OBJECTIVE: To investigate the magnitude of change at different time points in measures of gait symmetry, gait velocity and self-reported function following total hip replacement.
DESIGN: Longitudinal with test occasions pre-surgery and 3, 6 and 12 months post-surgery.
SUBJECTS: Thirty-four patients with hip osteoarthritis (mean age 63 years, standard deviation 11 years).
METHODS: Subjects walked back and forth along a 7-m walkway at slow, preferred and fast speed. Anteroposterior, vertical and mediolateral trunk symmetry was assessed by accelerometry, while single support symmetry, step-length symmetry and gait velocity was simultaneously assessed by an electronic walkway. Self-reported function was assessed by Hip disability and Osteoarthritis Outcome Score. Gait symmetry data were normalized for gait velocity. Changes between test occasions were reported as effect size.
RESULTS: All measures showed effect sizes > 0.30 from preoperative to 12-months postoperative assessments, and improvements were significant (p < 0.05) in all measures, except mediolateral symmetry. In general, gait symmetry and gait velocity improved most 6 and 12 months postoperatively, while self-reported function improved most 3 months postoperatively.
CONCLUSION: Early improvements were seen in self-reported function, suggesting immediate relief from stiffness and pain, while gait symmetry and velocity improved later postoperatively, suggesting that gait quality and performance require prolonged rehabilitation with postoperative guidance, muscular strengthening and motor relearning.
Key words: gait analysis; hip arthroplasty; clinical course; recovery; outcome measures; effect size.
J Rehabil Med 2011; 00: 00–00
Correspondence address: Caroline Hodt-Billington, Section of Physiotherapy Science, Department of Public Health and Primary Health Care, Faculty of Medicine and Dentistry, University of Bergen, PO Box 7804, NO-5020 Bergen, Norway. E-mail: caroline.hodt@isf.uib.no
Submitted September 3, 2010; accepted May 31, 2011
INTRODUCTION
Gait symmetry is often a goal for physiotherapy in patients after total hip replacement (THR), and has been advocated when evaluating gait quality after disease or injury affecting the lower limbs, such as stroke and hip osteoarthritis (1, 2). However, gait symmetry is not routinely assessed as a clinical outcome following THR. Evaluation should include temporal and spatial footfall movement as well as measures of trunk movement (1), because compensatory movements of the upper body are frequently seen in patients with injury or disease in the hip (3, 4). At present, gait velocity and self-reported function are typically reported as clinical outcomes after THR (5–7). These measures are easily administrated. Gait velocity is considered a fundamental measure of gait (3), while self-reported function has been advocated as a supplement to other information on clinical outcome (8). In contrast to measures of gait symmetry, gait velocity and self-reported function do not provide information that relate easily to specific movement strategies, which may in turn provide valuable information for the development of individually targeted rehabilitation programmes. Most longitudinal studies on change in function following THR assess function only once before and after surgery. Thus, information regarding the magnitude of change in function at different points in time is not known. Better knowledge about functional change following surgery may lead to better targeted rehabilitation programmes. The purpose of this study was to investigate the magnitude of change of gait symmetry, gait velocity and self-reported function at different time-points during the first 12 months after THR.
MATERIAL AND METHODS
Subjects
A total of 41 patients with primary hip osteoarthritis scheduled for hip replacement surgery were recruited from two university hospitals. To reflect the population in need of THR, chosen inclusion criteria comprised both genders at a wide range of ages (Table I), 3 categories of hip involvement (Table II), different implants and 2 postoperative weight-bearing regimes (Table II). However, all patients were without other musculoskeletal ailments likely to influence walking ability and were able to walk at least 10 m without assistive devices at all test occasions. For inclusion in the final analysis, subjects had to comply with postoperative instructions from the 2 operating hospitals and attend at least 3 test occasions. In order to compare outcome measures at a common gait velocity of 0.9 m/s, included patients had to have this speed within the range of self-selected gait velocities at every test occasion. Thirty-four patients with a mean age of 63 years, standard deviation (SD) 11 years (Table I) were included in the final analyses, after the exclusion of 1 patient due to postponed THR surgery, 2 due to postoperative complications, 2 because they missed 2 test occasions, and 2 because they walked too slowly 3 months postoperatively. All subjects received postoperative physical therapy during the hospital stay, and were encouraged to avoid the extremes of hip rotation, flexion and adduction. The Regional Committee for Medical Research Ethics approved the study, and all participants provided informed consent.
