OBJECTIVE: To explore ambulatory outpatient experiences and perceptions in post-acute care settings and how these experiences may have led to perceived gaps in continuity of rehabilitation care.
SUBJECTS: Fifty-seven adults undergoing outpatient rehabilitation for musculoskeletal conditions/injuries, who had had more than 10 physiotherapy treatment sessions.
METHODS: Qualitative study using a modified grounded theory approach. Data collection was carried out through 9 focus groups. Each group was recorded, transcribed literally and analyzed thematically.
RESULTS: Participants described 3 main themes in continuity; relational, informational, and management continuity. Several factors that led to gaps in the 3 types of continuity were described. The relevant factors for relational continuity were: consistency of the multi-professional rehabilitation team; and an established provider–patient relationship. Factors for informational continuity were: transfer of information among providers; and accumulated knowledge regarding patients’ disability experiences. Factors for management continuity included: consistency of care among rehabilitation providers; flexibility of the team in adapting care to functional changes; and involvement of the team in achieving patient collaboration.
CONCLUSION: This study provides evidence of gaps in different types of continuity of care within the post-acute rehabilitation services in ambulatory settings. Outpatients often perceive their experiences of rehabilitation care as non-connected or non-coherent over time.
Key words: continuity of care; outpatient; rehabilitation care.
J Rehabil Med 2011; 43: 58–64
Correspondence address: Francesc Medina i Mirapeix, Departmento de Fisioterapia. Facultad de Medicina. Universidad de Murcia, Campus de Espinardo, 30100, Murcia, Spain. E-mail: mirapeix@um.es
Submitted December 14, 2009; accepted September 20, 2010
INTRODUCTION
Post-acute rehabilitation services play an important role in improving consequences and impairments due to diseases in a manner that enables individuals with disabilities to return to a productive life (1). Rehabilitation services (such as physical therapy, speech therapy, and occupational therapy) may be delivered across several types of setting (2): inpatient rehabilitation facilities, transitional care units, ambulatory outpatient services, home care, etc.
Post-acute care service providers are under great pressure to demonstrate continuity of care throughout the entire course of care, from hospital discharge to patient’s return home (3, 4). There is growing concern among rehabilitation providers to develop policies for continuity of rehabilitation care (5, 6). This concern is consistent with an international effort to maintain and enhance continuity of care within the health system, as a way of expressing concern about the fragmentation of care (5, 7).
Despite increased interest, few empirical studies have been conducted on continuity in post-acute rehabilitation care. Most studies of continuity in rehabilitation care have focused on continuity across various healthcare services using professional information exchange between post-acute settings, with primary care physicians as the main focus (8). In spite of the complexity of many intrinsic aspects of post-acute care settings, continuity within them has not been explored. The existence of multi-professional rehabilitation teams in post-acute care settings, and the complexity of rehabilitation care suggest that gaps may exist within the continuity of care amongst different departments, professions, work shifts, and individuals within the same department (9).
There is an opportunity to improve the quality and increase the number of studies on continuity of care by studying continuity from the patients’ perspective. The experience of continuity for patients includes care that is connected and coherent over time (10). According to the model proposed by Haggerty et al. (11) from a systematic review and a subsequent workshop, this experience is dependent on patients’ experiences in 3 types of continuity: informational, management and relational continuity. Informational continuity refers to the use of information from previous events to provide adequate care to the patient. Management continuity is viewed as the provision of complementary services with shared management. Relational continuity is described as the ongoing relationship between a patient and 1 or more health providers (10).
This qualitative study aimed to contribute to the knowledge base in rehabilitation about continuity from the patients’ perspective. The study explored ambulatory outpatient experiences and perceptions in post-acute rehabilitation settings and how these experiences may have led to perceived gaps in continuity of care. Continuity of care is defined by Reid et al. (10) for this study. Therefore, two central questions were explored: (i) How do outpatients experience continuity of care in post-acute rehabilitation settings? and (ii) Which aspects of care lead outpatients to perceive a break in continuity of rehabilitation care?
METHODS
Study design
The qualitative design involved focus groups because group interaction can trigger responses and build insights that may not arise during interviews (12). Focus groups have previously been used to identify experiences related to continuity of care (13).
Setting and participants
This study included patients who were receiving post-acute rehabilitation services from a healthcare provider network in Spain. The patients were recruited from 3 post-acute ambulatory centers in Barcelona, Madrid and Seville. The centers in Madrid and Seville had a multidisciplinary rehabilitation team composed of rehabilitation physicians and physical therapists. The center in Barcelona included only physical therapists.
