OBJECTIVE: To analyse factors associated with late return to work in road accident victims.
Materials and methods: The ESPARR cohort comprises road accident victims monitored over time from initiation of hospital care. A total of 608 ESPARR cohort subjects were working at the time of their accident and answered questionnaires at 6 months and/or 1 year. For each level of overall severity of injury (Maximum – Abbreviated Injury Scale (M-AIS) 1, 2, 3 and 4–5), a time-off-work threshold was defined, beyond which the subject was deemed to be a late returner; 179 subjects were considered to be late in returning to work, while 402 showed a normal pattern of return. Logistic regression identified factors associated with late return.
RESULTS: Type of journey, overall injury severity and intention to press charges emerged as factors predictive of late return to work on the basis of the data collected at inclusion alone. After adjustment, pain (odds ratio (OR): 2.6; 95% confidence interval (95% CI) 1.0–6.7) and physical sequelae (OR: 3.8; 95% CI 1.7–8.3) at 6 months and the fact of pressing charges (OR: 2.6; 95% CI 1.2–5.5) remained significantly linked with late return to work.
CONCLUSION: Impaired health status at 6 months after the initial accident (in the form of persistent pain and physical sequelae) is a determining factor delaying return to work following a road traffic accident.
Key words: return to work; road traffic accident; cohort; injury.
J Rehabil Med 2011; 43: 283–291
Correspondence address: Martine Hours, INRETS, 25 Avenue François Mitterrand, FR-69500 Bron Cedex, France. E-mail: martine.hours@inrets.fr
Submitted June 25, 2007; accepted November 12, 2010
Introduction
Road traffic accidents have serious consequences for both the individual and society, yet little is known about their impact on victims’ lives.
Accident-related traumatic lesions often require an individual to take sick leave while health status recovers. On the other hand, prolonged sick leave may have harmful consequences, related to chronicization and socioprofessional marginalization. Return to work is a complex issue, depending on the individual, the pathology, rehabilitation and the socioeconomic environment. It is a determining factor in quality of life. Non-return to work also represents a serious social cost, in terms of care provision, sick leave and absenteeism. Return to work thus involves a range of issues, and has been the focus of much research. Krause et al. (1), in a review of the literature, highlighted the gaps in the field: understanding the causes and predictive factors involved in the process is an essential step towards developing prevention strategies. They identified, in this regard, 100 predictive factors that may influence return to work. Since this time, there has been much discussion on the importance of each factor: for example, Clay et al. (2) in a meta-analysis on orthopaedic injuries showed that there is always moderate to inconsistent evidence that age, sex and injury severity are prognostic factors, while there is a consensus concerning the level of education or the type or job (blue-collar/white-collar). Psychosocial factors (such as the psychological demand of work, high-stress work, etc.) (3, 4) or psychological factors (5) have been explored extensively. However, these studies have focused on back pain, and there have been very few studies of trauma.
Wasiak et al. (6) stressed the lack of knowledge on the subject of return to work. Return to work was here not merely a stage, but a complex process in itself, and a concept comprising 4 phases was drawn up: before returning, reintegrating the work environment, staying at work, and long-term evolution at work. Depending on the context and objectives of any given study, the focus may be on one or the other of these phases. Wasiak sought to develop a more systematic and comprehensive approach to the assessment of return to work. Chamberlain et al. (7), in a more recent paper, stressed the importance of vocational rehabilitation in a continuum from the acute phase to the return to work, even after the return to the labour market. The sooner this rehabilitation is provided by a multiprofessional team, the better the result in terms of cost-benefit.
The objective of the present study was to determine predictive factors of “late” (from the point of view of prolonged sick leave) return to work in road accident victims. It is based on the data of the ESPARR cohort (ESPARR is a follow-up study of a population of road accident victims in the Rhône administrative département of France: Etude de Suivi d’une Population d’Accidentés de la Route dans le Rhône), collected at the time of the accident and in the post-accident phase (8).
MaterialS and methods
ESPARR cohort
ESPARR is a study of a cohort of road accident victims that aims to shed light on the various consequences of the accidents. Inclusion criteria are: (i) having had a road accident in the Rhône administrative département of France involving at least one mechanical means of transport; (ii) being resident in the Rhône département; (iii) consulting in a healthcare centre in the département; and (iv) being alive on arrival at hospital.
Due to the great disproportion between mild and severe injuries, different survey fractions were applied according to initial lesion severity, as coded on the Abbreviated Injury Scale (AIS) (9). The AIS scores lesions from 1 (minor) to 5 (critical). Coding was performed by trained physicians from the initial injury report issued by the hospital. The Maximum-AIS (M-AIS) is the highest AIS score recorded in the case of multiple trauma. The objective was to recruit all cases of severe lesion (M-AIS ≥ 3) and 1 in 6 cases of mild to moderate lesion (M-AIS < 3). Body sections were those of the AIS (head, face, neck, thorax, abdomen, spine, superior limb, inferior limb, external lesions). Recruitment lasted from October 2004 to July 2006. The ESPARR cohort comprises 1373 subjects, including 1112 working age subjects (age range 16–64 years) and has been described in detail elsewhere (8).
