Systematic comparison is a key tool in critical discourse in science. It is useful not only for statistical comparison of intervention effects and clinical outcomes of treatment and rehabilitation, but also for analysis of conceptual developments. Here qualitative methods are also appropriate (1). Jansma et al. (2) use such an approach by applying a linguistic method to compare the concept of Physical and Rehabilitation Medicine (PRM), as described in the White Book on Physical and Rehabilitation Medicine in Europe (3, 4), with the concept of Self-Management Education (SME), as described by Lorig (5, 6) and Lorig et al. (7). This approach may contribute substantially to the philosophy and concepts of PRM and to the development of professional practice in the field.
Although the approach chosen by Jansma et al. (2) is useful for the debate, it has some limitations. Firstly, a linguistic method cannot replace discussion of the contents that may need further explanation. Additionally the linguistic method may highlight deficits in the description that do not necessarily substantially reflect the contents. Secondly, the subjects might differ substantially, so that the comparison does not tackle the core of the subjects. Both of these limitations are evident in the paper:
• Starting with the second limitation, there are substantial differences between PRM and SME. PRM is a concept based on a medical approach that includes prevention, therapy and rehabilitation. This approach includes the health condition as a key issue influencing functioning (8, 9). Within this context the definition of functioning refers to the model of the International Classification of Functioning, Disability and Health (ICF) that also aims at the health condition (10, see also 11, 12). SME does not include the medical approach of treating the underlying health condition (5). It focuses only on persons with chronic health conditions and is restricted to tertiary prevention (6). The concept is based on the principles of self-management and looks at the health system as kind of supply that has to be used in an efficient way. In contrast, PRM is part of the health system, of course using self-management approaches too. PRM is disease-related, whereas SME is not necessarily disease-related. PRM is a comprehensive concept of a medical specialty (“holistic approach”), whereas SME is “just” a self-management concept.
• Due to methods of linguistic analysis, a number of important contents are overlooked in the article. Although this is connected with some weaknesses of the White Book, some misinterpretations are obvious. First is that PRM is focused on disease. This may be true to some respect for the acute phase (13), but it does not fit for post-acute and long-term rehabilitation (Fig. 1). Here the functional approach is of special emphasis and quality of life is a main goal of intervention. The second is that the concepts of neuroplasticity and adaptation refer only to motor control. By contrast, recent results in neuroplasicity show that functional and even structural changes in the nervous system are strongly related to behaviour and behavioural learning is part of it (14 and others). This means that the reference to these concepts used by PRM interventions aiming at behaviour self-management and problem-solving capacities are, of course, included.1 Thus self-management concepts are part of PRM and are increasingly discussed in modern rehabilitation medicine (e.g. 15–17).
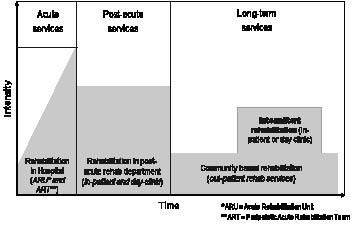
Fig. 1. Sectors of Physical and Rehabilitation Medicine (PRM) practice (8). Published with permission from Elsevier B.V.
1Some other (minor) misinterpretations from Jansma et al.’s table (2) are that:
Body functions according to the ICF model also include mental functions and psychological skills (10).
PRM also includes rehabilitation services in community settings (8).
Treatment and rehabilitation goals of PRM include improvement in quality of life (3, 4).
Social learning is also part of PRM (9).