Subjects were invited to participate if they were 18 years of age or older, they were undergoing outpatient rehabilitation for musculoskeletal conditions/injuries (i.e. amputation, fractures, soft tissue injuries) and had had more than 10 sessions of physiotherapy treatment at the time of recruitment. Participants were excluded if they were non-Spanish speaking or presented communication impairments.
Recruitment
The study was approved by the Committee of Ethics and Research of the University of Murcia. The recruitment process took place during February and March 2007. Patients were identified in each ambulatory center from a list of patients referred to physiotherapy treatment. The list contained relevant data, such as name, diagnosis and dates of the first and last sessions. In-house physiotherapists analyzed the inclusion/exclusion criteria. In total, 95 patients were eligible to enter the study.
A purposive sampling strategy (14) was used to include subjects of varying age, gender, and clinical conditions. This enabled the selection of participants who could best provide insight into specific and personal experiences regarding the issues being examined, rather than obtaining a representative sample, as would be sought in quantitative research. Although we were aware that the final sample size was dependent on the saturation of information, we initially selected 62 subjects.
At each center a research assistant gave invitation letters to selected subjects and confirmed their willingness to participate. The letter contained an explanatory statement, date, and place of meeting. It was not signed by any rehabilitation provider, in order to ensure that subjects did not feel obliged to participate. When several patients declined to participate, new patients presenting similar characteristics were invited in order to ensure a group with a minimum size of 4. Participants were verbally reminded 2–3 days prior to interview to ensure their presence in the focus group.
Homogeneous and heterogeneous criteria were used to form the groups. Groups were divided by gender, in order to avoid apprehension amongst participants about discussing health issues in the presence of the opposite gender. However, we formed heterogeneous groups by age and clinical conditions, in order to allow variability of experiences to stimulate discussions.
Data collection
The discussions were conducted by 2 researchers; 1 moderator and 1 assistant. A topic guide containing pre-determined questions was utilized. This guide was initially formed from a literature review. The topics covered aspects of perceived quality and continuity. The following areas were included, in order to cover the 3 types of continuity: information availability, provision of separate types of healthcare, and ongoing therapeutic relationship between patients and physical therapists. Additional questions were included according to themes that emerged from the initial focus groups (15). An audiotape was used for data collection during the interviews, and a videotape and field notes were used to record the subjects’ non-verbal language, incomplete or sarcastic expressions.
Patients were reassured of their confidentiality before the beginning of each interview session and completed a consent form. Every subject participating in the focus groups agreed to be interviewed before the session began. Nine focus groups were formed because categories were consolidated with these 9 groups (15). Focus group size varied from 5 to 8 participants, and sessions lasted from 40 to 80 min.
The sessions were transcribed literally. Each participant was assigned a code number for data entry. Notes taken during the interviews, and the moderator’s reflections were used to write a report of each focus group.
Data analysis
The following steps were used in the analysis process: a first reading of all transcripts to obtain an overall impression of content; segmentation of the transcripts’ sentences or paragraphs and codification; generation of themes; and identification of any combination among themes or categories (16). This data analysis was undertaken using a modified grounded theory (15) incorporating data collection, coding and analysis using a process of constant comparison without the theory development component (17).
Three authors (FMM, SOS and MSF) independently coded segments of phrases and labelled them into categories, and combined the categories into key themes. They used a combination of predetermined and emerging codes. Predetermined codes were based on the construct proposed by Reid’s model. In order to facilitate the codification process, we used the program MAXqda2 (18). The authors reviewed and compared their findings to form an agreement on categories. Three rounds of coding and discussion took place with the intention of enhancing credibility of the analysis used, and to develop clear themes and categories. This process was iterative with data collection, allowing new categories or themes to be inserted from the data of subsequent group transcripts. No new themes or categories emerged at the end of the seventh focus group, which implied that saturation was reached. Two researchers cross-checked their agreement through a blind review using codes for the same passages of 2 transcripts to check consistency of the final themes and categories (19). Any disagreements between the 2 researchers were resolved by discussion. Finally, the 3 researchers (FMM, SOS and MSF) interconnected the themes and categories. At every step, an independent researcher (PER) reviewed whether the analysis was systematically supported by the data with the intention of enhancing dependability (15). Confirmability was enhanced when the same categories emerged from the data of subsequent groups transcripts.