Written informed consent was obtained from the patient or the next of kin at inclusion. The study was approved by French committees concerned with ethics and medical information.
During the inclusion phase, investigators conducted interviews focusing on the accident and prior health status and family and work characteristics. These interview data were completed by the initial lesion assessment provided by the hospital departments. Cohort subjects were asked to participate in a 6-month (Q6m) then a 12-month (Q1y) follow-up in the form of a self-administered questionnaire, sent by post, investigating the subject’s opinion of his/her overall state of health. In the case of non-response, a telephone call was made in order to complete the questionnaire with the patient.
Variables and measurement tools
The variables studied at inclusion and during the post-accident phase were of several types (8). Briefly, for this analysis, the following variables were used:
• sociodemographic: gender, age, educational level, family status, socioprofessional group;
• accident-related: type of road user, type of journey, time of accident, circumstances of the accident, responsibility in the accident (10), intention to press charges against accident opponent;
• prior health status; several questions asked about chronic pathologies and/or pathologies in the previous year. The team physician (MH) coded blindly in several categories of “co-morbidities” (cardiovascular, metabolic, pulmonary, otorhynolaryngology, orthopaedic, substance abuse);
• initial care: treatment in a resuscitation room and/or intensive care, AIS, Injury Severity Score (ISS): sum of the squares of the AIS severity scores for the 3 most severe lesions in 3 different body sections), loss of consciousness at accident, cranial trauma, multiple trauma;
• information on work: sick leave, date of return (complete or partial return), significant changes in the job (employers, type, full- or part-time work, work facilities.), description of the job if different than that at the moment of the accident;
• post-traumatic stress disorder (PTSD) assessed by a French validated translation of Post-traumatic Check-list Scale (PCSL) (11): a score equal or above 44 indicates the presence of PTSD;
• consequences at 6 months: hospital admission following accident, rehabilitation centre referral, pain (visual analogue scale) and subjective medical status at 6 months.
Definition of return to work
There is no consensual definition of “return to work” in the literature. Several authors, however, have suggested that it is important to take account of the duration of sick leave in assessing return to work (6, 12) and to adjust the period of disability with respect to the lesion and its severity (13). The present study therefore distinguished “normal” and “late” return to “remunerative” work in terms of sick leave duration adjusted on the M-AIS severity score (4 groups: M-AIS 1, 2, 3 and 4–5). Sick leave duration was calculated from the date of the accident to the date of complete or partial return to work stated in Q6m and/or Q1y. The distribution of time to return to work varied greatly according to M-AIS group: (M-AIS1: mean = 46 days (standard deviation (SD) 76); med = 19 (q1–q3: 9–42)) (M-AIS2: mean = 90 days (94); median = 61 (22–108)) (M-AIS3: mean = 167 days (126); median = 131 (79–225)) (M-AIS4-5: mean = 138 days (104); median = 116 (58–190)), especially when the time off work was long. The 4 thresholds were determined after a comparison of our data with other observations: a validation survey of 30 physicians in the Lyon area of France, and the French national health insurance (Sécurité Sociale) intended to harmonize sick leave in work-accident victims (14). For 3 severity scores, the upper quartile of time to return to work was therefore taken as the threshold beyond which the return counted as “late”: 42 days for M-AIS1, 108 for M-AIS2, and 190 for M-AIS4/5). For M-AIS3, the threshold was set at the median value of 131 days, which was closer to the data provided by the two above validation studies than the upper quartile.
Study population
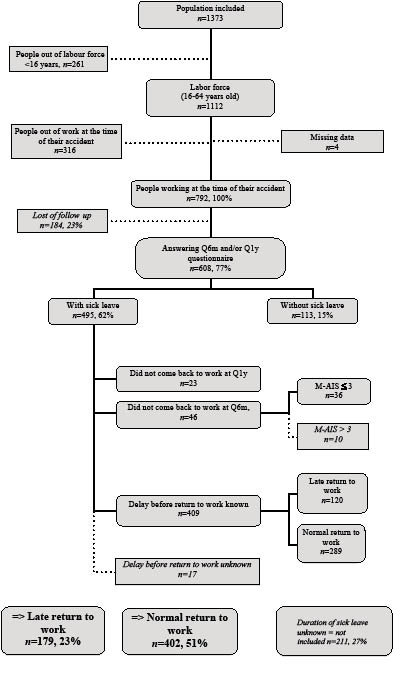
A total of 792 of the 1112 working age (age range 16–64 years) subjects in the ESPARR cohort were working at the time of their accident, and constituted the target population. Of these, 608 (76.8%) answered the Q6m and/or Q1y questionnaire. Return-to-work status could be determined for 581 subjects (95.6%, or 73.4% of the target population) (Fig. 1); time to return to work could not be determined for 27 subjects: 10 M-AIS4-5 subjects had not returned to work at 6 months, but then failed to answer Q1y and could thus not be classified as normal or late returners, and 17 subjects who had returned to work failed to give the date of their return.