Measurements
Single support (% of stride time), step length (m), and gait velocity (m/s) were registered by an electronic walkway (GAITRite Gold, CIR Systems Inc., NJ, USA). The GAITRite® has previously showed good to excellent test–retest reliability of temporal–spatial gait parameters (9–12), and is regarded as a valid tool for assessment of those parameters (9, 10). Trunk acceleration in anteroposterior (AP), vertical (V) and mediolateral (ML) directions was simultaneously registered by a 0.015 kg triaxial, piezoresistant accelerometer (Logger technology HB, Malmö, Sweden), which provides reliable and valid measures of movement during gait (13, 14). A computerized stopwatch was synchronized to the accelerometer and registered time sequences for each walk through photoelectric cells. The accelerometer was secured to the subject’s back, approximately at the L3-level of the spine, by a customized belt, and connected to a 0.3 kg battery-operated Personal Computer Memory Card International Association card data-logger (Logger Technology HB, Malmö, Sweden), also worn by the subjects.
The Hip disability and Osteoarthritis Outcome Score questionnaire (HOOS), Likert version (LK) 1.1, was used to assess self-reported symptoms and functional limitations. HOOS is disease specific and was developed to evaluate self-reported problems of patients with hip osteoarthritis (15, 16). HOOS has adequate measurement properties of validity and reliability (17), and has been recommended for use in the evaluation of patients with hip osteoarthritis before and after total hip replacement (16). The questionnaire is scored according to the “HOOS LK 1.1 User’s Guide 2003” (18) with 39 items in 5 sub-scales:
• P = Pain;
• S = Other symptoms, including stiffness;
• ADL = Function in daily living;
• QOL = Hip-related quality of life;
• SP = Function in sport and recreation.
Data from the SP subscale was not registered at postoperative tests due to postoperative movement restrictions. In each subscale, no symptoms equal a score of 0, while 100 indicates extreme symptoms, according to the HOOS LK 1.1 User’s Guide 2003 (18).
Procedure
To become accustomed to the equipment and avoid practice effect, subjects walked across the walkway twice before data collection started. Each subject then walked 6 times along the 7-m walkway: 2 walks at self-selected slow speed, 2 walks at self-selected preferred speed, and 2 walks at self-selected maximum safe speed. Footfall and trunk symmetry measures were assessed during the middle 4.3 m of the walkway, leaving the rest of the walkway for acceleration and deceleration. The subjects wore their own shoes and performed the tests without any personal assistance or walking aids. Questionnaires were posted to each subject less than 1 week before test occasions and returned when subjects presented for testing.
Data analysis
The electronic walkway’s software (GAITRite3A) and Microsoft Excel (97-2003) were used in the calculations of footfall measures and gait velocity. Analogue signals from the accelerometer were low-pass filtered at 55 Hz and sampled at 128 Hz before digital signals were transferred to a laptop for off-line processing in Matlab 7.1 (The Mathworks Inc., Natick, MA, USA). Acceleration signals were transformed to a true horizontal–vertical coordinate system, keeping the AP axis in the sagittal plane to eliminate unwanted gravity components caused by inaccurate orientation of the sensor (19).