RESULTS
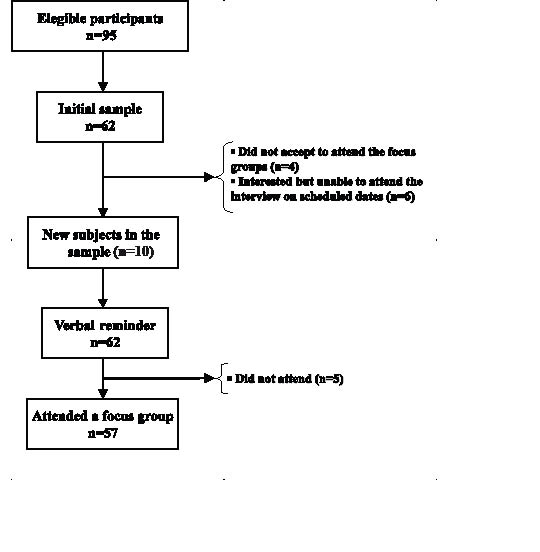
Sixty-two subjects were sampled from 95 eligible participants. Initially, 10 patients did not accept the invitation to attend the focus groups, or were unable to attend the interview on scheduled dates. Consequently, 10 new patients were added to the initial sample. Initially, 62 patients were interested in attending the meeting based on the verbal reminder, but not all of them participated in the focus groups. The stages of selection for the focus groups are shown in Fig. 1.
Fig. 1. Selection process for focus groups.
There were 57 subjects in this study (33 males, 24 females). Twenty-four subjects were over 45 years of age (Table I). All subjects reported that they had at least one experience that led them to perceive gaps in their continuity of care. These experiences were related to 1 of the 3 types of continuity of care (relational, informational and management). Thus, all experiences and perceptions are presented in the following themes: (i) relational continuity; (ii) informational continuity; and (iii) management continuity.
| Table I. Characteristics of patients |
| Characteristics | n (%) |
| Sex | |
| Male | 33 (57.9) |
| Female | 24 (42.1) |
| Age, years | |
| < 30 | 12 (21.1) |
| 31–45 | 21 (36.8) |
| > 45 | 24 (42.1) |
| Diagnosis | |
| Fractures | 28 (49.2) |
| Upper limb | 14 (24.6) |
| Lower limb | 14 (24.6) |
| Soft tissue injuries | 25 (43.8) |
| Shoulder | 11 (19.3) |
| Knee | 10 (17.5) |
| Others | 4 (7.0) |
| Amputation | 4 (7.0) |
Relational continuity
This theme focused on the ongoing therapeutic relationship between patients and rehabilitation providers as a mechanism to achieve connection of care during treatment. The importance of a good relationship with the rehabilitation team was a persistent theme within the subjects’ comments, and was also a key element in their own perception of continuity of care. The subjects perceived that the relational continuity was dependent on factors such as: (i) consistency of multi-professional rehabilitation team; and (ii) established provider–patient relationship.
Consistency of multi-professional rehabilitation team. Most patients received care from a team composed of one or more health providers who they could rely on during their rehabilitation. Rehabilitation teams composed of one physical therapist and one rehabilitation physician were mentioned most frequently, with some patients reporting more than one physical therapist or physician.
Subjects felt that consistency of providers within the rehabilitation team was very important. Having a consistent team enhanced the sense of safety, direction, and satisfaction with the rehabilitation process. In contrast, inconsistency in the team or provider who supervised their care throughout the whole rehabilitation process raised feelings of distrust, and perceptions that the progress of the rehabilitation process was impaired.
It is very good to always have the same professional who is constantly concerned about how I am, who explains how to do the exercise, such as: Put the foot this way, put the leg the other way, etc. It is like a support that makes you feel controlled, safe… (Female, 43 years, upper limb fracture).
When you have a change of physical therapist and another comes…, for example in vacations…, it feels different, because the new person does not know you, he/she does not want to move you much. It seems that your recovery is blocked. I prefer my physical therapist. (Male, 39 years, lower limb fracture).
Established provider–patient relationship. Patients usually felt that they had a good relationship with their providers during the whole period of treatment. Having a good relationship increased their sense of connection with care during treatment. However, for some patients, the consistency of a provider was not sufficient to ensure the relation of connection with their own care over time. Although they had the same provider, they attributed the loss of connection to a weak interpersonal relationship originating from low levels of communication during the treatment sessions.