Fig. 1. Study population selection flowchart. Twenty-seven subjects for whom time to return to work could not be assessed were excluded from the study. Normal return = 113 subjects without sick leave + 289 subjects with sick leave and normal return. Late return = 23 subjects not working at 1 year (Q1y) + 36 M-AIS ≤ 3 subjects not working at 6 months (Q6m) + 120 subjects returning to work later than would be expected. M-AIS: Maximum-Abbreviated Injury Scale.
Statistical analysis
Step 1 of the statistical analysis assessed study population representativeness by comparing study subjects with cohort subjects who did not answer Q6m.
A descriptive step then characterized the study population and compared proportions according to return-to-work status, on χ2 test. The Student t-test was used to compare means.
An explanatory step used weighted logistic regression to identify risk factors for late return to work.
The SAS 9.1 SURVEYLOGISTIC procedure (SAS Institute Inc., Cary, NC, USA) was used to take into account the ESPARR cohort survey plan, which was stratified by severity into two levels: M-AIS < 3 and M-AIS ≥ 3. For each stratum, weight was the number of injured in a road traffic accident in the Rhône administrative départements divided by the number of victims selected in the study.
Two independent multivariate models were constructed, to study respectively variables at inclusion (data directly following the accident) and health variables on the Q6m questionnaire. Variables correlating (p < 0.1) with the outcome on univariate analysis were selected for each model. Multivariate analysis selected factors significantly associated with outcome, using a backward elimination procedure for excluding variables without significant links (p > 0.05). Confounding factors were checked at each stage of model construction and potential interactions between explanatory variables in the final model were tested. Lastly, only adjustment variables significant at the 5% level were retained in the final model.
The main lesions were then analysed independently with outcome after adjustment on the second multivariate model. In that final step, patients with multiple trauma could appear in several analyses.
Results
Description according to return-to-work status
Compared with the 581 subjects who answered the Q6m and/or Q1y questionnaires, the 184 who were lost to follow-up and the 27 who were excluded from analysis (their date of return to work not being known) were slightly younger (31.2 vs 34 years; p = 0.001), had a lower educational level (63% vs 50% below the baccalaureate, which is equivalent to secondary school leaving certificate, p < 0.01), were less often cyclist victims (4.3% vs 10.7%, p < 0.05) and sustained milder injuries (54% vs 46% M-AIS1; p = 0.001). No other significant differences in sociodemographic factors or initial medical care emerged.
Twenty-three percent of the subjects who were working at the time of their accident (i.e. 30.8%; 179/581 of the study population) returned to work late after their accident (Fig. 1). Table I presents sociodemographic, accident-related and medical characteristics according to return-to-work status (normal or late). The gender distribution was similar in the two groups. Late returners had significantly lower educational levels. Motorized two-wheel vehicle users and victims who had a work-related accident were significantly more frequently late returners. Intention to press charges was also more frequent in the late return to work group.
Admission to a resuscitation room or intensive care, cranial trauma, ISS score > 9 and multiple trauma were significantly more frequent in the late return to work group; as were hospital admission, surgery and medical complications in the post-accident phase (Table II). At 6 months, pain, physical or psychoneurological sequelae and PTSD were significantly more frequent in the late return to work group.
|
Table I. General study population characteristics at time of accident, according to return-to-work status (univariate logistic regression; SAS 9.1 SURVEYLOGISTIC procedure)
|
|
|
Late return (n = 179)
n (%)
|
Normal return (n = 402)
n (%)
|
Raw OR
|
95% CI
|
p-value
|
|
Sociodemographic data
|
|
Gender
|
NS
|
|
Males
|
119 (66.5)
|
254 (63.2)
|
1
|
–
|
|
|
Females
|
60 (33.5)
|
148 (36.8)
|
0.9
|
0.6–1.4
|
|
|
Age group, years
|
NS
|
|
< = 34
|
96 (53.6)
|
229 (57.0)
|
1
|
–
|
|
|
> 34
|
83 (46.4)
|
173 (43.0)
|
1.2
|
0.8–1.9
|
|
|
Family status
|
NS
|
|
Single
|
67 (37.4)
|
172 (42.8)
|
1
|
–
|
|
|
Married
|
91 (50.9)
|
188 (46.8)
|
1.1
|
0.7–1.7
|
|
|
Divorced
|
21 (11.7)
|
42 (10.4)
|
1.2
|
0.6–2.5
|
|
|
Educational level
|
NS
|
|
Higher or equivalent than baccalaureate school leaving certificate
|
76 (42.5)
|
216 (53.7)
|
1
|
–
|
|
|
Lower than baccalaureate school leaving certificate
|
103 (57.5)
|
186 (46.3)
|
1.4
|
0.9–2.1
|
|
|
SEC
|
NS
|
|
Farmers, self-employed craftsmen, CEOs, executives
|
12 (6.7)
|
27 (6.7)
|
1.0
|
0.4–2.4
|
|
|
Intellectual and liberal professions
|
15 (8.4)
|
60 (14.9)
|
0.6
|
0.3–1.1
|
|
|
Intermediate profession
|
16 (8.9)
|
47 (11.7)
|
0.6
|
0.3–1.3
|
|
|
Office-workers, etc.