Between-step and between-stride trunk regularity were assessed by an autocorrelation procedure where a cyclic acceleration curve representing a walk was correlated to the same curve at a phase shift of one step and one stride, respectively. In the mathematical procedure proposed by Moe-Nilssen & Helbostad (20) and adopted by Tura et al. (21), the generic unbiased autocorrelation function, Ad(m), of the sample sequence x(i) is computed using:
| Ad(m) = | 1 | ∑ | N–│m│ | x(i) · x(i+m) |
| N–│m│ | i = 1 |
where, N is the number of samples and m is the time lag expressed as number of samples. The first peak of Ad(m) represents between-step regularity, while the second peak of Ad(m) represents between-stride regularity. Regularity values approaching 1.0 imply highly repetitive gait or high gait regularity, while values approaching 0.0 imply low gait regularity.
Scores were imputed for patients who missed one gait assessment. Changes in group mean values were calculated and added to the previous score of the patient with missing data. While the total number of score was 156 (4 test occasions times 34 patients) for each outcome measure, 8 of these scores were missing and thus imputed for each of SL and SS symmetry. For trunk symmetry and gait velocity measures, the number of imputed scores was 6 for each measure.
Missing data within each subscale of the HOOS questionnaire were replaced by the mean value for the subscale in question, as reported in previous studies (15). If more than 2 items were missing, the subscale in question was deleted from the analysis. To evaluate the inclusion of missing values, Friedman’s analysis of variance (ANOVA) was performed with and without the imputed values.
All gait symmetry measures were checked for speed dependency using data from the 6 walks performed by each subject preoperatively. The gradients (b1) of individual linear trend lines of a symmetry measure vs walking speed were tested by one-sample t-tests for H0: b1= 0. The tests returned significant linear relationships for most symmetry measures. Thus, controlling symmetry measures for gait velocity was warranted. Data from the 6 walks were used to make linear curve estimates for each subject, and data at a point estimate of 0.9 m/s were used in the analysis. This speed was within the range of gait velocities for included subjects at all test occasions, except for 1 patient whose fastest velocity 3 months postoperatively was 0.84 m/s. To avoid overall exclusion of this patient, linear curve estimates of symmetry data in relation to speed were extrapolated to 0.9 m/s at this particular occasion, before symmetry data were estimated.
Symmetry indices (SI) were calculated for each trunk and footfall measure. Step length and single support symmetry ratio were used to describe footfall symmetry:
SIfootfall = 1 – (limb with lower value/limb with higher value)
Trunk measures are previously used to describe gait symmetry (1, 20, 21), and symmetry indices were calculated separately for AP, V and ML signals:
SItrunk=between-stride regularity – │between-step regularity│
Absolute values of between-step trunk regularity are used because the software displays ML between-step trunk regularity with negative values. Ratio calculations of trunk measures are unsuitable because the between-step and between-stride autocorrelations may approach zero if regularity between neighbouring steps or neighbouring strides is low. The number zero cannot be used as the denominator. Hence, the symmetry indices of footfall and trunk measures are based on different calculations. However, at perfect symmetry, both indices equal 0, and positive indices indicate asymmetric gait.
Statistical analysis
Anthropometric data are presented as mean and SDs, while paired sample t-tests were used to evaluate change in these data from preoperative to 12 months postoperative assessments (Table I). The outcome measures, gait symmetry, gait velocity and self-reported function, are presented as median with 25th and 75th percentiles. Wilcoxon rank-sum test was used to assess possible differences in outcome measures related to differences in gender, postoperative weight-bearing restrictions or operating hospital. The Kruskal-Wallis test, followed by Wilcoxon rank-sum test when appropriate, was used to assess differences in outcome measures related to hip involvement. Change from preoperative to 12 months postoperative assessment was evaluated with the Friedman’s ANOVA, while the Wilcoxon signed-rank was used to assess changes between neighbouring assessments. To correct for the number of tests in the Wilcoxon signed-rank analysis, the Bonferroni corrections (α/number of comparisons) was used to decide a critical values (22, p. 577). Effect size (ES) was used to quantify functional change, as it is suited to compare the magnitude of change in measures using different scales and units of measurements (23, 24). Reports were made between neighbouring test occasions, and between preoperative and 12 months postoperative tests. The Rosenthal (25) formula, also adopted by Field (22, p. 550); ES = , lets Z equal the value of the observation expressed in SD units, while N is the number of total observations on which Z is based (22, p. 580). Small, medium and large magnitude of change equal ES values above respectively 0.1, 0.3 or 0.5, as suggested by Cohen (26), who further suggests that medium effect is comparable to improvement visible to the eye (26). The level of significance was set at p < 0.05. Statistical analyses were performed in Microsoft Excel and Statistical Package for Social Sciences (SPSS) Version 18.
