OBJECTIVE: The aim of this study was to explore in vivo the effects of botulinum toxin-A treatment on the muscle architecture of patients with stroke, using musculoskeletal ultrasonography.
METHODS: This prospective clinical trial included 26 adult stroke sufferers with a mean age of 55 years (standard deviation 14). Pennation angles between the fascicle path and the deep aponeurosis of the muscle, fascicle length, muscle thickness and muscle compressibility were scanned at the bulkiest part of the medial gastrocnemius on both limbs. Sonographic evaluations were performed initially before botulinum toxin-A injection and repeated on day 10 and after 2 months.
RESULTS: On the hemiplegic sides, anterior pennation angle and muscle thickness decreased (p = 0.014, p = 0.010, respectively), fascicle length increased (p = 0.025) and muscle compressibility did not change after 2 months of treatment compared with the baseline values.
CONCLUSION: The results confirm that muscle structure changes due to botulinum toxin-A. Long-term effects of botulinum toxin-A, timing for disappearance of the toxin effects, or evaluations for repeat injections, remain to be studied. The use of musculoskeletal ultrasonography appears to be promising in this regard.
Key words: botulinum toxin-A; muscle architecture, stroke; ultrasonography.
J Rehabil Med 2011; 00: 00–00
Correspondence address: Fatih Tok, İskenderun Military Hospital, Physical Medicine and Rehabilitation Service, Hatay, Turkey. E-mail: drfatihtok@gmail.com
Submitted April 15, 2011; accepted July 22, 2011
*This study has been accepted for oral presentation in ISPRM2011.
INTRODUCTION
With the use of musculoskeletal ultrasonography (MSUS), morphological changes in the architecture of paretic muscles have been reported in patients with stroke (1, 2). However, there is no information on whether those changes are further altered with botulinum toxin-A (BoNT-A) injection, which is a widely used treatment for focal spasticity in this group of patients (3). Previous studies have mainly investigated the effects of BoNT-A on clinical and functional outcome (4–9).
The aim of the present study was to explore in vivo the effects of BoNT-A treatment on the muscle architecture of patients with stroke. Given its myriad advantages (non-invasive, inexpensive, repeatable, does not contain ionizing radiation, provides dynamic imaging and comparison), we reasoned that MSUS can be a prompt method for measuring anterior pennation angle, fascicle length, thickness and compressibility of the gastrocnemius muscle. To the best of our knowledge, this study is the first to show the effects of BoNT-A on muscle architecture.
MATERIAL AND METHODS
Participants
Twenty-six consecutive adult stroke patients (14 male, 12 female) with a mean age of 55 years (standard deviation (SD) 14.04) were recruited. Inclusion criteria were: presence of hemiparesis and clinically detectable spasticity in the gastrocnemius muscle (with a score > 1+ according to Modified Ashworth Scale; MAS); and the absence of previous surgery on the lower limbs and injection (BoNT-A, phenol or alcohol) to the gastrocnemius muscle within the last year. All participants were informed about the study procedure and gave informed consent. The study protocol was approved by the Institutional Review Board.
Protocol
Data regarding age, height, weight, date of stroke onset, aetiology of stroke, dominant hemisphere, affected arterial territory, MAS scores, Brunnstrom stage of lower limb and leg circumference were noted.
Ultrasonographic evaluations of the medial head of the gastrocnemius muscle were performed bilaterally with a linear probe (7.5 MHz, Aloka Prosound 5000, Japan) while subjects were in a supine position on the examination table. Hip joints were kept in external rotation, knee joints in extension and ankle joints in a resting position. Pennation angles between the fascicle path and the deep aponeurosis of the muscle, fascicle length and muscle thickness were scanned at the most bulky part of the medial gastrocnemius (Fig. 1). These parameters were measured with minimum compression (in order to obtain a whole screen image rapidly with no shadowing). Thereafter, muscle thicknesses were also determined with maximum compression (Fig. 2) in order to calculate muscle compressibility (%) using the following formula:
where α = muscle thickness with minimum compression (mm); ß = muscle thickness with maximum compression (mm).