|
94 (52.5)
|
194 (48.3)
|
1
|
–
|
|
|
Blue-collar workers (in general)
|
36 (20.1)
|
57 (14.2)
|
1.1
|
0.6–2.0
|
|
|
Technical cooperative diploma
|
6 (3.4)
|
17 (4.2)
|
0.5
|
0.1–1.5
|
|
|
Accident-related data
|
|
Type of road user
|
NS
|
|
Four-wheel
|
77 (43)
|
195 (48.5)
|
1
|
–
|
|
|
Motorbike
|
70 (39.1)
|
120 (29.9)
|
1.5
|
0.9–2.4
|
|
|
Bicycle
|
12 (6.7)
|
50 (12.4)
|
0.7
|
0.3–1.5
|
|
|
Pedestrian
|
20 (11.2)
|
37 (9.2)
|
1.2
|
0.6–2.4
|
|
|
Type of journey
|
< 0.05
|
|
Personal
|
83 (46.6)
|
233 (58.0)
|
1
|
–
|
|
|
Professional
|
95 (53.4)
|
169 (42)
|
1.6
|
1.1–2.5
|
|
|
Responsibility
|
|
No
|
125 (69.8)
|
273 (67.9)
|
1
|
–
|
NS
|
|
Yes
|
43 (24.0)
|
115 (28.6)
|
0.78
|
0.5–1.3
|
|
|
Do not know/not asked
|
11 (6.2)
|
14 (3.5)
|
0.77
|
0.3–2.1
|
|
|
Intention to press charges
|
< 0.0001
|
|
No
|
73 (40.8)
|
233 (58.0)
|
1
|
–
|
|
|
Yes
|
48 (26.8)
|
41 (10.2)
|
3.3
|
1.9–5.9
|
|
|
Do not know/not asked
|
58 (32.4)
|
128 (31.8)
|
1.0
|
0.6–1.6
|
|
|
Medical data
|
|
Treatment in resuscitation room, yes
|
35 (19.5)
|
33 (8.2)
|
2.5
|
1.3–4.8
|
< 0.01
|
|
Intensive care, yes
|
21 (11.7)
|
24 (6.0)
|
3.4
|
1.6–7.7
|
< 0.01
|
|
Cranial trauma, yes
|
88 (49.2)
|
150 (37.3)
|
1.3
|
0.9–2.0
|
NS
|
|
Whiplash, yes
|
33 (18.4)
|
104 (25.9)
|
0.8
|
0.5–1.3
|
NS
|
|
ISS
|
|
≤ 8
|
149 (83.2)
|
371 (92.3)
|
1
|
–
|
< 0.001
|
|
9–15
|
18 (10.1)
|
17 (4.2)
|
3.4
|
1.9–6.1
|
|
|
≥ 16
|
12 (6.7)
|
14 (3.5)
|
2.7
|
1.4–5.4
|
|
|
M-IIS
|
< 0.001
|
|
0
|
41 (22.9)
|
177 (44.0)
|
1
|
–
|
|
|
1
|
105 (58.7)
|
200 (49.8)
|
1.71
|
1.1–2.7
|
|
|
2–5
|
33 (18.4)
|
25 (6.2)
|
5.11
|
2.3–11.3
|
|
|
Multiple trauma, yes
|
126 (70.4)
|
215 (53.5)
|
1.8
|
1.2–2.7
|
< 0.01
|
|
95% CI: 95% confidence interval; OR: odds ratio; NS: non-significant; SEC: socio-economic category; CEO: chief executive officers; ISS: Injury Severety Score; M-IIS: Maximum injury impairment scale.
|
|
Table II. Medical data collected at 6 months according to return-to-work status (univariate logistic regression; SAS 9.1 SURVEYLOGISTIC procedure)
|
|
|
Late return
n (%)
|
Normal return
n (%)
|
Raw OR
|
95% CI
|
p-value
|
|
Hospital admission
|
< 0.001
|
|
None
|
35 (23.5)
|
163 (56)
|
1
|
–
|
|
|
Simple admission
|
24 (16.1)
|
68 (23.4)
|
1.6
|
0.9–3.1
|
|
|
Admission with surgery
|
90 (60.4)
|
60 (20.6)
|
6.9
|
3.9–12.3
|
|
|
Medical complications, yes
|
31 (26.1)
|
17 (9.2)
|
3.5
|
1.5–8.3
|
< 0.01
|
|
Subjective medical status at 6 months
|
< 0.001
|
|
Full recovery
|
15 (12.8)
|
94 (40.5)
|
1
|
–
|
|
|
Improved/not recovered
|
76 (65)
|
108 (46.6)
|
3.8
|
1.9–7.5
|
|
|
Stable/worsened
|
26 (22.2)
|
30 (12.9)
|
4.8
|
2.0–11.2
|
|
|
Persistent pain, yes
|
113 (92.6)
|
158 (66.1)
|
5.1
|
2.3–11.3
|
< 0.001
|
|
Physical sequelae, yes
|
95 (78.5)
|
123 (52.6)
|
5.5
|
2.8–10.9
|
< 0.001
|
|
PTSD, yes
|
32 (29.4)
|
26 (11.5)
|
2.6
|
1.3–5.1
|
< 0.01
|
|
95% CI: 95% confidence interval; OR: odds ratio; PTSD: post-traumatic stress disorder.