| z |
| √N |
| Table I. Descriptive characteristics of the patients preoperatively (pre) and 3, 6, and 12 months postoperatively (post 3, 6, and 12) | ||||
| Pre (n = 34) Mean (SD) | Post 3 (n = 34) Mean (SD) | Post 6 (n = 31a) Mean (SD) | Post 12 (n = 31a) Mean (SD) | |
| Age, total sample, years | 63 (10.8) | |||
| Age, men, years (n = 14) | 60 (12.6) | |||
| Age, women, years (n = 20) | 65 (9.3) | |||
| Height, m | 1.74 (0.09) | 1.74 (0.09) | 1.74 (0.09) | 1.74 (0.09) |
| Weight, kg | 83.3* (16.4) | 83.4 (15.7) | 83.9 (15.9) | 86.3 (14.6) |
| BMIb, kg/m2 | 27.6* (4.9) | 27.5 (4.7) | 27.8 (4.7) | 28.5 (4.5) |
| Step countc | 40 (9) | 38 (7) | 35 (5) | 33 (6) |
| aMissing data not imputed for descriptive characteristics. bIndoor clothing, shoes and equipment (body fixed sensor and data logger) included in the measures of height and weight. cThe total number of steps used to calculate outcome measures at each test occasion. *Significant difference between preoperative and 12 months postoperative assessments (p = 0.05). BMI: body mass index; SD: standard deviation. | ||||
RESULTS
Patients increased their body weight significantly from preoperative to 12 months postoperative assessments (Table I). The mean number of steps used to evaluate gait symmetry was from 33 (SD 6) to 40 (SD 9) per test occasion (Table I). In general, men walked significantly faster than women at fast and preferred gait velocities throughout test occasions (p = 0.001 – p = 0.042), except for preferred gait velocity preoperatively, where the difference was insignificant (p = 0.10). Patients from one hospital showed higher gait symmetry, lower gait velocity and self-reported function. These differences were insignificant at most test occasions, except in 3 HOOS subscales preoperatively; symptoms (p = 0.035), ADL (p < 0.001) and QOL (p = 0.046), AP symmetry 3 and 12 months postoperatively (p = 0.04 – p = 0.03) and ML symmetry 6 months postoperatively (p = 0.02). Most outcome measures were unaffected by differences in postoperative weight-bearing restrictions, except for HQOL preoperatively (p = 0.045), V symmetry 3 months postoperatively (p = 0.007) and ADL 12 months postoperatively (p = 0.048). No differences in outcome measures were related to diagnostic group, except ADL 3 and 6 months postoperatively, where patients with one-sided affection demonstrated better self-reported function than patients with respectively bilateral 1st hip to be operated (p = 0.008) and bilateral 2nd hip to be operated (p = 0.011). All outcome measures, except ML symmetry, showed significant improvement from preoperative to 12 months postoperative assessments (Table III).