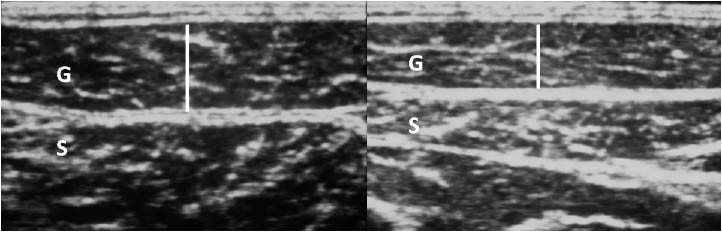
Fig. 1. Ultrasonographic imaging (longitudinal view) of the medial head of the gastrocnemius muscle in (A) a normal and (B) a hemiplegic subject demonstrating the pennate structure of the muscle. The curved arrows correspond to the pennate angle and the white lines correspond to single fascicles. G: gastrocnemius muscle, S: soleus muscle.
Fig. 2. Ultrasonographic imaging (axial view) of the medial head of the gastrocnemius muscle during (A) minimum and (B) maximum compression. G: gastrocnemius muscle, S: soleus muscle.
BoNT-A was delivered to both medial and lateral heads of the gastrocnemius muscle with a ratio of 50%. Injections were performed while the patient was in supine position and the knee in 90º flexion. Physical examination (passive ankle plantar and dorsiflexion) was used as guidance for injections.
All clinical and ultrasonographic evaluations were performed initially before BoNT-A injection and repeated on day 10 and after 2 months.
Statistical analyses
Data were analysed using SPSS 16.0. Descriptive statistics are given as mean (SD) and quantities. Wilcoxon signed-rank test was used for comparison of measurements (baseline, day 10 and month 2). Differences between the paretic and healthy lower limbs were assessed with a Mann-Whitney U test. Spearman’s rank correlation coefficient was used to discover the strength of an association between 2 sets of data. The level of significance was set at p < 0.05.
RESULTS
Mean duration after stroke onset was 861 (SD 1237) (range 67–5,761) days. Mean weight (kg) and height (cm) of the patients were 70.2 (SD 10.4) and 166.7 (SD 6.9), respectively. Twenty-two patients had ischaemic and 4 had haemorrhagic type of stroke. A mean of 128.46 (SD 24.28) (100–150) units of BoNT-A was used. Mean MAS scores decreased from 2.65 (SD 0.56) to 1.61 (SD 0.69) 2 months after treatment (p < 0.001).
On the hemiplegic sides, anterior pennation angle, muscle thickness and leg circumference decreased (p = 0.014, p = 0.010, p = 0.014, respectively), fascicle length increased (p = 0.025) and muscle compressibility did not change on the second month of treatment compared with baseline values (Table I). All of these parameters were statistically similar between baseline and day 10 measurements. Moreover, no significant differences were observed concerning the unaffected side either on day 10 or after 2 months.
| Table I. Ultrasonographic findings of the patients |
| | Healthy side | | Hemiplegic side | | Healthy side vs hemiplegic side |
| Mean (SD) | p | | Mean (SD) | p | | p |
| Anterior pennation angle, degree | |
| Baseline | 21.53 (1.88) | | | 21.26 (1.30) | | | 0.297 |
| 10 days post-treatment | 21.60 (2.20) | 0.262a | | 21.26 (1.19) | 0.962a | | 0.321 |
| 2 months post-treatment | 21.59 (2.14) | 0.586b | | 20.94 (1.57) | 0.014b | | 0.024 |
| Muscle thickness, mm | |
| Baseline | 15.55 (2.54) | | | 14.76 (2.40) | | | 0.313 |
| 10 days post-treatment | 15.35 (2.32) | 0.234a | | 14.60 (2.20) | 0.104a | | 0.247 |
| 2 months post-treatment | 15.58 (2.39) | 0.612b | | 14.43 (2.22) | 0.010b | | 0.065 |
| Fascicle length, mm |
| Baseline | 48.94 (4.35) | | | 39.86 (4.84) | | | <0.001 |
| 10 days post-treatment | 48.50 (3.98) | 0.138a | | 39.98 (4.98) | 0.530a | | <0.001 |
| 2 months post-treatment | 49.25 (4.18) | 0.201b | | 40.20 (4.75) | 0.025b | | <0.001 |
| Muscle compressibility, % |
| Baseline | 37.97 (8.52) | | | 24.77 (8.99) | | | <0.001 |
| 10 days post-treatment | 38.24 (9.94) | 0.948a | | 24.68 (9.71) | 0.821a | | 0.001 |
| 2 months post-treatment | 39.13 (8.68) | 0.073b | | 24.60 (10.01) | 0.841b | | <0.001 |
| aBaseline vs 10 days post-treatment; bbaseline vs 2 months post-treatment. SD: Standard deviation. |