|
Explanatory analysis
The multivariate model founded on inclusion data alone identified 3 predictive factors for late return to work: work-related accident, intention to press charges, and ISS score > 9 (Table III).
|
Table III. Factors associated with late return-to-work status (factors collected on recruitment) (weighted multivariate logistic regression; SAS 9.1 SURVEYLOGISTIC procedure) (total number of subjects not equal to 581 due to missing data)
|
|
|
Late return
n (%)
|
Normal return
n (%)
|
Adjusted OR
|
95% CI
|
p-value
|
|
Gender
|
|
|
|
|
|
|
|
|
Males
|
118 (66.3)
|
254 (63.2)
|
1
|
–
|
|
|
Females
|
60 (33.7)
|
148 (36.8)
|
1.04
|
0.64–1.70
|
|
|
Age group, years
|
96 (83.9)
|
229 (57.0)
|
1
|
–
|
|
|
≤ 34
|
82 (46.1)
|
173 (43.0)
|
1.26
|
0.78–2.02
|
|
|
> 34
|
|
|
|
|
|
|
|
|
Educational level
|
|
|
|
|
|
|
|
|
Higher or equivalent than baccalaureate school leaving certificate
|
76 (42.7)
|
216 (53.7)
|
1
|
–
|
|
|
Lower than baccalaureate school leaving certificate
|
102 (57.3)
|
186 (46.3)
|
1.09
|
0.68–1.77
|
|
|
SEC
|
|
|
|
|
|
|
|
|
Farmers, self-employed craftsmen, CEOs, executives
|
12 (6.7)
|
27 (6.7)
|
0.75
|
0.30–1.88
|
|
|
Intellectual and liberal professions
|
15 (8.4)
|
60 (14.9)
|
0.48
|
0.22–1.05
|
|
|
Intermediate profession
|
16 (9.09
|
47 (11.7)
|
0.56
|
0.25–1.25
|
|
|
Office-workers, etc.
|
94 (52.8)
|
194 (48.3)
|
1
|
–
|
|
|
Blue-collar workers (in general)
|
35 (19.7)
|
57 (14.2)
|
1.27
|
0.67–2.41
|
|
|
Technical cooperative diploma
|
6 (3.4)
|
17 (4.2)
|
0.48
|
0.14–1.58
|
|
|
Type of journey
|
|
|
|
|
|
|
< 0.05
|
|
Personal
|
83 (46.6)
|
233 (58.0)
|
1
|
–
|
|
|
Professional
|
95 (53.4)
|
169 (42.0)
|
1.68
|
1.07–2.65
|
|
|
ISS
|
|
|
|
|
|
|
< 0.001
|
|
≤ 8
|
89 (50.0)
|
300 (74.6)
|
1
|
–
|
|
|
9–15
|
60 (33.7)
|
71 (17.7)
|
1.66
|
0.99–2.78
|
|
|
≥ 16
|
29 (16.3)
|
31 (7.7)
|
3.64
|
2.04–6.51
|
|
|
Intention to press charges
|
|
|
|
|
|
|
< 0.001
|
|
No
|
73 (41.0)
|
233 (58.0)
|
1
|
–
|
|
|
Yes
|
48 (27.0)
|
41 (10.2)
|
3.38
|
1.83–6.23
|
|
|
Don not know/not asked
|
57 (32.0)
|
128 (31.8)
|
0.96
|
0.58–1.58
|
|
|
95% CI: 95% confidence interval; OR: odds ratio; NS: non-significant; ISS: Injury Severety Score; SEC: socio-economic category; CEO: chief executive officers.
|
The multivariate model founded on inclusion plus 6 months’ data also identified 3 predictive factors for late return to work: having pressed charges, pain at 6 months, and physical sequelae at 6 months (Table IV). Work-related accident was no longer significantly associated with late return to work, but this factor modified pain at 6 months interpretation; pain at 6 months was not significant in the modelling without work-related accident. Colinearity was verified and was null. Interaction of these two variables was not significant.
|
Table IV. Factors associated with late return-to-work status (factors collected on recruitment and medical or subjective conditions observed at 6 months) (total number of subjects not equal to 581 due to missing data and non-responses to 6 months)
|
|
|
Late return
n (%)
|
Normal return
n (%)
|
Adjusted OR
|
95% CI
|
p-value
|
|
Gender
|
|
NS
|
|
Male
|
64 (61.5)
|
122 (58.1)
|
1
|
–
|
|
|
Female
|
40 (38.5)
|
88 (41.9)
|
1.32
|
0.66–2.63
|
|
|
Age group, years
|
|
NS
|
|
≤ 34
|
56 (53.9)
|
107 (51.0)
|
1
|
–
|
|
|
> 34
|
48 (46.1)
|
103 (49.0)
|
0.75
|
0.37–1.54
|
|
|
Educational level
|
|
NS
|
|
Higher or equivalent than baccalaureate school leaving certificate
|
51 (49.0)
|
127 (60.5)
|
1
|
–
|
|
|
Lower than baccalaureate school leaving certificate
|
53 (51.0)
|
83 (39.5)
|
1.11
|
0.57–2.17
|
|
|
SEC
|
|
NS
|
|
Farmers, self-employed craftsmen, CEOs, executives
|
8 (7.7)
|
13 (6.2)
|
1.08
|
0.22–5.38
|
|
|
Intellectual and liberal professions
|
8 (7.7)
|
34 (16.2)
|
0.37
|
0.11–1.25
|
|
|
Intermediate profession
|
11 (10.6)
|
27 (12.9)
|
0.60
|
0.19–1.86
|
|
|
Office-workers, etc.