| Table II. Diagnostic, operational and postoperative weigth-bearing descriptive characteristic among the patients | |||
| aPWB (n = 15) n (%) | bWBAT (n = 19) n (%) | Total (n = 34) n (%) | |
| Operated hip | |||
| Left hip | 6 (18) | 9 (26) | 15 (44) |
| Right hip | 9 (26) | 10 (29) | 19 (56) |
| Total | 15 (44) | 19 (56) | 34 (100) |
| Diagnostic group (radiographic images) | |||
| 1-sided osteoarthritis | 5 (15) | 11 (32) | 16 (47) |
| 2-sided osteoarthritis 1st hip to be operated | 4 (12) | 5 (15) | 9 (26) |
| 2-sided osteoarthritis 2nd hip to be operated | 6 (18) | 3 (9) | 9 (26) |
| Total | 15 (44) | 19 (56) | 34 (100) |
| Prosthesis; acetabulum/ femur components | |||
| cCharnley Ogee cement/Charnley cement | 2 (6) | 12 (35) | 14 (41) |
| cReflection cement/Spectron cement | 5 (15) | 3 (9) | 8 (24) |
| dReflection/Landos Corail cement less | 5 (15) | 5 (15) | |
| cOther brands | 3 (9) | 1 (3) | 4 (12) |
| eBirmingham hip resurfacing | 3 (9) | 3 (9) | |
| Total | 15 (44) | 19 (56) | 34 (100) |
| aPWB: partial weight-bearing. Patients were instructed to allow a maximum load of 20–30 kg on the operated leg and to use crutches 3 months post-operatively. Patients operated with direct lateral approach were additionally instructed to avoid active hip abduction exercises 6 weeks post-operatively. bWBAT: weight-bearing as tolerated, limited by pain. Patients were instructed to use crutches 6 weeks post-operatively. cDirect lateral approach. dDirect lateral approach in 3 patients and dorsal approach in 1 patient. eDorsal approach. | |||
| Table III. Friedman’s analysis of variance (ANOVA) (χ2) statistics of main effect with level of significance (p-value), post-hoc tests (Wilcoxon signed-rank tests) with a Bonferroni correction of level of significance p < 0.0167 (0.05/3) are applied and supplemented with effect sizes (ES) to evaluate change between neighbouring assessments | ||||||||||
| Main effecta p-value | Pre-post 12 | Pre-post 3 | Post 3–6 | Post 6–12 | ||||||
| p-value | ESb | p-value | ESb | p-value | ESb | p-value | ESb | |||
| Symmetry indices | ||||||||||
| AP | < 0.001 | < 0.001 | –0.43 | 0.125 | –0.19 | < 0.001 | –0.41 | 0.191 | –0.16 | |
| V | < 0.001 | < 0.001 | –0.52 | 0.013 | –0.30 | 0.043 | –0.25 | 0.064 | –0.22 | |
| ML | 0.20 | 0.11 | –0.20 | 0.774 | –0.04 | 0.661 | –0.05 | 0.011 | –0.31 | |
| SL | 0.011 | 0.006 | –0.33 | 0.030 | –0.26 | 0.554 | –0.07 | 0.015 | –0.29 | |
| SS | 0.002 | < 0.001 | –0.41 | 0.543 | –0.08 | 0.012 | –0.30 | 0.778 | –0.04 | |
| Velocity, m/s | ||||||||||
| Fast | < 0.001 | < 0.001 | –0.51 | 0.791 | –0.03 | < 0.001 | –0.42 | 0.388 | –0.11 | |
| Pref | < 0.001 | < 0.001 | –0.54 | 0.598 | –0.07 | 0.001 | –0.40 | 0.001 | –0.38 | |
| Slow | < 0.001 | < 0.001 | –0.42 | 0.713 | –0.05 | 0.073 | –0.22 | < 0.001 | –0.45 | |
| HOOS | ||||||||||
| Pc | < 0.001 | < 0.001 | –0.62 | < 0.001 | –0.61 | 0.319 | –0.12 | 0.002 | –0.35 | |
| S | < 0.001 | < 0.001 | –0.62 | < 0.001 | –0.58 | 0.016 | –0.29 | < 0.001 | –0.40 | |
| ADL | < 0.001 | < 0.001 | –0.61 | < 0.001 | –0.59 | < 0.001 | –0.47 | 0.002 | –0.36 | |
| QOL | < 0.001 | < 0.001 | –0.62 | < 0.001 | –0.59 | < 0.001 | –0.45 | 0.34 | –0.12 | |
| aMain effect based upon χ2 test (degrees of freedom = 3); bES based upon Z-values; cn = 33; AP: anteroposterior; V: vertical; ML: mediolateral; SL: step length; SS: single support; Gait velocities: Fast, Preferred (pref) and Slow; HOOS: Hip disability and Osteoarthritis Outcome Score questionnaire; P: pain; S: other symptoms, including stiffness; ADL: function in daily living; QOL: hip-related quality of live; SP: function in sport and recreation. ES values above 0.1, 0.3 or 0.5 represent small, medium and large effects. | ||||||||||
The magnitude of change between preoperative and 12 months postoperative assessments in symmetry measures that showed significant improvement ranged from ES 0.33 to 0.52 (Table III). Comparing neighbouring test occasions, the largest improvement in AP and SS gait symmetry was seen from 3 to 6 months postoperatively, in SL and ML symmetry from 6 to 12 months postoperatively, while V showed the highest improvement between preoperative and 3 months postoperative assessments; however, continuous improvement (ES > 0.22) throughout test occasions.