Despite these limitations Jansma et al.’s analysis (2) is important for future discussions of PRM concepts. Although PRM claims to use a patient-centred approach (3, 4, 8, 9) and includes enabling of the person with chronic illness and disability including self-management skills, PRM practice still tends to use a traditional medical-driven approach. This originates, on the one hand, in the traditional education of medical doctors. On the other hand this is induced by the patient’s expectations towards a doctor that his or her pathology will be treated. As it enables the persons with disability and chronic health conditions to independent living (3, 4) and self-management (7), the medical approach needs to be transferred into a shared decision-making process with the person in order that he or she can make his or her own decisions within his or her social environment. Thus, the terms “patient-centred” and “shared decision-making” have to be defined much more clearly in the descriptions of PRM strategies, and the consequences for daily PRM practice has to be elaborated in more detail. Approaches can already be found in the conceptual descriptions of the rehabilitation strategy and PRM that have recently been adopted by the European Union of Medical Specialists (UEMS)-PRM-Section and the European Society of Physical and Rehabilitation Medicine (ESPRM) (18, 19) (Table I). Here the partnership between the person with disability and the service provider is part of the strategy, and the patient-centred problem-solving process is clearly addressed. In addition, the team-approach of PRM also includes the patient and his or her own wishes. (20). As mentioned above, the methods of reaching these goals need to be described in more detail. In addition, training in PRM, both at undergraduate and postgraduate level, should include techniques of shared decision-making and empowerment. Some approaches have already been developed in this respect, but more emphasis on this aspect is required.
| Table I. International Classification of Functioning, Disability and Health (ICF)-based conceptual description of Physical and Rehabilitation Medicine (PRM) (ICF terms are marked in bold text, rows are numbered in grey) (18) | ||||
| 1 | Physical and Rehabilitation Medicine is the medical specialty that, based on WHO’s integrative model of functioning, disability and health and rehabilitation as its core health strategy, | |||
| 2 | diagnoses health conditions taking into account the International Classification of Diseases | |||
| 3 | assesses functioning in relation to health conditions, personal and environmental factors | |||
| 4 | performs, applies and/or prescribes biomedical and technological interventions to treat health conditions suitable to | |||
| stabilize, improve or restore impaired body functions and structures | ||||
| prevent impairments, medical complications and risks | ||||
| compensate for the absence or loss of body functions and structures | ||||
| 5 | leads and coordinates intervention programs to optimize activity and participation | |||
| in a patient-centered problem-solving process | ||||
| in partnership between person and provider and in appreciation of the person’s perception of his or her position in life | ||||
| performing, applying and integrating biomedical and technological interventions, psychological and behavioral; educational and counseling, occupational and vocational, social and supportive, and physical environmental interventions | ||||
| 6 | provides advice to patients and their immediate environment, service providers and payers | |||
| over the course of a health condition, | ||||
| for all age groups | ||||
| along and across the continuum of care, | ||||
| including hospitals, rehabilitation facilities and the community | ||||
| and across sectors | ||||
| including health, education, employment and social affairs | ||||
| 7 | provides education to patients and relatives to promote functioning and health | |||
| 8 | manages rehabilitation, health and multi-sector services | |||
| 9 | informs and advises the public and decision makers about suitable policies and programs in the health sector and across the other sectors that | |||
| provide a facilitative larger physical and social environment; | ||||
| ensure access to rehabilitation services as a human right; | ||||
| and empower PRM specialists to provide timely and effective care | ||||
| 10 | with the goal | |||
| to enable persons with health conditions experiencing or likely to experience disability to achieve and maintain optimal functioning in interaction with the environment and in partnership between person and provider. | ||||
Overall, the comparative analysis of PRM and SME makes a useful contribution to the debate on present and future concepts of PRM. Although some differences in the principles between PRM and SME have to be taken into account, self-management should be an integrated part of PRM. Thus, in contrast to Jansma et al.’s conclusion (2), for PRM this means that self-management training should not start after medical care, but needs to be integrated into all aspects of rehabilitation and all processes of prevention.
REFERENCES
Submitted June 2, 2010; accepted August 30, 2010
Christoph Gutenbrunner, MD, PhD
Department for Rehabilitation Medicine & Coordination Centre for Rehabilitation Research, Hannover Medical School, Carl-Neuberg-Str. 1, DE-30625 Hannover, Germany. E-mail: gutenbrunner.christoph@mh-hannover.de
1Some other (minor) misinterpretations from Jansma et al.’s table (2) are that:
Body functions according to the ICF model also include mental functions and psychological skills (10).
PRM also includes rehabilitation services in community settings (8).
Treatment and rehabilitation goals of PRM include improvement in quality of life (3, 4).
Social learning is also part of PRM (9).