|
57 (54.8)
|
104 (49.5)
|
1
|
–
|
|
|
Blue-collar workers (in general)
|
17 (16.3)
|
27 (12.9)
|
1.52
|
0.51–4.50
|
|
|
Technical cooperative diploma
|
3 (2.9)
|
5 (2.3)
|
0.68
|
0.10–4.64
|
|
|
Type of journey
|
|
NS
|
|
Personal
|
119 (56.7)
|
46 (44.2)
|
1
|
–
|
|
|
Professional
|
91 (43.3)
|
58 (55.8)
|
1.71
|
0.87–3.36
|
|
|
Pressed charges
|
|
< 0.05
|
|
No
|
43 (41.3)
|
27 (12.9)
|
1
|
–
|
|
|
Yes
|
48 (46.2)
|
165 (78.6)
|
2.95
|
1.36–6.37
|
|
|
No answer
|
3 (2.9)
|
3 (1.4)
|
1.84
|
0.62–5.48
|
|
|
Don’t know
|
10 (9.6)
|
15 (7.1)
|
3.53
|
0.36–34.51
|
|
|
Persistent pain
|
|
< 0.05
|
|
No
|
7 (6.7)
|
72 (34.3)
|
1
|
–
|
|
|
Yes
|
97 (93.3)
|
138 (65.7)
|
2.62
|
1.04–6.60
|
|
|
Physical sequelae
|
|
< 0.001
|
|
No
|
13 (12.5)
|
97 (46.2)
|
1
|
–
|
|
|
Yes
|
82 (78.9)
|
108 (51.4)
|
4.64
|
2.10–10.28
|
|
|
Don not know
|
9 (8.6)
|
5 (2.4)
|
5.91
|
1.35–25.91
|
|
|
95% CI: 95% confidence interval; OR: odds ratio; NS: non-significant; SEC: socio-economic category; CEO: chief executive officers.
|
|
Lesions
Table V presents the main lesions associated with late return to work, after adjustment on the second multivariate model (see above: Statistical analysis). The late return to work group more frequently included mild cranial trauma, severe head lesion (excepting fracture without intracranial lesion), severe thoracic lesion, severe upper-limb fracture (AIS-3: 11.2% vs 5.2%), severe lower-limb fracture (AIS-3: 22.9% vs 5.5%) and spinal lesion. Only severe lower-limb lesion, severe thoracic lesions and cranial trauma (whether mild or severe) showed association after adjustment on the final model. Spinal lesion (fracture or other) was more frequent in late returners (15.6% vs 4.2%), but showed no significant association after adjustment (odds ratio (OR) = 2.1; 95% CI = 0.8–5.3), the calculations were based on few subjects (n = 13).
|
Table V. Lesion characteristicsa according to return-to-work status (multivariate logistic regression adjusted on gender, age group, educational level, professional status, type of journey, having pressed charges at 6 months, persistent pain, physical sequelae)
|
|
|
Late return
n (%)
|
Normal return
n (%)
|
p-value χ2
|
Adjusted OR
|
95% CI
|
p-value
|
|
Head lesion
|
|
|
|
|
|
|
|
|
|
Mild cranial trauma (AIS-1)
|
43 (24.0)
|
70 (17.4)
|
NS
|
3.0
|
1.3–6.5
|
< 0,01
|
|
Lesion other than fractureb (AIS-3)
|
9 (5.0)
|
4 (1.0)
|
p < 0.01
|
4.8
|
1.3–17.0
|
< 0.05
|
|
Thoracic lesion
|
|
|
|
|
|
|
|
|
|
Contusion of lung (AIS-3)
|
16 (8.9)
|
8 (2.0)
|
p < 0.001
|
9.9
|
1.9–50.8
|
< 0.01
|
|
Other thorax lesion (AIS-3)
|
15 (8.4)
|
16 (4.0)
|
p < 0.05
|
3.4
|
1.1–10.7
|
< 0.05
|
|
Abdominal lesion
|
|
|
|
|
|
|
|
|
|
Lesion of Abdomen (AIS-2)
|
11 (6.2)
|
7 (1.7)
|
p < 0.01
|
0.9
|
0.3–3.2
|
NS
|
|
Upper-limb lesion
|
|
|
|
|
|
|
|
|
|
Shoulder contusion (AIS-1)
|
3 (1.7)
|
33 (8.2)
|
p < 0.01
|
0.2
|
0.03–0.8
|
< 0.05
|
|
Upper-limb fracture (AIS-3)
|
20 (11.2)
|
21 (5.2)
|
p < 0.01
|
1.0
|
0.4–2.6
|
NS
|
|
Lower-limb lesion
|
|
|
|
|
|
|
|
|
|
Contusion of knee (AIS-1)
|
5 (2.8)
|
32 (8.0)
|
p < 0.05
|
0.4
|
0.1–2.2
|
NS
|
|
All lower-limb lesions (AIS-2)
|
57 (31.8)
|
50 (12.4)
|
p < 0.0001
|
4.0
|
1.6–9.9
|
< 0.01
|
|
All lower-limb lesions (AIS-3)
|
41 (22.9)
|
22 (5.5)
|
p < 0.0001
|
4.0
|
1.3–12.3
|
< 0.05
|
|
- Including femoral fracture (AIS-3)
|
25 (14.0)
|
8 (2.0)
|
p < 0.0001
|
3.8
|
1.1–14.0
|
< 0.05
|
|
- Other AIS-3 lower-limb lesions
|
39 (21.8)
|
18 (4.5)
|
p < 0.0001
|
4.7
|
1.9–11.7
|
< 0.001
|
|
Spine
|
|
|
|
|
|
|
|
|
|
Spinal fracture (AIS-2-3-4-5)
|
20 (11.2)
|
13 (3.2)
|
p < 0.001
|
3.3
|
0.9–11.4
|
NS
|
|
Other (AIS-2-3-4-5)
|
13 (7.3)
|
7 (1.7)
|
p < 0.001
|
2.2
|
0.4–12.6
|
NS
|
|
aOnly lesions significantly associated with return-to-work status on univariate analysis are shown.
bOther: not cranial or cranial base fracture, e.g. cerebral contusion, etc.