In measures of gait velocity, the ES magnitude of change from preoperative to 12 months postoperatively ranged from 0.42 to 0.54. Median gait velocity decreased insignificantly from preoperative to 3 months postoperatively, while the increase in gait velocity was largest from 3 to 6 months postoperatively (Tables III and IV).
| Table IV. Median values with 25th and 75th percentiles (percentiles) of symmetry indices, gait velocities and HOOS subcategories (n = 34) preoperatively (pre) and 3, 6 and 12 months postoperatively (post 3, 6 and 12) | |||||
| Measure | Pre | Post 3 | Post 6 | Post 12 | |
| Median (percentiles) | Median (percentiles) | Median (percentiles) | Median (percentiles) | ||
| Symmetry indices | |||||
| AP | 0.26 (0.10, 0.51) | 0.15 (0.06, 0.47) | 0.09 (0.06, 0.18) | 0.09 (0.04, 0.14) | |
| V | 0.15 (0.05, 0.28) | 0.06 (0.02, 0.18) | 0.04 (0.01, 0.12) | 0.03 (0.00, 0.09) | |
| ML | 0.13 (0.06, 0.28) | 0.14 (0.05, 0.23) | 0.12 (0.08, 0.19) | 0.08 (0.03, 0.18) | |
| SL | 0.05 (0.03, 0.09) | 0.04 (0.02, 0.07) | 0.04 (0.03, 0.09) | 0.04 (0.01, 0.06) | |
| SS | 0.08 (0.04, 0.13) | 0.05 (0.03, 0.12) | 0.04 (0.02, 0.07) | 0.04 (0.01, 0.07) | |
| Velocity (m/s) | |||||
| Fast | 1.50 (1.26, 1.83) | 1.48 (1.28, 1.86) | 1.57 (1.38, 1.96) | 1.74 (1.42, 1.98) | |
| Pref | 0.97 (0.87, 1.13) | 0.96 (0.87, 1.11) | 1.08 (0.95, 1.21) | 1.18 (1.05, 1.30) | |
| Slow | 0.49 (0.45, 0.59) | 0.49 (0.43, 0.58) | 0.54 (0.45, 0.68) | 0.68 (0.62, 0.79) | |
| HOOS | |||||
| Pa | 61.1 (52.8, 66.7) | 13.9 (2.8, 27.8) | 13.9 (5.6, 25.0) | 5.6 (0, 19) | |
| S | 57.5 (43.8, 70.0) | 25 (15, 35) | 20 (10, 31.3) | 15 (5, 20) | |
| ADL | 58.8 (48.9, 63.2) | 29.4 (22.8, 35.3) | 16.2 (8.1, 32.4) | 10.3 (2.9, 21.3) | |
| QOL | 75 (67.2, 82.8) | 50 (43.8, 62.5) | 37.5 (25, 51.6) | 37.5 (25, 50) | |
| SPb | 75 (68.8, 87.5) | ||||
| an = 33; bSP only reported preoperatively, due to postoperative movement restrictions. Gait velocities: Fast, Preferred (pref) and Slow; AP: anteroposterior; V: vertical; ML: mediolateral; SL: step length; SS: single support; HOOS: Hip disability and Osteoarthritis Outcome Score questionnaire; P = Pain, S = Other symptoms, including stiffness; ADL: function in daily living; QOL: hip-related quality of life; SP: function in sport and recreation. | |||||
The magnitude of change from preoperative to 12 months postoperative test occasions in self-reported function ranged from ES 0.61 to 0.62. The largest improvement in self-reported function was seen from preoperative to 3 months postoperatively (Tables III and IV), although improvement was high for most categories throughout test occasions.
