test on a cycle ergometer. Taken together, these studies suggest that the energy cost in individuals with MS may depend on the type of exercise performed. In order to ensure stability, exercise on a cycle ergometer might require less energy-demanding compensatory mechanisms than walking.
The present study provided evidence that the increase in the CW is probably associated with an EDSS score > 2.5. This finding may have clinical implications, suggesting that individuals with MS with even mild disabilities may have an increased energy demand and, therefore, may require aerobic training. Interestingly, previous studies have shown that patients with MS can benefit from an aerobic programme in terms of exercise tolerance (32–36).
In this study, the CW was not related to the perceived effect of fatigue. In individuals with MS, the lack of correlation between the CW and perception of fatigue may be due to the multidimensional origin of fatigue, because central factors (37, 38), in addition to peripheral mechanisms (6, 39), are known to play a key role in the pathogenesis of this symptom. Notably, Newman et al. (34) showed that the CW could decrease after an aerobic programme, in spite of no change in perception of fatigue.
Our results also confirmed a previous report, which failed to show a direct link between the subjective sense of dyspnoea on exertion and an increased CW (6). Taken together, these results support the view that the underlying mechanisms of exertional dyspnoea may be elusive in individuals with MS. In addition, despite having no cardiopulmonary impairment, our individuals with MS reported a higher breathlessness perception after the walk, compared with healthy subjects. A possible explanation for the greater dyspnoea intensity in people with MS at a given walked distance may be a different perceptual response to normal dyspnoeogenic stimuli during walking. Interestingly, exertional dyspnoea was related to fatigue perception in our study. Despite the different mechanisms that may be involved in these disabling symptoms, subjectivity is inherent to both of them, and this is the most like explanation of their relationship.
This study has a number of limitations. Firstly, although the 6MWT is based on self-paced walking, it does not exactly reflect natural customary walking. In fact, in healthy subjects, who perform the 6MWT, their walking speeds are usually higher than their natural customary walking speeds (24). In addition, the practice test could affect the participant’s level of fatigue. However, the 6MWT is a well-standardized walking test (19), which is an easy-to-administer form of exercise for patients (24) and, notably, has provided useful information on walking capacity and functional status of individuals with MS (35, 39–42). Interestingly, it has also been shown that, in individuals with MS, there was no fatigability while repeating the 6MWTs with a 1-h rest period between test sessions (41). Secondly, we assessed the subjects’ perceived effect of fatigue by means of the MFIS, which is a measure of fatigue in relation to the previous 4 weeks and not in relation to the actual 6MWT. We cannot exclude that measuring fatigue levels after the walk could have provided useful information on the functional status of our patients. However, in our study we aimed to analyse the impact of the patients’ fatigue on daily function and their walking capacity.
In summary, this study shows that individuals with MS, even with mild disability and not requiring any assistive devices, may have an increased CW and suggests that a an aerobic training programme should be considered in these individuals. In addition, energy expenditure when walking is not a determinant of fatigue and exertional dyspnoea in people with MS.
ACKNOWLEDGEMENTS
The authors thank Dr Patrizia Sola from the Neurosciences Department of S. Agostino-Estense New Civil Hospital of Modena and Ms Lara Bellagamba from the School of Physiotherapy, University of Modena and Reggio Emilia, for their help in recruiting and assessing patients.
We gratefully acknowledge the help of Dr Carolyn Maureen David in reviewing the manuscript.
REFERENCES