95% CI: 95% confidence interval; OR: odds ratio; AIS: Abbreviated Injury Scale; NS. non-significant.
|
Discussion
Various factors characterized late return to work; most concerned initial lesion type and severity: mild cranial trauma, severe lower-limb lesion, severe head lesion and severe thoracic lesion. Predictive factors identified from inclusion data were: type of journey, lesion severity, and intention to press charges. Predictive factors identified from inclusion plus 6-months data were: persistent physical or neuropsychological sequelae, persistent pain and pressing charges.
Interpretation
Gender and age criteria did not correlate significantly with late return to work, although there were more persons over the age of 45 years among late returners (23% vs 18%). Normal physical weakening with age, reduced adaptability and presence of comorbidity might play an essential role in this age distribution, notably in cases of cranial trauma (15, 16). In fact, medical history before the accident did not influence the time to return to work (23.5% for late return to work vs 22.9% for normal returners, p = 0.9).
A low educational level was reported to be associated with difficulty in returning to work for patients with medullary (17) or cerebral lesions (18). This may be due to physical demands of the job for such persons, limited ability to change posts, and difficulty in benefiting from occupational guidance. Although ESPARR cohort victims with a low educational level were more often late returners, this did not emerge as an explanatory factor in itself.
Accidents on the journey to or from work were more frequent among late returners; but, once adjusted for 6-month factors, the type of journey no longer features, being replaced by pain and sequelae. Several authors claim that indemnities paid in relation to work accidents have the effect of delaying return to work (6, 16, 17, 19, 20); it may also, however, be argued that work-related accidents are experienced as more traumatic, and this in turn may explain why, apart from the type of journey, the fact of pressing charges should be a predictive factor. Pressing charges is usually associated with difficulty in returning to work, and several authors consider it to be a negative factor in the process of returning to work (16, 20–22). Pressing charges, however, may be an indicator of suffering, which dysfunctional administrative, healthcare and insurance systems tend to aggravate, so that what MacEachen et al. (23) calls the “toxic dose” of system problems is reached. It may also be the case that pressing charges is associated with a self-perception as victim, with the charges being meant to compensate for an injustice, especially when the accident has resulted in pain and sequelae (24). In the present study, however, the victim’s non-responsibility in the accident did not associate significantly with return to work. Likewise, while PTSD was more frequent in late returners (as also reported elsewhere (15, 25)), it did not emerge as a predictive factor.
ISS scores equal to or greater than 9 and/or multiple trauma, on the other hand, were predictive of late return to work. In subjects sustaining severe injuries in an accident, severity is known to be a major predictor of non-return to work (26): Vles et al. (27) reported that an ISS score > 25 and a large number of lesion sites had a negative impact on return to work; and Shames et al (28), in a review of the literature on return to work after cranial trauma, found trauma severity to be of negative impact.
Two other factors appeared to be of particular importance, in agreement with other reports: sequelae (18) and persistent pain (26, 29). MacKenzie et al. (16), in a prospective study of lower-limb fracture, demonstrated that more intense pain was associated with lower levels of return to work.