In regards to physical therapists, it is more than just a professional–patient relationship, because it’s like they become part of your life, they tell you their stuff, they are interested in yours… and I like this because I feel that I do not have to remind him of my problems or preferences. (Female, 38 years, soft tissue knee injury).
There was always one physical therapist who attended my case, but this did not increase my confidence. He didn’t say anything, or give me incentives… he would arrive and pass the exercises, and nothing else. Sometimes I felt that, perhaps, he did not remember much of my problem. (Female, 52 years, soft tissue shoulder injury).
Informational continuity
This theme focused on the availability of information that providers had in order to provide appropriate care. Occasionally, patients presented a belief that their providers did not have the necessary information regarding prior events or circumstances. The subjects were of the opinion that the rehabilitation team’s acknowledgement of their experiences regarding their disability and treatment was as important as the actual biomedical information about health conditions, disabilities or treatments, to ensure that services were responsive to the patient’s needs.
According to the data, patients felt that informational continuity was dependent on factors such as: (i) transfer of information among providers; and (ii) accumulated knowledge regarding the patients’ experiences of disability.
Transfer of information among providers. Patients revealed some negative experiences with regards to the topic of information exchange among providers within the rehabilitation team. Problems with transfer of information among physical therapists and rehabilitation physicians were the most frequent. The lack of information was perceived when professionals affirmed that they were not acquainted with some information or circumstances and when practitioners planned interventions that had previously been suspended by another practitioner. Patients believed that the quality and safety of their treatment could be affected when sufficient information was not available to their providers.
The doctor who fixed this finger told me that I must not exert any effort for now or bend it, but the physical therapist who treated me was trying to bend the joint. She told me that she did not know anything about what the doctor told me, and that she would have a look at the X-ray. And you think: Do they talk with each other? (Male, 33 years, upper limb fracture).
The rehabilitation physician told me in a consultation: You are going to start rehabilitation today and you must stretch the leg (knee) as much as you can. Well, later he presented the physical therapist that would treat me, and the first thing she said was: What we must do is to bend the leg (knee), but do not stretch it, ah! (Female, 42 years, soft tissue knee injury).
Accumulated knowledge of patients’ disability experiences. Accumulated knowledge was related to a high frequency of follow-up treatments because it facilitated the communication and sharing of expertise about patients’ own experiences of disability and treatment. According to patients’ statements, regular physical therapists had more accumulated knowledge of their experiences of disability than did other professionals in the team (i.e. other physical therapists or physicians).
There is a reliance relationship with your physical therapist because he is the one who treats you, and the one who sees you daily. My physical therapist, at the time he touches my knee, already knows if I am feeling well or bad. He is aware of any problem. (Female, 48 years, lower limb fracture).
The professional who really knows you is the physical therapist because he is the one who sees you every day, sees your problem. In my case for example, since I have a wound, he knows how I am doing. (Male, 38 years, soft tissue knee injury).
Management continuity
This theme focused on the provision of separate types of healthcare delivered by the rehabilitation team over time, and how they complement each other. Patients often perceived that the care received from different providers was not connected in a coherent way. Moreover, patients also reported that their collaboration with the rehabilitation team was not exploited or coordinated. In fact, they felt themselves to be their own providers of self-management strategies and adherence to professionals’ advice. As far as patients were concerned, these gaps in continuity were dependent on: (i) consistency of care among rehabilitation providers; (ii) flexibility of the team in adapting care to functional changes or other needs; and (iii) involvement of the team in achieving collaboration with the patient.
Consistency of care among rehabilitation providers
Patients felt a lack of consistency of care in relation to content or synchronization of care between physicians and physical therapists, or even between physical therapists.
The patients usually reported a lack of consistency of care, in terms of therapy content or sequence of care among doctors and physical therapists, or even among physical therapists. The lack of consistency of therapy content was detected when the content of the therapy plan was not sufficiently shared within the rehabilitation team. As a result, this lack of consistency was perceived as a consequence of low interaction among providers, or as an explicit disagreement with the other provider’s opinion. The awareness of a discoordinated implementation of care inclined patients to feel anxious and prompted them to form the opinion that their rehabilitation process was affected.