Compared with the unaffected sides, the hemiplegic sides had similar angles of anterior pennation at baseline and on day 10 (p > 0.05), but smaller angles after 2 months of BoNT-A injection (p = 0.024). Values pertaining to fascicle length and muscle compressibility of the hemiplegic sides were significantly smaller than the unaffected sides at baseline, day 10 and month 2 (all p < 0.001). Muscle thickness and leg circumference values were similar between sides at any time of measurement (all p > 0.05). Duration after stroke onset was positively correlated with unaffected side muscle thickness, and negatively correlated with hemiplegic side anterior pennation angle and muscle compressibility (r=0.494, p = 0.010; r = –0.497, p = 0.011 and r = –0.760, p = 0.000, respectively). However, duration after stroke onset was not correlated with any of the ultrasonography measurements on either day 10 or 2 months after treatment (all p > 0.05).
DISCUSSION
This study describes the effects of BoNT-A on muscle architecture in stroke patients. The findings revealed that muscle thickness and anterior pennation angle decreased, and fascicle length increased 2 months after BoNT-A injection.
Although muscle atrophy after BoNT-A injection was reported in some studies, none of them have evaluated changes with respect to anterior pennation angle and fascicle length which, per se, have association with muscle tension/length and eventual joint contractures (10–12). Furthermore, those studies used magnetic resonance imaging, or muscle biopsy, which are quite expensive and inconvenient methods. Our study have used MSUS to evaluate the muscle structure in vivo. Yet, it has been shown previously that MSUS is a potentially useful tool to quantify certain parameters of the skeletal muscle (13, 14). Given its several advantages, MSUS is convenient for physicians to perform and is easily accepted by their patients (15, 16). Likewise, it has also been used for imaging of the spastic muscle architecture in stroke patients (1, 2, 17). Compared with healthy controls, Gao et al. (1) have reported smaller pennation angles, shortened fascicle length and thinner muscle thickness in chronic stroke survivors. Although baseline fascicle length values for our patients were also found to be shortened on the hemiplegic sides, anterior pennation angle and muscle thickness values were similar on both sides of our patients. We believe that the latter disparity could stem from the difference between the durations after stroke onset in the two studies. Yet, Gao et al. included chronic patients who had at least one year duration after stroke onset (1). However, 12 (46.1%) of our patients had less than one year history of stroke, and in most of those patients increased muscle thickness and anterior pennation angle were observed.
In the current study, we additionally used “muscle compressibility” as a new sonographic parameter in order to evaluate muscle elasticity, which is known to be negatively affected in spastic muscles (18, 19). Our findings showed that compressibility of the gastrocnemius muscle was significantly impaired either before or after BoNT-A injection. Moreover, compressibility displayed negative correlations with duration after stroke onset; indicating decreased muscle elasticity in chronic stroke survivors. Another finding of our study was the positive correlation between healthy side muscle thickness and duration after stroke onset. This may be due to the relative overuse of the unaffected lower limb during the interim.
The present study has some limitations, primarily the lack of control group receiving placebo injection. Addition limitations are the lack of long-term follow-up and blinding. Nevertheless, our results appear to be significant.
In conclusion, muscle thickness and anterior pennation angle decrease, but fascicle length increases after BoNT-A injection in stroke patients. Long-term effects of BoNT-A, i.e. the exact timing for disappearance of the toxin effects or evaluation of the effects of repeat injections, remain to be deciphered in further studies. The use of MSUS would be particularly noteworthy in this regard.
The authors declare no conflicts of interest.
REFERENCES