Published data frequently implicates duration of hospital stay as a predictive factor of non-return to work (18, 26, 29, 30). Soberg et al. (31) reported a 20-week stay to be a threshold beyond which the rate of return to work falls off. According to Holbrook et al. (32), it is the duration of intensive care that counts. In the same type of population, Brenneman et al. (33) showed that patients who returned to work had spent 3 times less time in intensive care and had a 9-fold shorter overall hospital stay. The present study, however, adjusted duration of disability on overall lesion severity, whence it emerged that these duration factors were merely indicators of severity and not in themselves predictors of late return to work.
In the present cohort, the type of lesion most frequently associated with late return to work was mild cranial trauma, in agreement with other reports (29, 34). Lower-limb lesions are frequently associated with late return to work, too (35): the AIS score may perhaps underestimate their longer-term severity, associated with longer sick leave; our choice of the median value rather than the upper quartile for this level of severity may be a reflection of this observation.
Spinal lesions are often mentioned as entailing an elevated risk of difficulty in returning to work (36, 37), and were more frequent in the late-return group; lack of statistical power, however, precluded demonstration of a significant relation. Unlike other authors (38, 39), however, we did not find significantly more cases of whiplash in the late-return group, in agreement with Gun et al. (40).
Strengths and limitations
The 184 subjects lost to follow-up showed significant differences from respondents: they were younger, with a lower educational level and milder injuries. Late return to work in adults of the cohort may thus be biased; age, however, would not appear to be relevant. Due to the definition of the threshold based on the sick leave duration in function of the severity, the milder lesions of non-respondents would not change the estimation of the prevalence of a late return to work except if the lower educational level is related both to the severity and to the duration of sick leave. Moreover, the response rate was satisfactory (76.8%), so that loss to follow-up is unlikely to have affected identification of predictive factors, especially inasmuch as the multivariate model allows age and severity to be mutually adjusted.
The analysis also used weighting according to survey fraction to take account of the difference in cohort survey fraction between subjects with M-AIS < 3 and M-AIS ≥ 3.
A novel feature of the study is the definition of “normal” or “late” return to work based on the duration of sick leave adjusted on each M-AIS severity score. The choice of 4 thresholds determined by the upper quartile of time to return to work for each M-AIS level (or rather, by the median in the case of M-AIS3) is open to criticism, but was validated by two different sources: a survey of 30 physicians, and the French national health insurance (Sécurité Sociale) used in following up work-accident victims (14). It is, however, possible that subjects were inexact in specifying the date of their return to work, leading to some misclassification.
AIS score is known to reflect the immediate severity. This immediate severity does not predict the disability at discharge or at 6-months post-injury (41), but could reflect the length of normal healing after a lesion. However, AIS score was only used to stratify population study and to choose threshold of sick leave duration, because each lesion is clearly individualized in the AIS score. Our results show that both the immediate severity and the disability at one year are linked with a late return to work.
Finally, it is evident that having only one lesion is quite different to having several lesions: this could explain why some of our subjects with M-AIS = 3 have long sick leave, possibly due to several lesions to the lower limbs, which complicate the return to work. This is why we used the ISS in the analysis, which measures the seriousness of multiple traumatic injuries; it was not significantly associated with the return to work in multivariate analysis. Disability at discharge and at 6 months post-injury was not studied, but specific lesions were analysed independently in a multivariate analysis. We did not use this score to define our thresholds of sick leave, due to the difficulties of individualizing the numerous possibilities of combinations of 1–3 lesions per subject.
Not taking into account some occupational factors, such as job demand or social support in the workplace, might introduce a limitation in our study.
In conclusion, return to work after an accident is a complex process: many factors influence the duration of sick leave. Severe lesions of the lower limbs are particularly related to late return to work. Pressing charges, persistent pain at 6 months and physical sequelae of the initial lesions emerged as predictive of late return to work in the present road accident victim population.
ACKNOWLEDGEMENTS
The authors would like to thank all those who helped them perform this study: Nadia Baguena, Jean Yves Bar, Amélie Boulanger, Elodie Paquelet, Stuart Nash, Véronique Sotton for collecting the data, Irène Vergnes for creating the databases, Anne-Marie Bigot, Nathalie Demangel, Geneviève Boissier for managing the subject database, Valérie Bonnavion for her help in analysing the literature, Amina Ndiaye, Blandine Gadegbeku and the Rhône Département Road Trauma Register Association (ARVAC) for its help in collecting medical data and for placing the Registry database at our disposal, the Scientific Committee (Daniel Floret, François Chapuis, Jean Michel Mazaux, Jean Louis Martin), all the hospital staff who accepted the interviewers’ presence and brought the patients to their attention, and, lastly, the 'Service d'Aide Médicale Urgente' (SAMU) team who reported their emergency calls on a daily basis. Many thanks to Iain McGill for reviewing the English language in this paper.
The study was approved by French committees of ethics and medical information (CCTI Number 04.159 and CNIL Number 04-1417).
Funding sources:We acknowledge funding from the French Ministry of Equipment, Transport, Housing, Tourism and Sea (Predit 3 Program “New Knowledge in the Field of Road Safety”: Number SU0400066) and from the French Ministry of Health (Program PHRC2003: PHRC-N03; and PHRC2005: PHRC-N051).
The individual authors have no competing interests to declare.
References