DISCUSSION
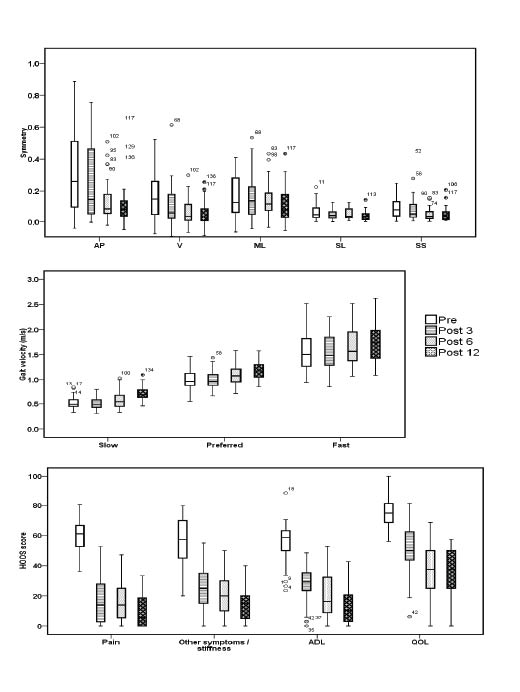
The purpose of this study was to investigate the magnitude of change in measures of gait symmetry, gait velocity and self-reported function preoperatively, and 3, 6 and 12 months postoperative to THR. A repeated measures design was chosen to allow identification of periods with larger and smaller magnitudes of clinical change. Overall, all measures showed postoperative improvement in function, but the period of largest change differed between measures. While gait symmetry and gait velocity measures in general showed the largest postoperative improvement towards 6 and 12 months postoperatively (Fig. 1a, 1b), self-reported function showed the largest improvement towards 3 months postoperatively. However, improvement in self-reported function was large for all test occasions (Fig. 1c).
Fig. 1. (a–c) Median with 25th and 75th percentiles for outcome measures assessed preoperatively (pre), and 3, 6 and 12 months (post, 3, 6, 12) after total hip replacement surgery. (a) Anteroposterior (AP), vertical (V), mediolateral (ML) trunk symmetry indices, step length (SL) and single support (SS) symmetry indices (0 = perfect symmetry). (b) Fast, preferred and slow gait velocity. (c) Hip disability and Osteoarthritis Outcome Score questionnaire (HOOS) with subscales: Pain, Other symptoms, including stiffness, Function in daily living (ADL), and hip-related quality of life (QOL) (0–100 = best to worse score).
The largest improvement in most symmetry measures was observed at test occasions 6 and 12 months postoperatively. The same time-lagged postoperative improvement in gait symmetry has also been reported previously (27, 28), and may be explained by early postoperative weight-bearing restrictions, time needed to recover from surgery and the need for muscular strengthening and motor relearning to achieve symmetrical gait. Change in ML symmetry differed somewhat compared with the other symmetry measures, and improvement was scarce at assessments 3 and 6 months postoperatively. However, 12 months postoperatively, ML symmetry showed largest improvement among symmetry measures, suggesting that ML symmetry describes different qualities of gait compared with other symmetry measures. Unilateral muscular weakness of the hip abductors has been reported in patients with osteoarthritis (27, 29) and has also been found to persist 2 years after THR (27). The weakness may lead to the so-called Trendelenburg gait, where a failure to stabilize the pelvis during stance may result in lateral deviation of the trunk, hence ML trunk asymmetry.