We have two physical therapists: one in the morning and another in the evening. The one who comes in the morning instructs me to perform some exercises, and the other gives different instructions. One says that exercises in the pool are good for me and the other says the contrary. That worries me, because in the end you no longer know what is better. (Male, 48 years, amputation).
Likewise, inadequate sequencing of care was noticed when different activities delivered by the rehabilitation team occurred at the same time as physical therapy sessions. Some patients reported that rehabilitation physicians often scheduled their follow-up visits during the physical therapy slot, which had been arranged previously. They also reported that they felt some negatives consequences regarding implementation of physical therapy, and reported a low level of satisfaction.
The consultations with the rehabilitation doctor frequently coincide with the physical therapy session. I don’t agree with that because on that day you don’t have enough time to do physical therapy and the treatment you were receiving is interrupted. (Female, 60 years, soft tissue shoulder injury).
Flexibility of the team in adapting care to patient’s functional changes and other needs. Patients were aware that the rehabilitation team often adapted the treatment or advice to functional changes or specific circumstances that happened during their rehabilitation progression. However, some patients felt that this response was delayed. Consequently, this delay was identified as a stopping point in their rehabilitation process.
On the day I told my physiotherapist that I was having a lot of pain and that I was not feeling very well. He said: Well, so we are not going to force it too much today. In my case, he assessed the situation I had with my arm and kept molding the treatment. You see, they are not rigorous, they adapt to what you feel at the moment… (Female, 44 years, upper limb fracture).
I was doing the same treatment for 3 weeks, walking from side to side in the swimming pool. Every day I asked the physiotherapist what I should do next and he answered: ‘Do the same, the same, walking…’ Until the day I came to him and said: ‘Only walking? I can do much more!’ Then he changed the exercises. (Male, 35 years, lower limb fracture).
Involvement of the team in achieving patient collaboration. Subjects considered the explicit request to collaborate over their plan of care relevant, and valued information on activity restrictions, warning symptoms, possible side-effects, follow-up timetables, etc. However, they often felt that their rehabilitation providers did not seek their collaboration with the plan of care. The absence of patient education was perceived to be important, because some patients experienced adverse effects derived from inadequate exercises.
A good thing I find here is that they give you a list so that you help yourself in your recovery. They teach you how to do the exercises, and explain the most correct way to do them, etc. (Male, 56 years, soft tissue shoulder injury).
…the physical therapist always used to say: When you are discharged, continue to do the exercises at home, at least 15 or 20 min daily, especially for your problem of degenerative arthritis. This leg needs to be very strong… (Female, 55 years, soft tissue knee injury).
One day I got up from the bed to do the standing up exercises. I put my leg down, but I couldn’t maintain it, so I hurt it. I believe that this happened because I forced myself to do something that I was not yet prepared. How could I know..? But if they teach you in another way, for example, holding the parallel bars with more support, then you take more care and collaborate more. (Male, 23 years, soft tissue knee injury).
DISCUSSION
This qualitative study of patients’ perspective of continuity in rehabilitation found that patients experienced a sense of non-connected care over time while attending post-acute rehabilitation. This negative experience of continuity related to their perceptions of inconsistency or interrupted relationships with a team, and that some providers were not aware of prior events or experiences with their disability, or that providers disagreed on a management plan or in adapting their care to changes in their individual needs.
Patients’ concerns in relation to their experience of continuity have been identified in rehabilitation settings, either using the Reid’s model with cardiac patients (20) or using the client-centered philosophy (21). From this last perspective, continuity is viewed as a client knowing the roles and responsibilities of each team member at each stage of rehabilitation (22). Nevertheless, our study was based on a global model (10) and provided a wider view of the experience of continuity of care for post-acute rehabilitation settings.
We noticed that the patients in our study commented on experiences of discontinuity dependent on all 3 aspects of continuity of care (relational, informational and management) previously identified by Reid et al. (10) in a literature review conducted on behalf of the Canadian Health Research Foundation and other organizations. Our study provides empirical support to the Reid model of continuity of care, based on the patients’ experiences in rehabilitation post-acute care.
The aspects that led to gaps in continuity of rehabilitation care were different for each type of continuity. Most of these aspects were similar to those in the Reid model (10). In this model, management continuity is achieved when services are consistent and flexible; informational continuity depend on transference of documented information but also on accumulated knowledge about patient’s preferences and context; and relational continuity is achieved when an ongoing therapeutic relationship exists. However, small differences in these aspects were identified, which were essentially derived from their specific application in the rehabilitation field. For example, where Reid et al. identified “accumulated knowledge” and “flexibility”, we identified “accumulated knowledge of patients’ disability experiences” and “flexibility of team in adapting care to the patients’ functional changes”, respectively. In addition, the other aspect relevant for continuity identified in our study: “involvement of the team in achieving patient’s collaboration”, was not included in Reid et al.’s study. This aspect confirms the idea supported by some authors about the patients’ desire to collaborate in the management of their own problem (23).
When there was an absence of some relevant aspects of continuity, patients perceived a stopping point in their rehabilitation process, and expressed feelings of loss of coherence in the treatment. One situation that exemplifies this feeling was when patients observed a lack of consistency between providers or in the content of care. Additionally, patients had feelings of distrust about the quality of care that they were receiving. In fact, our participants provided a connection between perception of continuity and quality of care. Both aspects, quality and continuity, are concepts that originated from the literature (24). There are a few discussions about the relationship of these two aspects. Some authors believe that quality of care requires continuity (25, 26). Conversely, other authors consider that continuity is not an attribute of providers or organizations, but an attribute of how an individual patient experiences the integration of services and coordination (11).
The absence of some relevant aspects of continuity are related to negative consequences, such as feelings of mistrust or frustration, whereas the presence of these aspects of continuity are associated with satisfaction. These findings are consistent with previous studies. Equally, continuity of care has been related to satisfaction in many other studies (27–29). Although our study did not identify additional benefits, the literature shows that continuity of care has multiple benefits for quality of life (30), patient adherence (31) and decreased use of post-hospitalization services (32).
Most of the gaps presented by the patients within the 3 types of continuity of rehabilitation care indicate that there are many aspects that are modifiable and therefore amendable to practice improvement. Professionals should have an awareness of the relevance of interpersonal communication, as a means of achieving connection of care during the entire rehabilitation period. Examples include the promotion of patient-accumulated knowledge, support for the provider–patient relationship, and patient participation in self-management strategies. The rehabilitation team should share consistent information over time, and improve the coordination of consensual therapeutic plans.
Limitations of this study include the cross-sectional design, and the lack of patients with neurological disorders (i.e. stroke, brain injury, etc.) or presenting complex conditions (i.e. cardiopulmonary conditions, impairment resulting from illness, etc.). It is possible that the experiences presented by patients with musculoskeletal disorders were slightly different from those that would be presented by patients with different disorders. However, since more than 90% of the subjects in the 3 selected centers presented with musculoskeletal condition this was beyond our control. Secondly, the study was cross-sectional and retrospective. It is possible other study designs would allow the subjects to provide a more detailed perspective of their experiences. Therefore, longitudinal and prospective studies that include patients with different health conditions and follow the patients throughout the entire rehabilitation process may offer additional understanding about what promotes or detracts from the continuity of rehabilitation care.
Finally, given the sample size and the fact that the focus groups were conducted in only 3 post-acute care settings, we should not generalize our conclusions from the results presented in this study. Nevertheless, our results are highly consistent with other studies that have examined continuity of care in other contexts (33, 34). Not only quantitative, but also qualitative studies are necessary in order to generalize our results to a broader theory (35).
Although there were limitations to this study, the methodology used was controlled. Methodological rigor was enhanced by multiple and coordinate coding and cross-checked codes developed by different researchers when comparing results (36). The principal investigator’s personal and intellectual biases were minimized by using a research assistant for the interviews, by allowing open-questions to develop the interviews naturally, and by reporting on a wide range of perspectives.
In conclusion, within the known limitations, patients often perceive that their experiences in rehabilitation care are non-connected or non-coherent over time. When these experiences occurred, the patients felt that the quality or safety of their treatment could be affected. Providers’ interpersonal skills, transfer of information among providers and patients in order to maintain mutual collaboration, and coordination of care among providers and patients were reported as conditions that influence continuity of care.
Improvements in the continuity of rehabilitation care are possible because most of the issues described by subjects are, at least in part, within the power of clinicians and rehabilitation care organizations to improve. Future studies should not only test the validity of the many associations identified between relevant aspects and the perception of gaps in continuity, but should also measure continuity and test possible associations between continuity of care and clinical outcomes or safety in post-acute care.
Acknowledgements
This study was supported by Health Research Fund from Carlos III Health Institute, Ministry of Health (project number PI060836), Spain.
References