The pattern of change in gait velocity differed somewhat compared with the observed change in gait symmetry and self-reported function (Fig. 1c), as patients tended to walk slightly slower after 3 months than they did preoperatively. Thereafter, gait velocity increased at 6 and 12 months postoperative assessments. The delayed increase in gait velocity may be explained by consciousness and awareness surrounding the effort to achieve symmetrical gait, but also by postoperative insecurity in general. van den Akker-Scheek et al. (30) let the patients use walking aids at postoperative gait assessment and found increased gait velocity as soon as 6 weeks postoperatively. However, in agreement with our findings, the largest improvement in gait velocity was seen 6 months postoperatively. Self-reported function showed the largest overall magnitude of change and ES above 0.58 as soon as 3 months postoperatively and above 0.61 after 12 months. This large and early improvement may be explained by the patients’ experience of immediate relief from stiffness and pain, which is also previously reported after THR (31).
The achievement of gait symmetry may be a prerequisite to avoid later disease or injury caused by misalignment. Time-consuming clinically guided exercises, along with muscular strengthening and relearning, may be necessary to achieve gait symmetry, and naturally lead to improvement later postoperatively compared with improvement in self-reported function. Our findings support previous findings that highlight the importance of including objective measures in postoperative evaluation and rehabilitation strategies (8). Self-reported measures alone, or a failure to also include objective measures with unique properties, such as properties suggested for measures of ML symmetry in this study, may conceal important functional qualities of gait and may also delay rehabilitation after THR.
The low number of steps per walk may represent a limitation, but is clinically relevant because of limited space available at typical test locations. However, data were collected from 6 walks, with a mean of at least 33 steps at any of the 4 test occasions (Table I). A number of symmetry indices with known limitations have been used previously to quantify gait symmetry (32). The two indices used in this study were chosen because they relate easily to performance of limbs or movement qualities, and ratio indices are previously advocated for similar reasons (33). ES are not calculated from main effect, but rather for the preoperative test compared with 12 months postoperatively, in addition to neighbouring test occasions, due to the limited possibility to calculate ES based on χ2 statistic with more than 1 degree of freedom (22).
Although our results suggest continuous improvement throughout the first year following THR in all reported measures, ML symmetry seems to improve later than the other measures evaluated in this study. Longer follow-up periods or exercise programmes aimed to strengthen and stabilize the trunk and pelvis, and the hip abductors in particular, may reveal to what degree the observed change in ML symmetry reflects a time-lagged recovery compared with the other measures. Future studies should implement disease-specific exercise programmes before and after THR, and evaluate change over time measured by different objective and self-reported clinical outcome measures. Gait symmetry is suggested as a preferred measure of gait quality. However, the variation in time and magnitude of postoperative change found in this study supports the additional inclusion of gait velocity and self-reported function to provide a complete postoperative evaluation after THR.
In conclusion, the results of this study showed improvement in gait symmetry, gait velocity and self-reported function 1 year after THR. Only change in ML symmetry was not significant. The magnitude and time of improvement differed among clinical outcome measures. Large and early improvement was seen in self-reported function, suggesting immediate relief from stiffness and pain post-surgery. Gait symmetry and gait velocity showed later improvements, suggesting that these functions may require prolonged rehabilitation, with muscular strengthening and motor relearning, possibly with postoperative guidance. A test-battery including assessment of gait symmetry, gait velocity and self-reported function is suggested in postoperative evaluation of THR.
ACKNOWLEDGEMENTS
The study was funded by The Norwegian Fund for Post-Graduate Training in Physiotherapy. We thank the patients who participated in the study and the staff at Oslo University Hospital, Ullevaal and Bergen University Hospital, Kysthospitalet in Hagevik for their help in the recruitment of patients.
REFERENCES

